
Abstract
Introduction:
Unfractionated heparin is the most commonly utilized anticoagulant in extracorporeal membrane oxygenation (ECMO) due to clinician familiarity, ease of reversal, and low cost compared to alternative agents. However, heparin’s anticoagulant effect can be unpredictable and its use accompanies a risk of heparin induced thrombocytopenia (HIT). Successful use of bivalirudin as an alternative to heparin in non-HIT ECMO patients has previously been described. However, there is a paucity of data regarding its utilization in patients with confirmed HIT on ECMO.
Methods:
This single-center retrospective chart review at Cleveland Clinic Main Campus included 12 ECMO patients who were managed with bivalirudin for a new diagnosis of HIT. Descriptive statistical analyses were performed utilizing median with interquartile range and number with percent as appropriate.
Results:
Of the 12 patients included, median ECMO duration was 328.5 (218.8–502.1) h and venoarterial ECMO was the most common configuration. No patients experienced the primary outcome of in-circuit thrombosis while on bivalirudin. One patient developed a deep vein thrombosis 22.5 h after switching from heparin to bivalirudin. Major bleeding occurred during bivalirudin therapy in 8 (66.7%) patients.
Conclusions:
Overall, our study results suggest that bivalirudin is effective for the management of HIT and did not show evidence of in-circuit thrombosis. A high incidence of major bleeding was observed with bivalirudin use within this study. Clinicians should view bivalirudin as an acceptable agent for the treatment of HIT in the ECMO population, but must consider bleeding risk given the lack of effective reversal agents.
Introduction
Patients requiring extracorporeal membrane oxygenation (ECMO) are often anticoagulated to prevent arterial and venous thromboembolism, as well as in-circuit thrombosis. 1 Due to the foreign nature of the circuit, ECMO induces a complex inflammatory response and subsequent activation of the coagulation cascade. 2 The Extracorporeal Life Support Organization provides anticoagulation guidelines that support anticoagulation with unfractionated heparin for patients on ECMO. 1 Unfractionated heparin is the most frequently utilized anticoagulant in ECMO due to its high familiarity among clinicians, ease of reversal, and low cost compared to alternative agents.1,3 However, heparin’s anticoagulant effect can be unpredictable and its use accompanies a risk of heparin induced thrombocytopenia (HIT).3,4 Patients requiring ECMO commonly experience thrombocytopenia due to platelet shearing, activation, aggregation, and multi-organ dysfunction and clinicians often have concern for HIT.2,5
Patients on ECMO may also be at higher risk to develop HIT than the general population and alternative anticoagulant use is recommended when there is intermediate or high probability for HIT. 6 It has been postulated that ECMO as well as cardiopulmonary bypass circuit-related effects including extensive platelet activation, thrombocytopenia, as well as release of large amounts of platelet factor 4 lead to an increased incidence of HIT. 6 Bivalirudin, a direct thrombin inhibitor that has a strong affinity for free and bound thrombin, predominantly undergoes non-end organ elimination through proteolysis and has been shown to exhibit a more predictable anticoagulant effect than heparin.1,3,7 Additionally, bivalirudin exhibits its anticoagulant effect independent of antithrombin III, which may often be depleted in patients requiring ECMO. 8 Successful use of bivalirudin as an off-label alternative to heparin anticoagulation in non-HIT ECMO patients has previously been described and was associated with less activated partial thromboplastin time (aPTT) variability, greater time within therapeutic aPTT range, and no difference in 7-day thrombosis, bleeding, or mortality.3,9 Additional alternative anticoagulation strategies include argatroban, though clinicians may be weary of its use due to the extended half-life as compared to bivalirudin. However, previous data in the non-HIT ECMO population has found argatroban to be non-inferior to unfractionated heparin in regards to bleeding and thrombosis. 10
There are potential risks to using bivalirudin in this setting, as there are no available pharmacologic antidotes for bivalirudin-related bleeding. In addition, it has been proposed that blood stagnation within the ECMO circuit or native heart may lead to increased bivalirudin degradation and subsequent thrombus formation. 11
Experience with the use of bivalirudin in ECMO patients with suspected and confirmed HIT is limited to a small number of case reports, and the safety and effectiveness of bivalirudin for this patient population has not been fully described.12 –14 The goal of this study was to evaluate the use of bivalirudin in the management of serotonin release assay (SRA) confirmed HIT-positive patients requiring ECMO.
