
Abstract
Background:
Early assessment of response to Impella in cardiogenic shock may guide escalation of mechanical circulatory support. Therapeutic goal and response to Impella have not previously been defined. This study tested the hypothesis that targeting 3-h post- Impella cardiac power output index (CPOi)—“hemodynamic response”—in cardiogenic shock is associated with 12-h lactate clearance.
Methods:
Single-center study of 37 consecutive patients who underwent left-sided Impella support for cardiogenic shock due to either acute myocardial infarction or decompensated heart failure. Patients who achieved 3-h post-Impella CPOi ⩾ 0.30 W/m2 were defined as Impella “hemodynamic responder.”
Results:
Twelve of the thirty-seven patients achieved 3-h post-impella CPOi ⩾ 0.30 W/m2 (“hemodynamic responders”). Post-Impella CPOi correlated with 12-h lactate (r = −0.779, p < 0.001) and lactate clearance (r = 0.747, p < 0.001). “Hemodynamic responders” had lower 12-h lactate level and greater 12-h lactate clearance (52 (44–58) vs 17 (14–26)%, p < 0.001). Higher pre-Impella norepinephrine dose (−0.341, p = 0.003) and baseline lactate (−0.009, p = 0.003) were independently associated with lower 3-h post-Impella CPOi. Eighteen patients died within 30 days (2/12 “hemodynamic responders” compared to 16/25 “non-responders,” p < 0.001).
Conclusion:
Patients who achieved early 3-h post-Impella CPOi of ⩾0.30 W/m2 have greater lactate clearance and better short-term survival. Early post-Impella CPOi of 0.30 W/m2 may be used as a therapeutic goal and define favorable response to Impella in cardiogenic shock.
Goal-directed therapy is a well-established therapeutic approach in critical care to guide the use therapeutic interventions such as fluid administration and vasoactive drugs. Impella micro-axial ventricular assist devices are increasingly deployed in cardiogenic shock 1 ; but hemodynamic goals and response to Impella have not been well characterized. Data on early hemodynamic response to Impella would be useful in guiding timely escalation of mechanical circulatory support (MCS) to improve clinical outcomes. Indeed, Tongers et al. showed that early escalation of MCS resulted in greater 12-h lactate clearance, which was associated with better outcomes in cardiogenic shock, 2 highlighting the need for early assessment of hemodynamic response to MCS.
Circulatory failure is the defining feature of shock states, irrespective of the underlying etiology or phenotype. Cardiac power output index (CPOi), the product of cardiac index (CI) and perfusion pressure (difference between mean arterial pressure (MAP) and central venous pressure (CVP)) 3 describes the interaction between the hydraulic work performed by the heart and “vascular function.” Thus, circulatory shock, whether cardiogenic, hypovolemic, obstructive or distributive in origin would result in reduced CPOi. Similarly, failure to reverse circulatory shock would be reflected by a persistently low CPOi.
At our institution, we adopted CPOi of ⩾0.30 W/m2 as a treatment goal in cardiogenic shock, and patients who achieved this treatment goal following Impella support were defined as Impella “hemodynamic responders.” The aim of this study was to determine if “hemodynamic responders” was associated with lower 12-h lactate and greater lactate clearance; hypothesizing that Impella “hemodynamic responders” (3-h post-Impella CPOi of ⩾0.30 W/m2) was associated with lower 12-h lactate level and higher 12-h lactate clearance in patients with cardiogenic shock.
