
Abstract
Atrial septostomy has been the last resort in the management of patients with the right ventricular failure related to pulmonary hypertension before lung transplantation. In this paper, we present a simple and safe technique (transatrial approach) for balloon atrial septostomy in a patient who required central venoarterial extracorporeal membrane oxygenation after pulmonary endarterectomy.
Keywords
Case
A 28-year-old woman was referred for pulmonary endarterectomy (PEA) due to chronic thromboembolic pulmonary hypertension (CTEPH). In past medical history, she had an implanted port which was placed into superior vena cava and experienced repeated episodes of deep venous thrombosis during the course of chemotherapy for ovarian cancer. Physical examination and routine laboratory tests were within the normal range. Oxygen saturation was 82% while breathing ambient air. Chest computed tomography revealed bilateral pleural effusion, enlarged pulmonary arteries with chronic occlusion of the segmental and subsegmental branches (Figure 1(a)). Lung ventilation/perfusion scan showed multiple mismatched perfusion defects in both lobes lungs (Figure 1(a)). She was referred for PEA after anticoagulation with warfarin for 1 year.
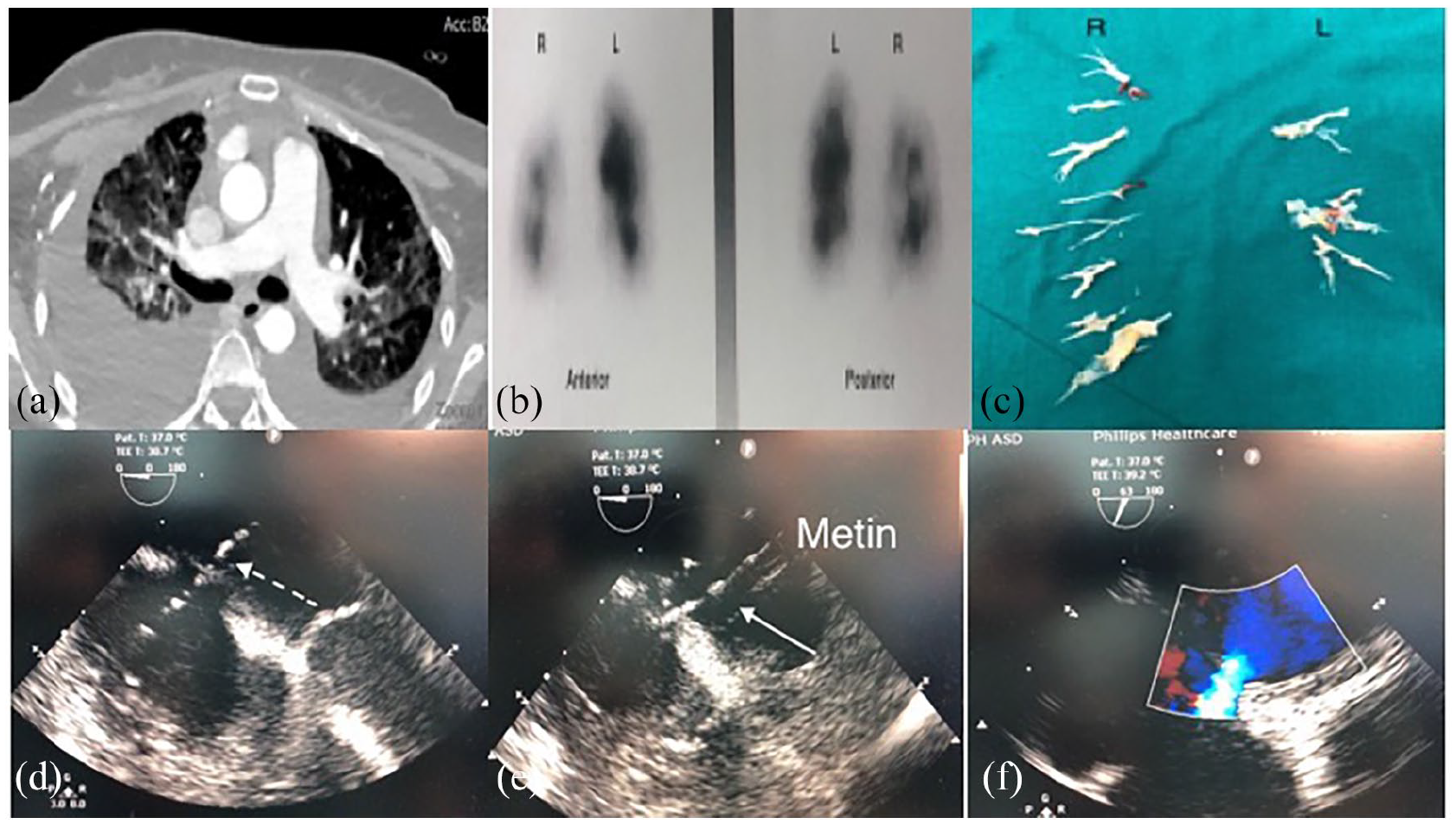
(a) Preoperative pulmonary computed tomography angiography, (b) Ventilation/Perfusion scan, (c) Endarterectomy material, (d) Intraoperative transthoracic echocardiography showing the guidewire through the interatrial septum (dotted arrow), (e) Inflated balloon for septostomy (arrow), and (f) Bidirectional shunting through the septum after septostomy.
Transthoracic echocardiography revealed a severe right ventricular (RV) dysfunction and peak tricuspid regurgitant velocity of 4.2 m/s. Her 6-min walk distance was 177 m. Right heart catheterization revealed a mean pulmonary arterial (PA) pressure of 51 mmHg (83/26), PA wedge pressure of 9 mmHg, pulmonary vascular resistance of 14.93 wood units, and mean right atrial (RA) pressure of 16 mmHg.