Methods
This was a single-center retrospective, observational study conducted at Cleveland Clinic (Cleveland, OH) and was approved by the Institutional Review Board (IRB #21-074). Patients were identified from January 2015 through February 2020 by screening our institutional ECMO database. Additional patients were included from March to December 2020 by screening all orders for bivalirudin infusions in the electronic medical record. Patients were included in the study if they were at least 18 years of age, supported on either venoarterial (V-A) or venovenous (V-V) ECMO for at least 48 h, treated with bivalirudin for acute HIT while requiring ECMO support, and had a positive SRA result. If an SRA was unavailable, a positive anti-platelet factor-4 IgG enzyme-linked immunosorbent assay (anti-PF4 ELISA) result (optical density >0.4) was used for diagnosis of HIT. All patients were admitted to either the cardiovascular intensive care unit (CVICU) or the coronary care intensive care unit (CICU). Patients with a negative SRA result, those diagnosed with COVID-19 infection, and those receiving prophylactic anticoagulation while on ECMO were excluded from the analysis. For ECMO support, our institution primarily utilizes Rotaflow (Maquet) pumps with Quadrox (Maquet) oxygenators and HLS (Maquet) cannulae (19–29 French). For single-site cannulation, Avalon (Maquet) or Crescent (Medtronic) cannulae are utilized. Softline coating is used preferentially. General ECMO anticoagulation practices at our institution include bolus administration of 50–100 units/kg unfractionated heparin at the time of ECMO cannulation followed by a heparin infusion to maintain an aPTT of 49–67 s (correlating to an anti-factor Xa level of 0.2–0.5 IU/mL). Our institution routinely utilizes measurements of post-oxygenator partial pressures of oxygen (PO2) to assess for adequate gas exchange and oxygenator effectiveness. Upon clinical suspicion for HIT, an anti-PF4 ELISA is sent, vascular medicine is consulted, and the patient may be switched to bivalirudin if the patient is intermediate or high-risk for HIT. Bivalirudin infusions are typically managed by a practitioner from the Department of Vascular Medicine and titrated to target an aPTT of 46–65 s.
Clinical and demographic data were extracted from the electronic medical record. The primary objective was to describe the rate of new in-circuit thrombosis in patients managed on bivalirudin for the treatment of HIT in patients requiring ECMO. In-circuit thrombosis was defined as a documented thrombus within the ECMO cannulas or oxygenator that required oxygenator or circuit exchange. Secondary objectives were to describe the rate of major bleeding in ECMO patients on bivalirudin for HIT, to describe the percentage of time maintained on bivalirudin within the defined therapeutic aPTT target range, and to characterize risk factors associated with HIT in patients requiring ECMO.
Major bleeding was defined by ELSO criteria as clinically overt bleeding associated with a hemoglobin fall of at least 2 g/dL in a 24 h period, greater than 20 mL/kg blood loss over a 24 h period, a transfusion requirement of one or more 10 mL/kg packed red blood cells (PRBC) over a 24 h time period, or bleeding that is retroperitoneal, pulmonary, involves the central nervous system, or requires surgical intervention. 1 Minor bleeding was also defined by ELSO criteria as bleeding that requires one 10 mL/kg transfusion or less or blood loss ⩽20 mL/kg/day. 1 Minor bleeding was not documented for patients that experienced a major bleeding event. A therapeutic aPTT was defined as an aPTT within the range defined within the bivalirudin order administration instructions. For all patients, the 4T score was documented in the electronic medical record by a Vascular Medicine practitioner at the time of bivalirudin initiation.
Descriptive statistical analyses were performed for continuous variables using median with interquartile range (IQR). Categorical variables were expressed as number (percent). All analyses were performed using StataIC 14 (StataCorp LLC, College Station, TX).
Results
A total of 292 patients were screened for inclusion for this evaluation and 280 patients were excluded (Figure 1). Of the 12 patients included, 10 (83.3%) patients were located in the CVICU and the remainder of patients in the CICU (Table 1). Patients in this study had a median ECMO duration of 328.5 (218.8–502.1) h, V-A ECMO was the most common configuration, and three (25%) patients were concomitantly managed on Impella support. In total, 11 patients had SRA-confirmed HIT and one patient was included by result of anti-PF4 ELISA due to an indeterminate SRA result. The median anti-PF4 optical density in our cohort was 1.37 (0.83–2.0). HIT was diagnosed during the course of ECMO support in ten (83.3%) patients (Table 2). The remaining two (16.7%) patients were both diagnosed within 8 days of ECMO cannulation and were maintained on bivalirudin throughout ECMO support. Of the cohort diagnosed with HIT during ECMO, the median time to anti-PF4 ELISA order from ECMO cannulation was 205.3 (147.8–274) h. In patients diagnosed with HIT while on ECMO support, the documented 4T scoring estimated low probability for HIT in two patients (20%), intermediate probability in four patients (40%), and high probability in four patients (40%). Within this cohort, six (60%) patients had evidence of a thrombotic event prior to anti-PF4 ELISA order. These thrombotic events included three (30%) deep vein thrombosis, two (20%) in-circuit thrombosis, one (10%) Impella cannula thrombosis, and one (10%) arterial thrombosis.