Methods
This is a single-center retrospective analysis of prospectively collected data of consecutive patients from January 2014 to September 2021. Inclusion criteria were: left-sided Impella support for cardiogenic shock due to either acute myocardial infarction or decompensated heart failure. Exclusion criteria were: Impella use to support high risk intervention, Impella combined with VA ECMO or right ventricular assist device at the outset and incomplete hemodynamic data. During this study period, 107 patients underwent Impella support. A total of 70 patients were excluded: high-risk cardiac interventions (n = 29); combined with VA ECMO or right ventricular assist device (n = 26); or incomplete hemodynamic data (n = 15). Thirty-seven patients were included in this retrospective study. This study has institutional approval as part of clinical governance as described previously. 4
Baseline hemodynamic data and lactate were collected within an hour before Impella insertion. Cardiac power output index was calculated as (MAP-CVP) × CI/451 as previously described. The hemodynamic goal of Impella support was to achieve CPOi of ⩾0.30 W/m2. Patients who achieved ⩾0.30 W/m2 on Impella support were defined as “hemodynamic responder.” The rationale for this hemodynamic goal was as follows:
(1). Oxygen delivery (DO2) is calculated as (1.34 × Hb × SataO2) × CI; where Hb = haemoglobin; SataO2 = arterial oxygen saturation.
(2). In cardiogenic shock, a DO2 of at least three times that of oxygen consumption has been recommended 5 ; oxygen consumption in critically ill patients 6 has been estimated at about 100 ml/min/m2. Assuming Hb 100 g/L, to achieve DO2 ⩾300 ml/min/m2 would require CI of ⩾2.23 L/min/m2.
(3). A perfusion pressure (MAP-CVP) ⩾60 mmHg has been recommended.7,8
(4). Based on a MAP-CVP of 60 mmHg and CI of 2.23 L/min/m2, the minimum CPOi target for the treatment of cardiogenic shock can be determined for CPOi: 60 × 2.23/451 = 0.297 W/m2, or rounded up to 0.30 W/m2.
Therefore, we adopted 3-h post-Impella CPOi ⩾0.30 W/m2 as a treatment goal in cardiogenic shock and defined Impella “hemodynamic responder” accordingly. The 3-h time point was selected to allow optimization of Impella and vasopressor/inotrope support. Of note, our CPOi criterion differed from that described in the SHOCK trial. 9 The latter utilized an incomplete equation for the calculation of cardiac power output (CVP excluded from the calculation) and as such, we felt it was inadequate as a therapeutic goal. 3 Indeed, a recent study reported poorer prognostic performance compared to the cardiac power calculation used in this study (CVP included in the calculation). 10 All cardiac output studies were derived from thermodilution studies using pulmonary artery catheters. Vasoactive inotrope score (VIS) 11 was calculated as the sum of Dopamine (in mcg/kg/min) + Dobutamine (in mcg/kg/min) + 100 × epinephrine (in mcg/kg/min) + 100 × norepinephrine (in mcg/kg/min) + 10 × milrinone (in mcg/kg/min) + 10000 × vasopressin (in U/kg/min).
The primary outcomes of interest are 12-h lactate and lactate clearance. Lactate clearance was calculated as difference between baseline and 12-h lactate divided by baseline lactate. The association between hemodynamic response and 30-day mortality was assessed as an exploratory secondary outcome of interest.
Statistical analysis
Data were presented as mean ± standard deviation or median (interquartile range) for parametric and non-parametric data respectively. The Shapiro-Wilk test for was used to test for normality. Differences between groups were tested using t test or Mann Whitney U test for parametric and non-parametric data respectively. Fisher’s exact test was used for categorical data. Serial changes were assessed by paired t test; or signed rank test. Multivariable regression analysis was performed to examine the relationship between 3-h post-Impella CPOi and 12-h lactate level and clearance. p value of <0.05 was considered statistically significant. Statistical analyses were performed on Stata v16.1 (Texas, USA).
Results
Thirty-seven patients were included in this study. Twelve of the 37 patients achieved 3-h post-impella CPOi ⩾0.30 W/m2 (“hemodynamic responders”). Baseline demographics were comparable except for higher ejection fraction and tricuspid annular plane systolic excursion in the “hemodynamic responder” group (Table 1). At baseline, the VIS was higher in non-responders compared to responders (28 ± 5 vs 18 ± 5, p < 0.001), due to higher doses of epinephrine and norepinephrine doses (VIS excluding epinephrine and norepinephrine were comparable: 5 ± 2 vs 6 ± 2, p = 0.085) (Table 2). Despite higher doses or norepinephrine, non-responders had lower systemic vascular resistance index compared to “hemodynamic responders” (1920 ± 297 vs 2125 ± 305 dyne.s.m2/cm−5, p = 0.048). Baseline norepinephrine dose did not correlated with baseline lactate (p = 0.133) (Data supplement). Baseline CPOi were comparable between Impella “hemodynamic responders” compared to “non-responders.”