Bilateral PEA was performed under deep hypothermia (20°C) and intermittent circulatory arrest. Intraoperatively, pulmonary pathology was consistent with the distal type of involvement (Figure 1(c)). After being weaned off cardiopulmonary bypass (CPB) with vasoactive drugs and inhaled nitric oxide, the patient was hemodynamically unstable and severely hypoxemic. Despite an apparently successful PEA, systolic PA pressure was almost systemic at 95–100 mmHg and RV contraction severely depressed. CPB was resumed, and a central venoarterial extracorporeal membrane oxygenation (VA-ECMO) was instituted. The arterial and venous cannulae were tunneled subcutaneously and sternum was closed in a regular fashion. After 2 days of stable ECMO run, the flow had been reduced in a stepwise manner. On postoperative day 5, the patient was weaned off ECMO with the eventual flow of 800 ml/min, she experienced a rapid hemodynamic deterioration and RV dysfunction on bedside echocardiogram. Repeated trials of weaning had remained unsuccessful. The decision for transatrial balloon atrial septostomy (BAS) in the operating theater was given. After reopening of the sternum and putting a purse string suture to the lateral wall of the RA, a needle was passed through the RA and the interatrial septum (IAS) is punctured under transesophageal echocardiography (TEE) guidance. Then, a guidewire was passed through the IAS (Figure 1(d)). A 8 mm × 50 mm peripheral angioplasty balloon (Boston Scientific) was used for atrial septostomy (Figure 1(e)). A 6–7 mm defect was created with bidirectional shunting (Figure 1(f)). The VA-ECMO was weaned without decannulation. The leftward bulging of the IAS was disappeared immediately and the peak tricuspid regurgitant velocity decreased to 3.7 m/s. A trivial drop was seen in systemic oxygen saturation after transatrial BAS (96%–93% under 40 FiO2%). The RA pressure decreased from 24 mmHg to 14 mmHg almost 30 min after septostomy. After 1 h of watchful waiting, the decision for decannulation and chest closure was given. The postoperative hemodynamics were stable. She underwent tracheostomy to facilitate extubation on postoperative day 13 and discharged from hospital on postoperative day 20.
Comment
Atrial septostomy has been taken into consideration as the last resort for the treatment of RV failure from severe pulmonary arterial hypertension (PAH) before lung transplantation and severe PAH. Its immediate hemodynamic benefits are a significant decrease in RV end-diastolic pressure and an increase in cardiac index about 20%–25%. 1 It has been shown that in selected patients with PAH, BAS is a safe and effective intervention that exerts a beneficial impact on long-term survival, especially when it is combined to PAH-specific pharmacotherapy. 2
After PEA, some patients might have a borderline RV function due to the CBP-related myocardial and pulmonary dysfunction in addition to the long term unfavorable effect of CTEPH on the RV myocardium. In case of severe RV failure after PEA, institution of VA-ECMO is necessary for a while postoperatively. The need for VA-ECMO support after pulmonary endarterectomy (PEA) has been reported in 4%–20% of the cases. While the outcome of VA-ECMO has been reported to be satisfactory, a considerable amount number of patients on VA-ECMO could not be weaned off after PEA. 3 As a rescue procedure, BAS is commonly preferred for decompression of the RA or left atrium (LA) and increasing the mixing at the atrial level in patients with congenital heart defects. In patients under VA-ECMO, it has been claimed that BAS facilitates the weaning off ECMO and better outcome in pediatric patients with myocarditis and pulmonary hypertension.4,5 Baruteau et al. 5 revealed that percutaneous BAS is an efficient approach for decompressing the LA in patients with end stage LV failure supported by VA-ECMO. They reported an immediate reduction of both the mean LA pressure and LA-RA pressure gradient from 24.2 ± 6.9 mmHg to 7.8 ± 2.6 mmHg and 17.2 ± 7.1 mmHg to 0.09 ± 0.5 mmHg, respectively.
Herein, we present an alternative and simple technique of transatrial BAS before weaning in a patient who underwent PEA and required VA-ECMO immediately after CPB. In our institution, central ECMO is preferred over peripheral ECMO in both post-cardiotomy and post-endarterectomy patients as it precludes the potential disadvantages of peripheral cannulation like limb ischemia and need for doing extra punctures or incisions in already anticoagulated patients. Deep sternal infection or mediastinitis is shown to be the major disadvantage of central ECMO but it could be minimized via tunneling of all cannulae with sternal closure in our opinion. Although it is underutilized, atrial septostomy could be regarded as a rescue procedure in some patients on VA-ECMO after PEA. 6 Balloon atrial septostomy is routinely performed via percutaneous approach. 7 However, it has been found that BAS for left atrial decompression can be performed without procedural mortality but is associated with significant morbidity. 8 Moreover, presence of the venous cannula in the atrium and delayed sternum closure in these patients might make the peripheral access a bit challenging for cardiologists or interventionists. Our balloon size was apparently smaller than those routinely used in BAS. We preferred using a smaller balloon size for BAS as the patient needed a relatively lower ECMO flow to maintain the proper RV functioning. Therefore, as the estimated volume of the blood to be shunted through the interatrial defect was regarded as low, a small sized balloon was selected. Otherwise, systemic arterial desaturation would complicate the postoperative course of the patient.
Recently application of percutaneous veno-venous ECMO devices like ProtekDuo has gained popularity for effective decompression of the right heart in lung transplantation candidates with acute decompensation. 9 The use of these devices could be a rational approach in patients who had acute RV failure immediately after PEA.
In our opinion, transatrial BAS is a simple and safe alternative to the percutaneous approach in these patients. Its proposed hemodynamic benefits might improve the early outcome after PTE in selected patients with ECMO.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.