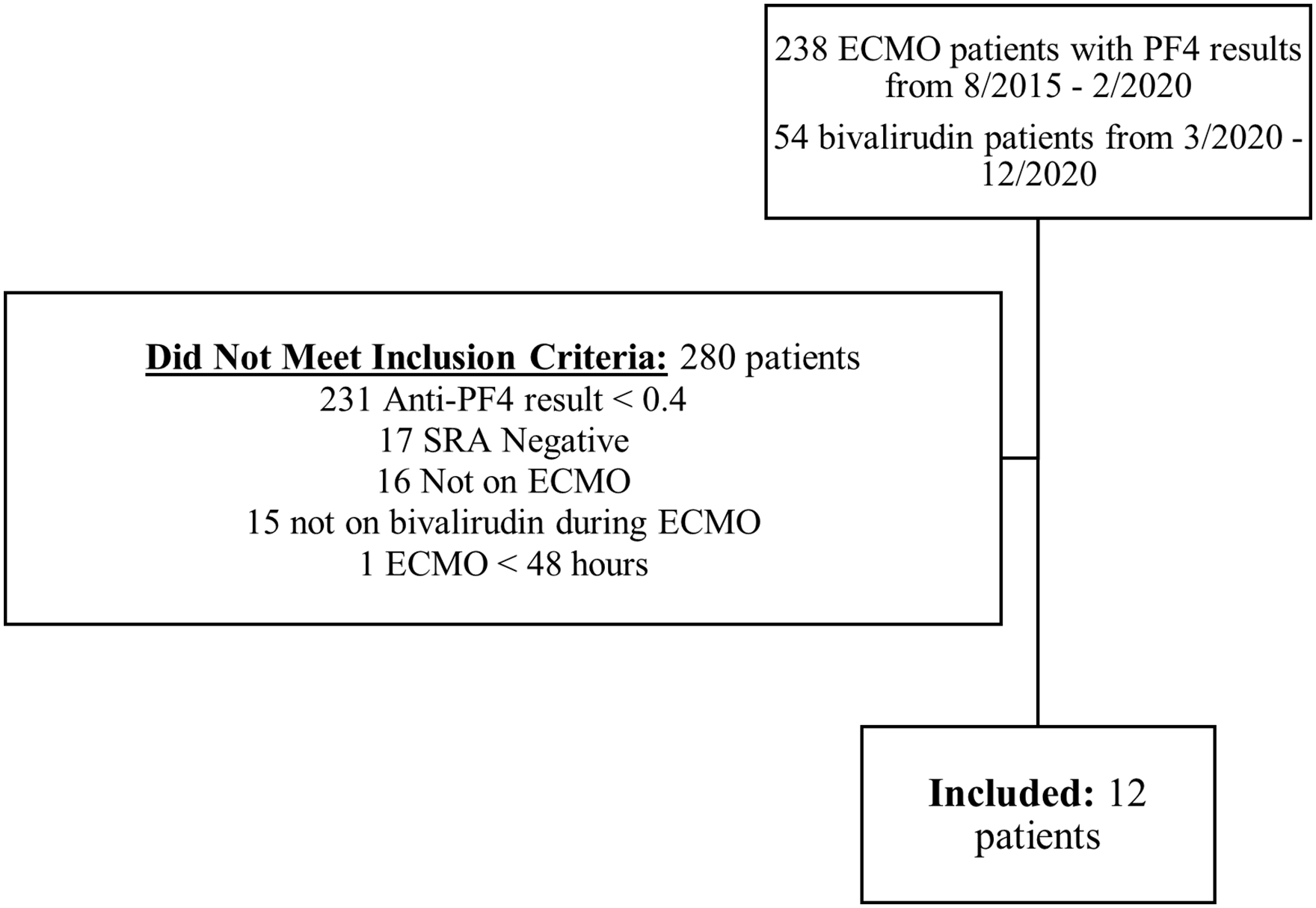
Patient inclusion.
Baseline characteristics.