Baseline patient characteristics.
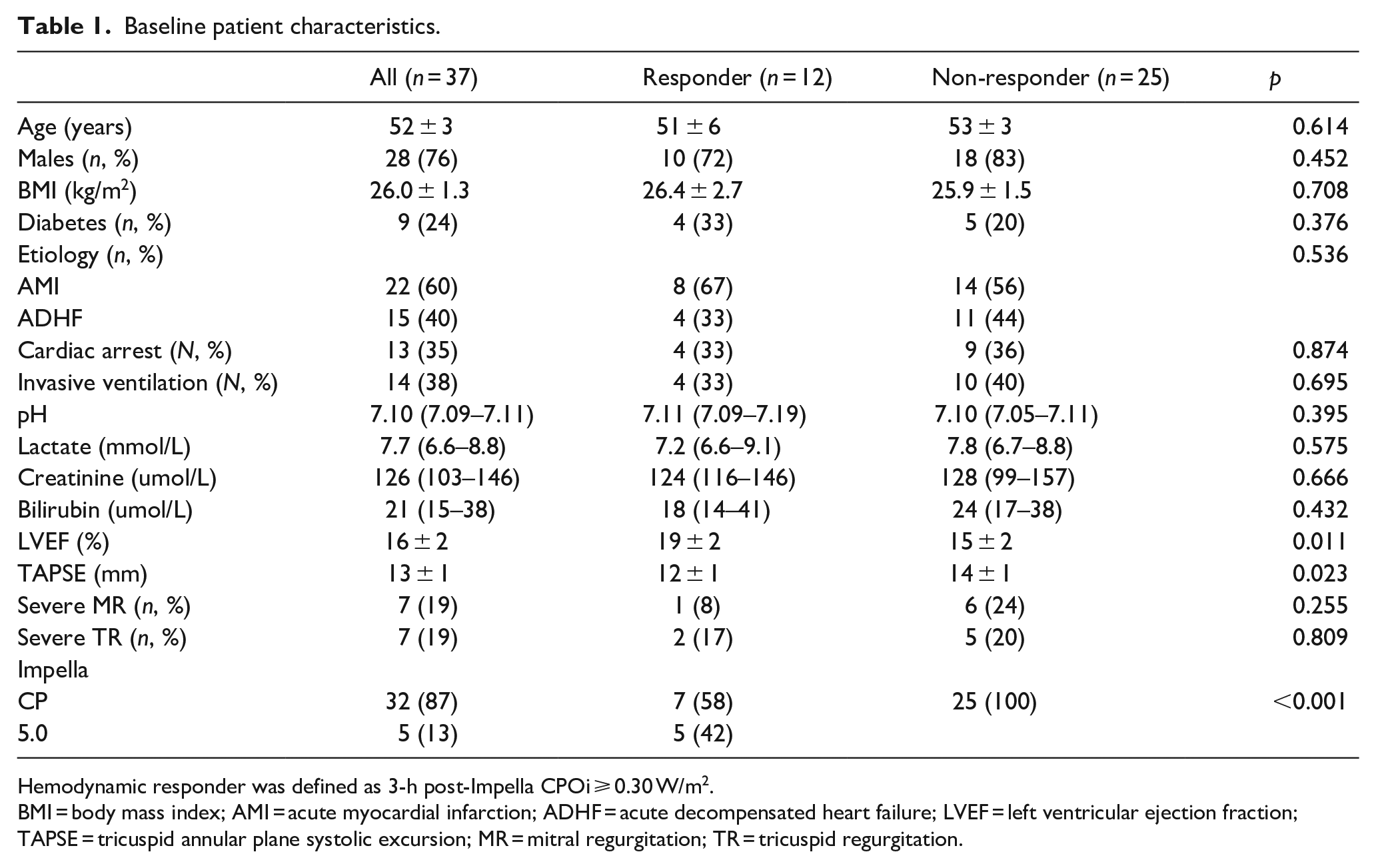
Hemodynamic responder was defined as 3-h post-Impella CPOi ⩾ 0.30 W/m2.