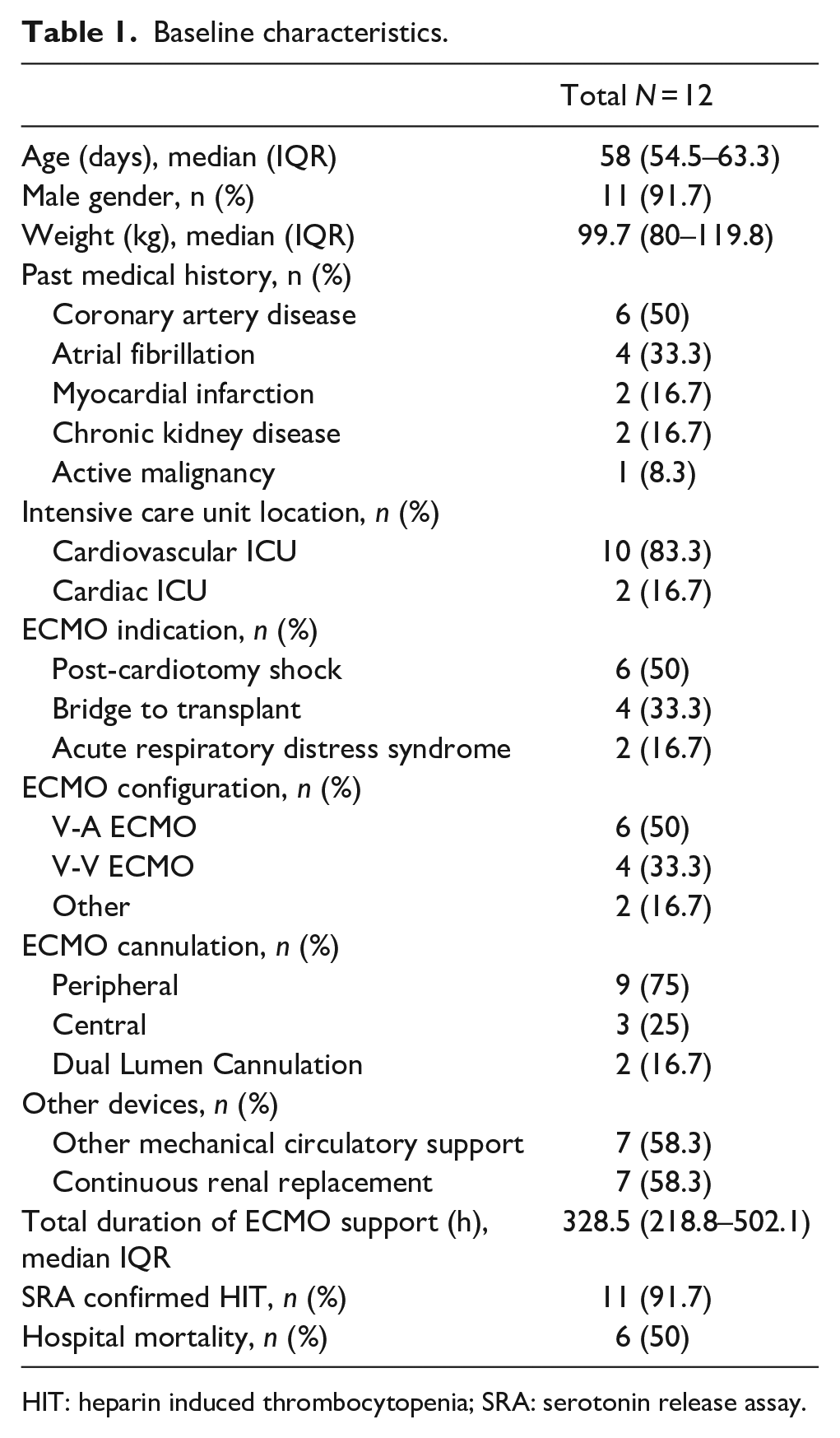
HIT: heparin induced thrombocytopenia; SRA: serotonin release assay.
Heparin induced thrombocytopenia, diagnosed on ECMO.
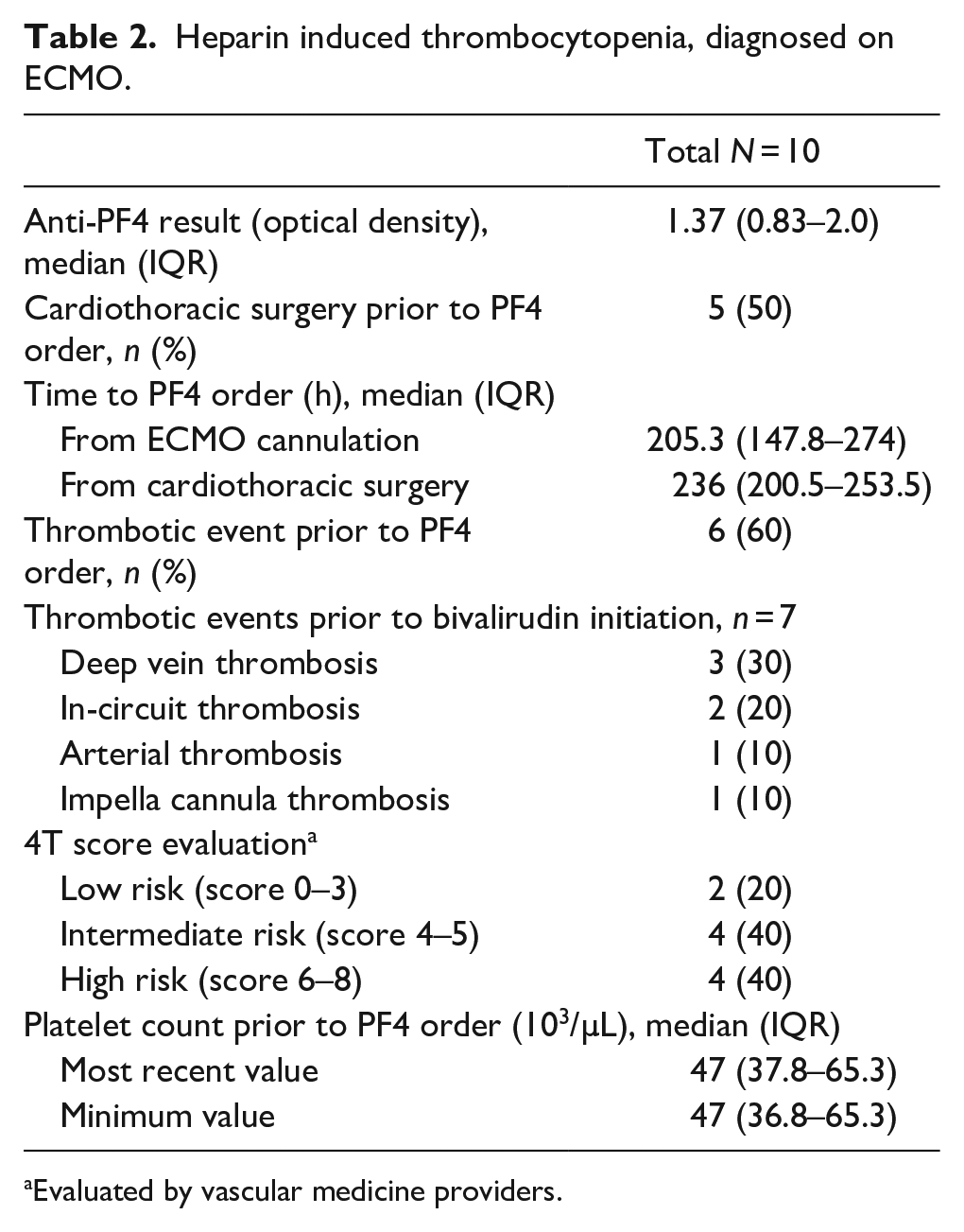
Evaluated by vascular medicine providers.
No patients experienced the primary outcome of in-circuit thrombosis while on bivalirudin. The median initial dose of bivalirudin was 0.065 mg/kg/h (0.05–0.1 mg/kg/h) and the median time to achieve therapeutic anticoagulation was 6.4 (2–11.3) h (Table 3). The median time from bivalirudin initiation to ECMO decannulation or death was 106.8 (70.4–192) h. Patients within this cohort were within the defined therapeutic range for 71.3% of total bivalirudin time on ECMO and 139 (66.2%) aPTTs were within therapeutic range. One patient did not have bivalirudin titrated to a therapeutic aPTT due to continued oozing from ECMO cannula sites. Excluding this patient, the total time in therapeutic range for the cohort was 81.7%. Post-oxygenator partial pressures of oxygen (PO2) were stable after anticoagulation switch with a median of 265.5 (214.8–301) mmHg before bivalirudin initiation to 283 (199.3–313) mmHg afterward, using the lowest PO2 documented until decannulation or death. All patients exhibited an increase in platelet count of at least 25% after bivalirudin initiation. One patient developed a deep vein thrombosis (DVT) 22.5 h after switching from heparin to bivalirudin. This patient was therapeutic on bivalirudin at the time of DVT diagnosis and no low ECMO flows were documented during ECMO support prior to diagnosis of the thrombotic event.
Heparin-induced thrombocytopenia treatment, bivalirudin.
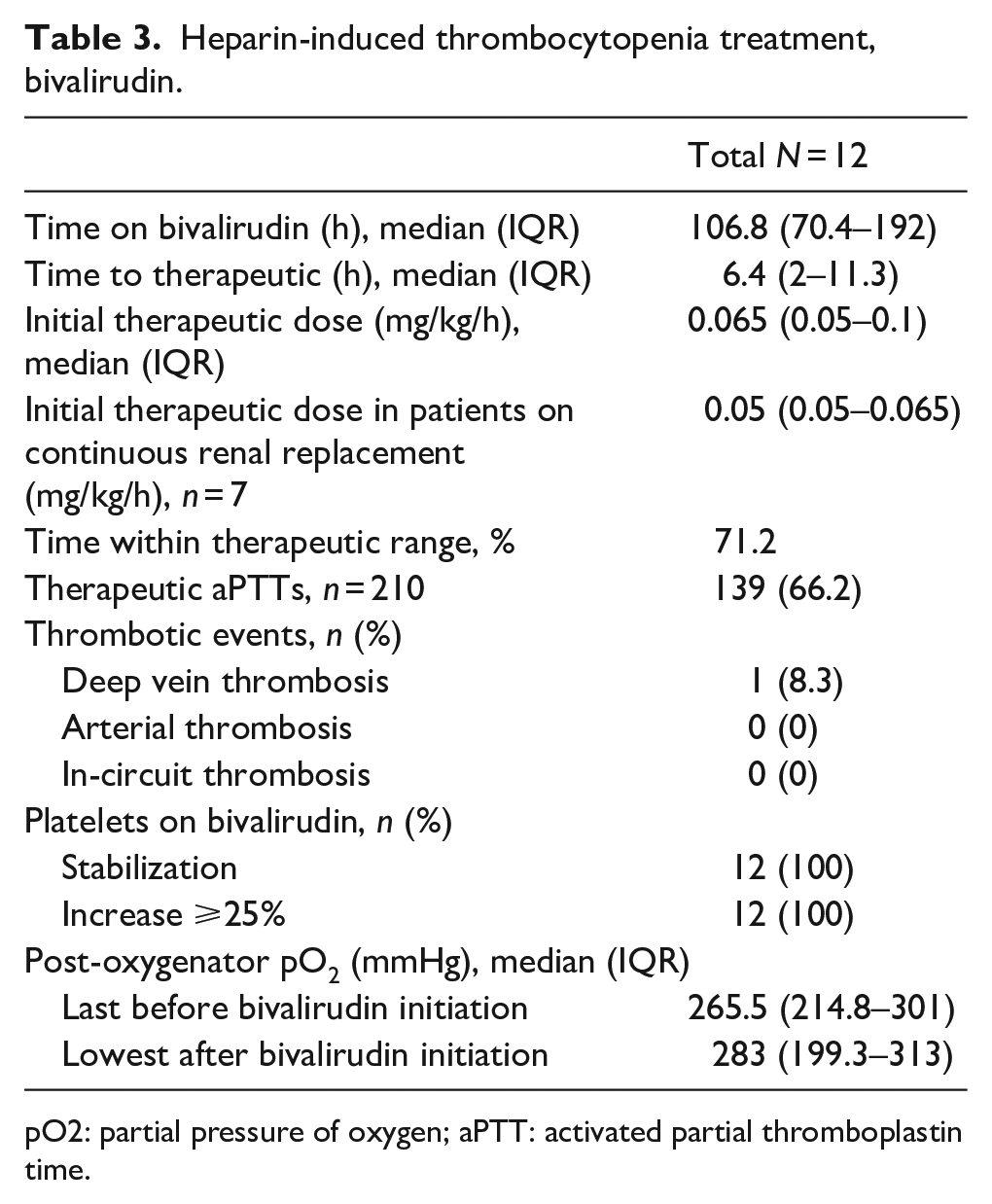
pO2: partial pressure of oxygen; aPTT: activated partial thromboplastin time.
Major bleeding occurred during bivalirudin therapy in eight (66.7%) patients and minor bleeding occurred in two (16.7%) patients (Table 4). Major bleeding locations included four (50%) surgical site bleeds, three (37.5%) central nervous system (CNS) bleeds, and one (12.5%) gastrointestinal-related bleed. Of the three patients with CNS related bleeding, one patient experienced an intracerebral hemorrhage and two patients experienced subarachnoid hemorrhages. This bleeding led to withdrawal of care and eventual mortality in two patients. All five patients that were administered an antiplatelet during ECMO cannulation experienced a major bleeding event. Only two (16.7%) patients in our cohort were free from bleeding events during bivalirudin therapy. Of the eight major bleeding events, two (25%) patients had an aPTT that was supratherapeutic prior to the bleeding event at 65.8 and 77.6 s. Four (50%) patients that experienced a major bleeding event on bivalirudin underwent continuous renal replacement therapy while on ECMO. Bleeding events occurred a median time of 39.8 (19.3–107.5) h from bivalirudin initiation. Patients experiencing a major bleeding event required 4.1 mL/kg/day in transfusion of PRBC during their bivalirudin course. Antiplatelet agents were concomitantly ordered in five (62.5%) patients that experienced a major bleeding event.
Patient bleeding events on bivalirudin.