BMI = body mass index; AMI = acute myocardial infarction; ADHF = acute decompensated heart failure; LVEF = left ventricular ejection fraction; TAPSE = tricuspid annular plane systolic excursion; MR = mitral regurgitation; TR = tricuspid regurgitation.
Baseline and post-Impella hemodynamic parameters.
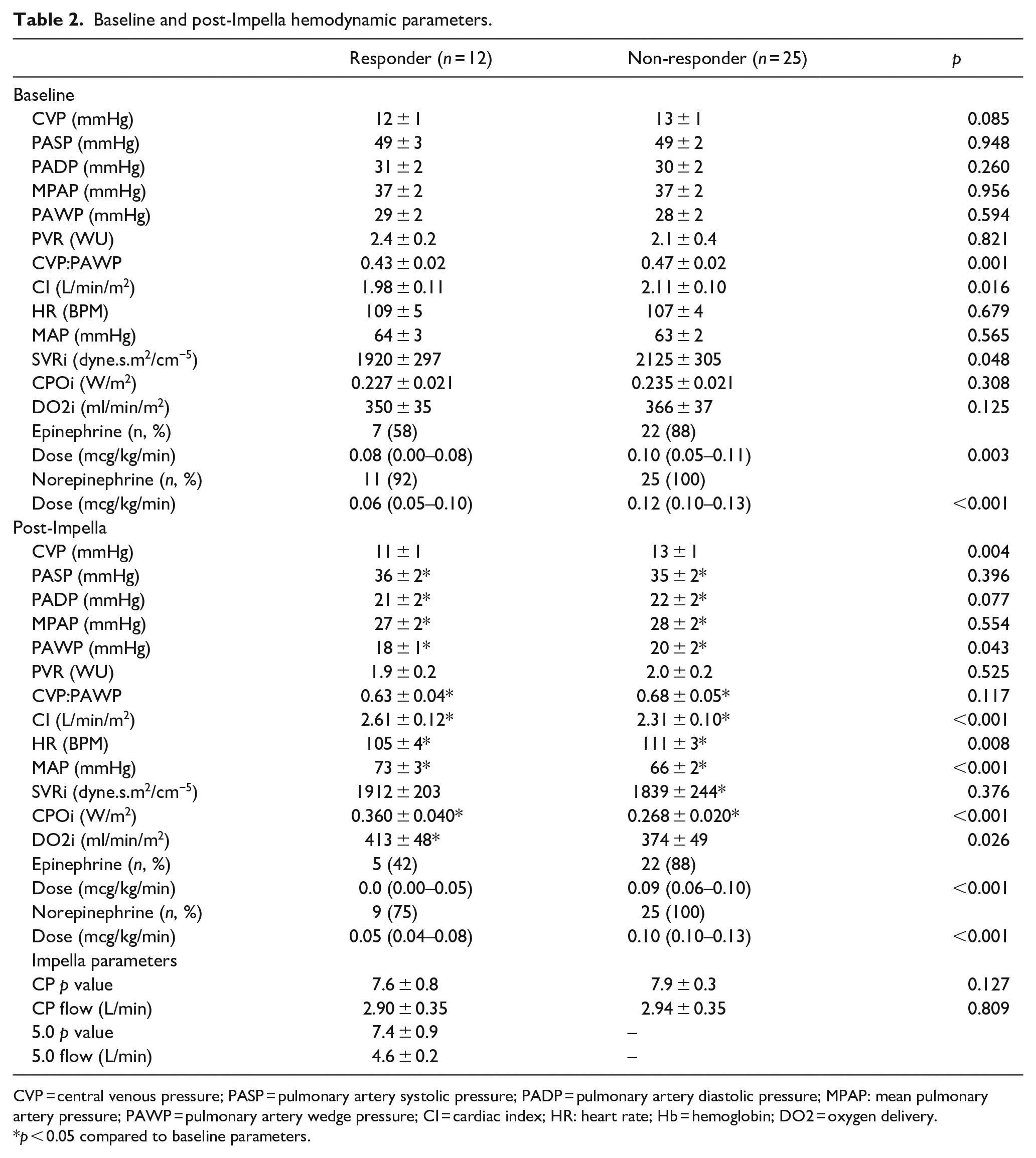
CVP = central venous pressure; PASP = pulmonary artery systolic pressure; PADP = pulmonary artery diastolic pressure; MPAP: mean pulmonary artery pressure; PAWP = pulmonary artery wedge pressure; CI = cardiac index; HR: heart rate; Hb = hemoglobin; DO2 = oxygen delivery.