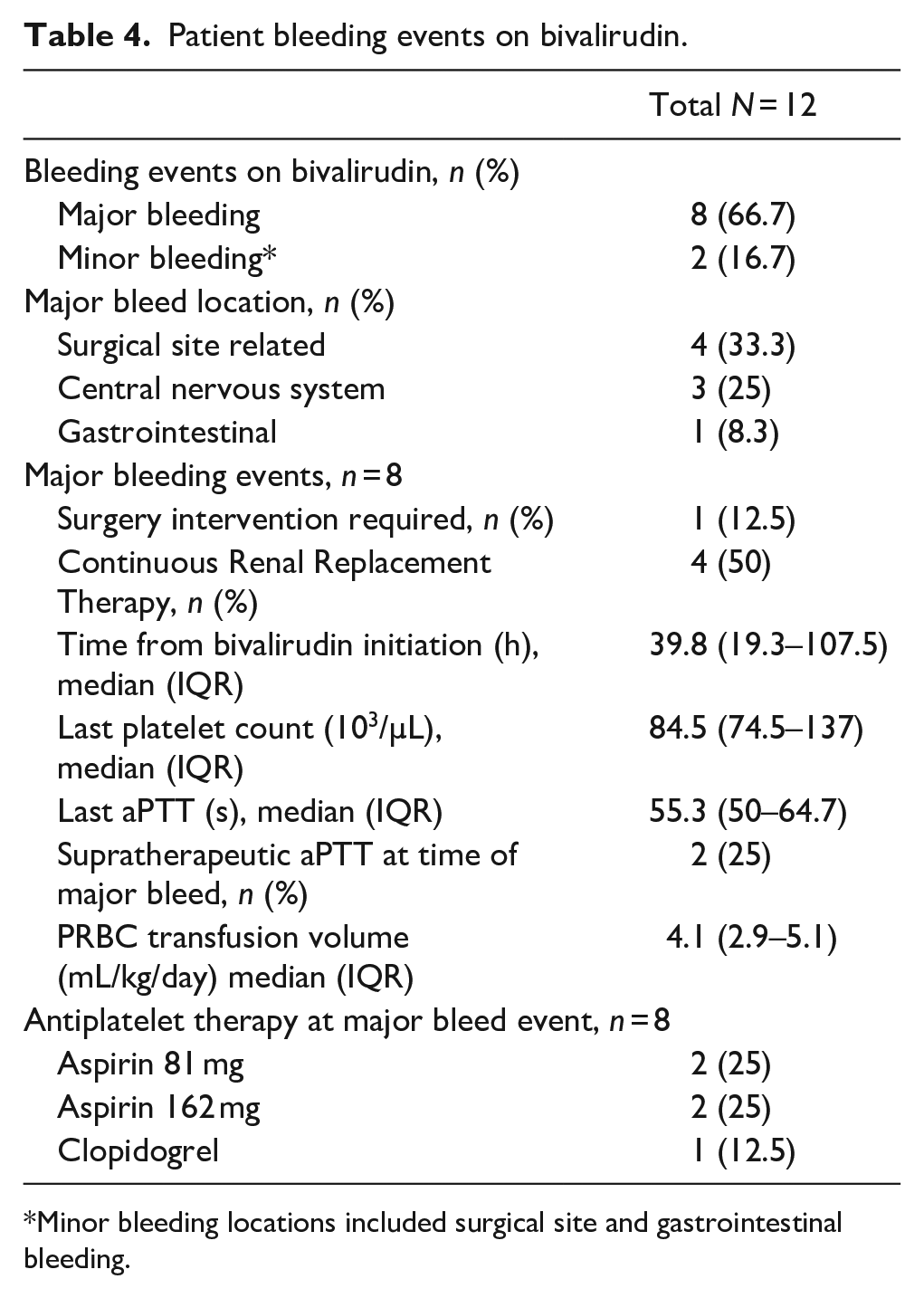
Minor bleeding locations included surgical site and gastrointestinal bleeding.
Discussion
To our knowledge, we describe the largest cohort of patients managed with bivalirudin while on ECMO for the treatment of HIT. This retrospective observational study found no evidence of our primary outcome of in-circuit thrombosis. Patients in our cohort spent a large percentage of time within therapeutic range on bivalirudin and reached therapeutic aPTT soon after initiation. Major bleeding events were frequent within this small cohort of patients, including three central nervous system-related hemorrhages. In addition, interpretation of the 4T score may be unreliable in patients requiring ECMO as the majority of patients fell into either low or intermediate risk for HIT.
Previous literature describing the use of bivalirudin for treatment of HIT for patients requiring ECMO is extremely limited. In 2009, Pappalardo et al. 14 detailed a patient treated with bivalirudin for acute HIT on V-A ECMO after mitral valve replacement. The patient developed a new thrombus on the atrial side of the new prosthesis on bivalirudin and exhibited persistent thrombocytopenia throughout the duration of ECMO support. The etiology of this continued HIT-mediated reaction was confounded by the use of a heparin-coated ECMO circuit. Stagnant intracardiac blood in a patient with refractory cardiogenic shock, combined with bivalirudin’s unique mechanism of elimination via enzymatic metabolism may have contributed to this new left atrial thrombus formation.