p < 0.05 compared to baseline parameters.
Pulmonary artery pressures reduced significantly in both groups at 3-h post-Impella due to reduction in pulmonary artery wedge pressures (Table 2). The p value settings of Impella CP and 5.0 were 7.8 ± 0.5 and 7.4 ± 0.9, respectively. CPOi increased in “hemodynamic responders” and “non-responders” due to increase in MAP and CI. Post-Impella CPOi correlated with 12-h lactate (r = −0.779, p < 0.001) and lactate clearance (r = 0.747, p < 0.001). “Hemodynamic responders” had significantly lower 12-h lactate level and greater 12-h lactate clearance (Figure 1(a) and (b)). On linear regression analysis (including norepinephrine, epinephrine doses, baseline lactate, baseline mean arterial blood pressure, TAPSE, ejection fraction and Impella CP use), higher pre-Impella norepinephrine dose (−0.341, 95% CI: −0.556 to −0.127, p = 0.003) and baseline lactate (−0.009, 95% CI: −0.014 to −0.003, p = 0.003) were associated with lower 3-h post-Impella CPOi.
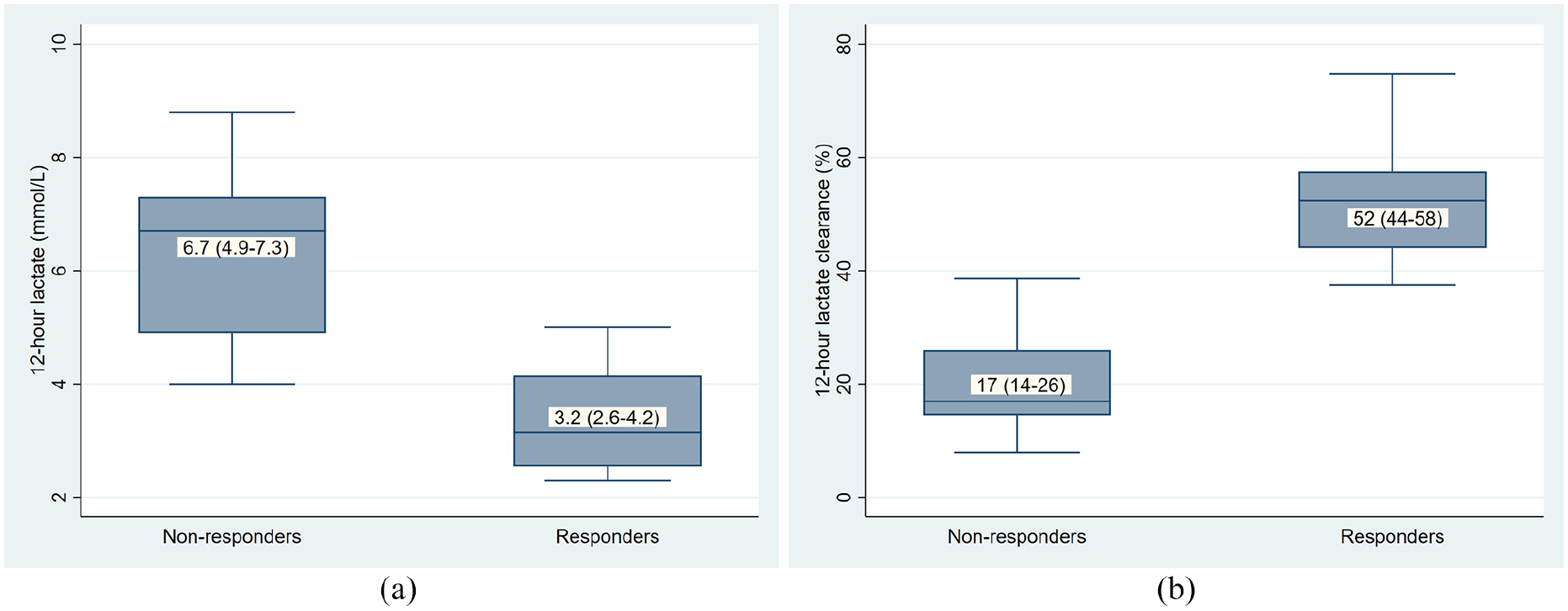
(a) 12-hlactate levels in Impella hemodynamic responders (3-h post-Impella CPOi ⩾ 0.30 W/m2) and non-responders (3-h post-Impella CPOi < 0.30 W/m2) (p < 0.001).
Pre-Impella norepinephrine dose of >0.10 mcg/kg/min was associated with 96% sensitivity and 67% specificity for non-response to Impella (Figure 2). None of the “hemodynamic responders” underwent MCS escalation compared to 16/25 “non-responders” (p < 0.001) who underwent additional veno-arterial extracorporeal membrane oxygenation support. Eighteen patients died within 30 days, with a greater proportion in non-responders (p < 0.001) (Figure 3). Nine of the 16 “non-responders” who underwent escalation died at 30 days.
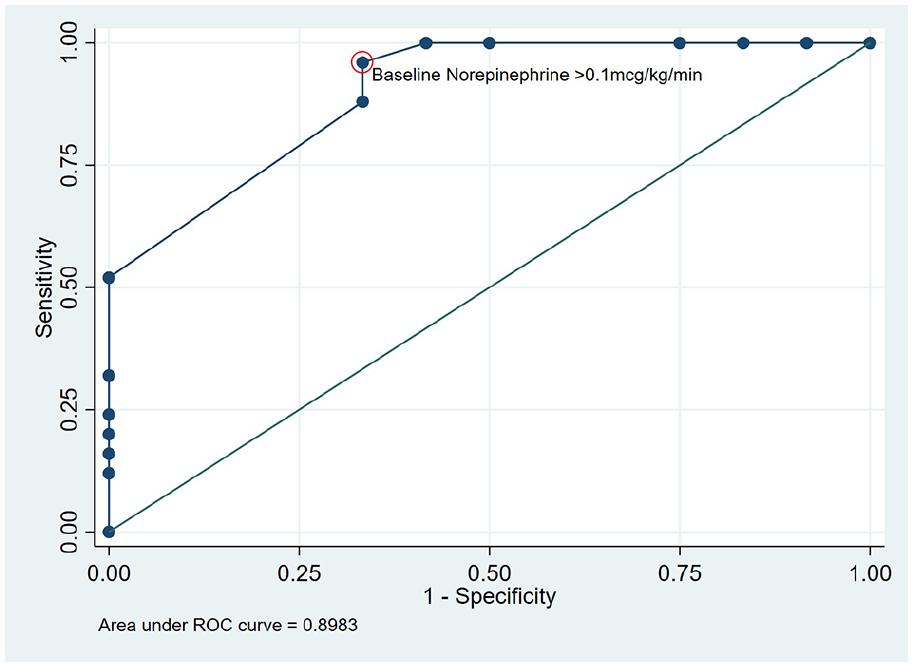
Receiver operating characteristic curve of baseline norepinephrine dose in discriminating between Impella response versus non-response. The circled point represents baseline norepinephrine dose of >0.10 mcg/kg/min, which was associated with 96% sensitivity and 67% specificity for non-response to Impella (post-Impella CPOi <0.30 W/m2).