In 2017, Natt et al. 12 further added to the literature detailing five patients with suspected HIT on ECMO, two of which were newly diagnosed and confirmed by SRA. All patients were successfully treated with bivalirudin, exhibiting resolution of thrombocytopenia and absence of new thrombosis. These small retrospective case reports support the need for additional literature. The absence of serious thrombotic complications in our cohort should provide clinicians increased comfort in managing patients with bivalirudin for HIT in this population. Although one patient developed a DVT during HIT treatment with bivalirudin, given the timing after HIT diagnosis this thrombus may have been present prior to detection of HIT while the patient was anticoagulated with heparin.
A significant concern with utilizing bivalirudin as primary anticoagulant in the ECMO population is the risk of hemorrhagic complications due to the lack of a specific reversal agent. Our analysis showed a high rate of major bleeding with bivalirudin therapy, including three central nervous system bleeds. Previous literature has displayed widely varying rates of major or significant bleeding in adult ECMO patients on bivalirudin ranging anywhere from 5.3% to 72.7%, though definitions of bleeding vary widely between studies.3,9,15,16 Though not specific to the HIT population, Rivosecchi et al. 17 reported one of the largest cohorts to date of ECMO patients on bivalirudin, reporting a major bleeding rate of 11.7%. The analysis by Rivosecchi et al. is limited by the enrollment of only patients requiring V-V ECMO and did not assess anticoagulation intensity. Comparatively, our cohort enrolled a higher percentage of post-surgical patients and patients requiring V-A ECMO. In 2021, Giuliano et al., 18 published a retrospective cohort study of 144 ECMO patients to compare rates of complications with bivalirudin versus heparin. The authors included 13 patients treated with bivalirudin, however, this cohort was limited to only 4 patients with confirmed HIT. The authors found no differences in rates of hemorrhagic complications between heparin and bivalirudin, though the analysis was limited by its retrospective nature and limited sample size. 18 The etiology of increased major bleeding in our cohort compared to previous studies is uncertain and these results should be interpreted with caution given our small sample size. In addition, all patients that were administered an antiplatelet within our cohort experienced a major bleeding event. This high rate of bleeding may have been related to increased platelet inhibition in an already thrombocytopenic population.
Our median initial therapeutic dose of bivalirudin within this study was 0.065 mg/kg/h. Sanfilippo et al. 19 previously published a systematic review discussing bivalirudin dosing in ECMO patients. The authors found widely variable dosing within their studied population, however, adult patients on continuous renal replacement consistently necessitated higher rates of bivalirudin. Contrary to this finding, patients on continuous renal replacement within our small cohort required low initial bivalirudin infusion rates to reach therapeutic range. These results should be cautiously interpreted as we did not trend bivalirudin dosing requirements throughout the entire course of ECMO therapy.
Currently, there is no validated scoring tool to predict the diagnosis of HIT in the ECMO population. The 4T score has previously been evaluated by Kimmoun et al. 20 in conjunction with a positive anti-PF4 assay. Used together, they were found to have poor predictive value for the presence of HIT in a V-A ECMO population. Glick et al., 5 found the median 4T score within a HIT-positive ECMO population to equate to a score estimating an intermediate risk for HIT. The majority of patients within our cohort were estimated at a low to intermediate risk category. The presence of ECMO is often documented as a definitive cause of thrombocytopenia, lowering the maximum possible 4T score and potentially resulting in a missed diagnosis of HIT. Many patients requiring ECMO have undergone cardiothoracic surgery, a patient population with a higher risk for HIT than the general medical population and one where traditional methods for assessing risk for HIT may be confounded. 21 Further research is needed to develop a predictive scoring tool for the presence of HIT specific to the ECMO population.
This study has inherent limitations as it is a retrospective single-center evaluation of a small cohort of patients on ECMO. In addition, the study enrolled patients over a 5 year period in which changes in practice over time that may not have been accounted for could have potentially impacted our results. Because bivalirudin was the institutional agent of choice for the treatment of HIT, this analysis lacked a comparator evaluating patients treated with an alternative agent for HIT while on ECMO. In addition, the lack of an institutional protocol for regular monitoring of venous thromboembolic events upon HIT diagnosis may have resulted in late detection of the recorded thrombotic event on bivalirudin. Lastly, our institution does not strictly protocolize anticoagulation monitoring and dose adjustments, as targets are often dependent on individual patient bleeding and thrombotic risk.
Overall, our study results suggest that bivalirudin is effective for the management of HIT and did not show evidence of in-circuit thrombosis. A high incidence of major bleeding was observed, including central nervous system-related bleeding. Clinicians should view bivalirudin as an acceptable agent for the treatment of HIT in the ECMO population, but must consider bleeding risk given the lack of effective reversal agents. Future studies are needed to prospectively evaluate bivalirudin for the treatment of HIT in the ECMO population to assess risk of hemorrhage.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.