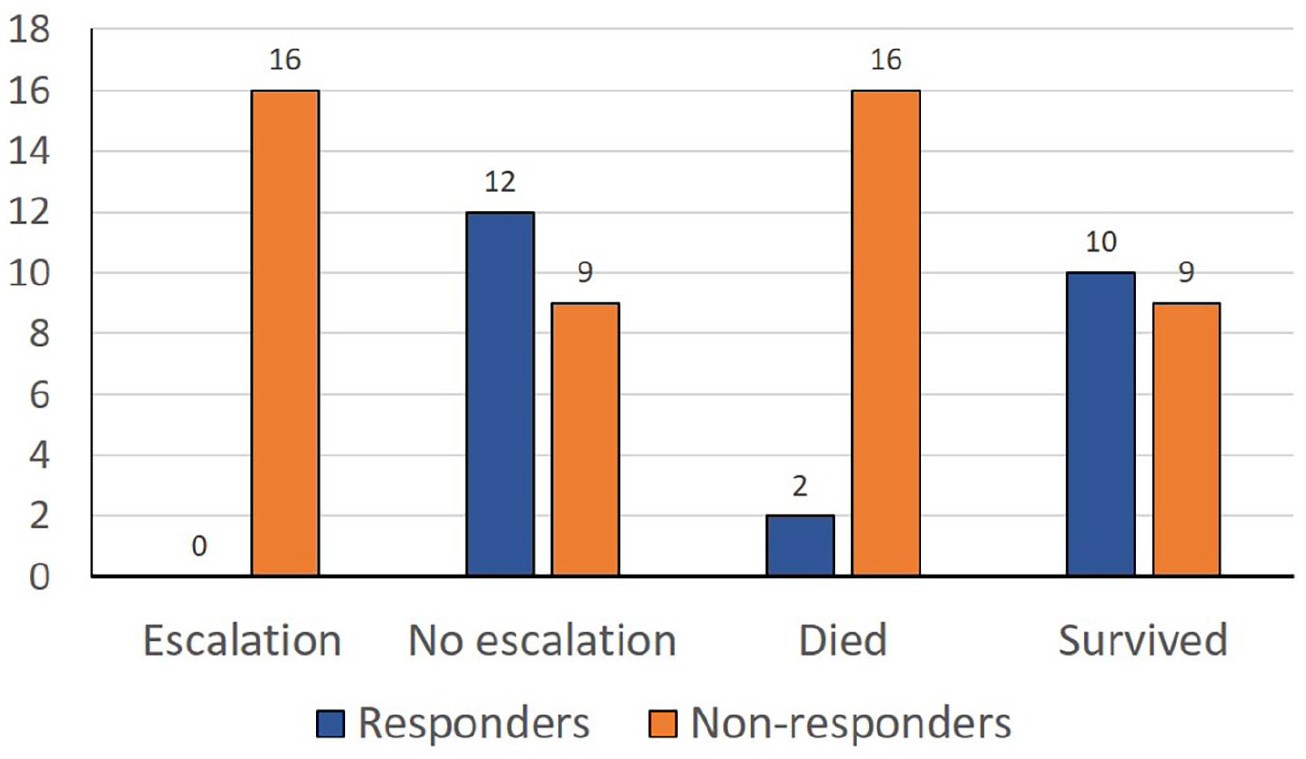
Escalation of MCS and 30-day mortality in hemodynamic responders and non-responders.
Discussion
It is common to define response to therapy in cardiovascular medicine. In all cases, the defining parameter and its cut-off should be measurable, responsive to the therapeutic intervention and relevant to the outcome of interest. The parameter of CPOi fulfils these criteria. We adopted CPOi to define response to Impella and the current data suggest that 3-h post-Impella CPOi of ⩾0.30 W/m2 was associated with lower 12-h lactate, greater lactate clearance and lower 30-day mortality.
One of the defining features of circulatory shock is the failure of DO2 and oxygen utilization. Indeed, DO2 has been long been advocated as the therapeutic target of VA ECMO support—“to maintain systemic oxygen delivery at least three times oxygen consumption.” 5 Historically, DO2 is calculated as the product blood oxygen content and cardiac output. Although this DO2 calculation describes the total oxygen delivery, “effective” DO2 is dependent on (regional) vasomotor tone to maintain perfusion pressure, epitomized by the autoregulatory mechanisms to maintain blood flow and oxygen delivery to vital organs. In practice, mean arterial blood pressure is used as a simple surrogate for perfusion pressure. At any given vascular tone, the heart supplies hydraulic energy to maintain the pressure within the circulation; this rate of energy output is termed CPOi. Thus, increases in both DO2 and CPOi are necessary for an increase in “effective” oxygen delivery in circulatory shock. Indeed, hemodynamic responders were characterized by both an increase in DO2 and CPOi.
CPOi calculation in its current iteration uses MAP instead of the mean systolic pressure. This subtle substitution is a pragmatic one, as it is not clinically practical to integrate systolic pressure. However, somewhat serendipitously, the use of MAP takes into consideration diastolic blood pressure, which is largely influenced by “vascular function”—both the resistance vessels and the capacitance of the aorta (windkessel model). Thus, by using MAP, we are inadvertently describing the state of the circulation, and not “cardiac function per se.” CPOi is responsive to Impella support. Increased left ventricular unloading/output, consequent improvement in right heart function through series and parallel ventricular interaction and in the absence of any changes in “vascular function” would be expected to increase CPOi. Norepinephrine dose is a surrogate index of poor “vascular function” (i.e. combined distributive and cardiogenic shock phenotype), as the dose is typically titrated to achieve a target MAP. Indeed, systemic vascular resistance index was lower in non-responders at baseline despite higher norepinephrine doses, indicative of a distributive component to the circulatory shock in the majority of non-responders. These data suggest that “vascular failure” (high norepinephrine requirement) in association with more severe circulatory shock (higher lactate) cannot be adequately overcome by Impella CP support alone.
CPOi is also prognostically relevant. 12 In this study, post-Impella CPOi is related to 12-h lactate clearance, which is linked to short-term survival in the critical care setting 13 and in cardiogenic shock.2,14 Thus, 12-h lactate and lactate clearance are useful measures of response to treatment. However, despite its undoubted clinical value, 12-h lactate is by definition a relatively late measure of response, and early appreciation of inadequate response would allow optimization or escalation of support. Thus, early CPOi assessment at 3 h (“hemodynamic response”) complements 12-h lactate level measurement in assessing response to Impella in cardiogenic shock. The relationship with clinical outcomes in this study is of interest but exploratory at this stage in view of the small cohort.
This study has a number of limitations. Firstly, this study is susceptible to biases as a single center observational study, especially with the small size of the patient cohort (n = 37). Secondly, only a small number of patients were supported with Impella 5.0 and no clear conclusion regarding could be made regarding response to different Impella devices. Thirdly, this study did not evaluate a CPOi-guided MCS strategy on clinical outcomes in cardiogenic shock. Thus, these findings should be considered hypothesis-generating and will need to be confirmed in future studies.
In conclusion, early 3-h post-Impella CPOi of ⩾0.30 W/m2 may be used to define favorable response to Impella. Early post-Impella CPOi of <0.30 W/m2 is associated with poor 12-h lactate clearance, need for subsequent escalation of MCS and higher 30-day mortality.
Supplemental Material
sj-tif-1-jao-10.1177_03913988221100278 – Supplemental material for Cardiac power output index to define hemodynamic response to Impella support in cardiogenic shock
Supplemental material, sj-tif-1-jao-10.1177_03913988221100278 for Cardiac power output index to define hemodynamic response to Impella support in cardiogenic shock by Hoong Sern Lim in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Honoraria from Abiomed.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.