
Abstract
Background:
Sleep disturbances in patients with chronic kidney disease (CKD) are related to decreased quality of life and increased health-related risks. There is insufficient data about actual prevalence and related factors of poor sleepers in this group. In this study, we aimed to investigate prevalence and related risk factors of self-reported poor sleep quality in patients with pre-dialysis CKD.
Methods:
In this cross-sectional study, 259 pre-dialysis CKD patients (median age 56 years; range, 19–85) were included. Demographical, clinical and laboratory correlates were recorded. Body mass index (BMI) was calculated. Estimated glomerular filtration rate (eGFR) was calculated by the Modification of Diet in Renal Disease (MDRD) formula. Sleep quality was assessed by Pittsburgh Sleep Quality Index (PSQI), a self-rated questionnaire. Depression was evaluated using the Beck Depression Inventory (BDI).
Results:
Median eGFR was 27.6 ml/min/1.73 m2 (range, 9–56). Of the 259 patients, 110 (42.5%) were poor sleepers with global PSQI score >5. The univariate correlation analysis revealed that global PSQI score was positively correlated with age, BMI, waist circumferences (WC), hip circumferences (HC), serum phosphorus and triglyceride levels, systolic blood pressure (BP), pulse pressure and BDI score, and negatively correlated with male gender and hemoglobin level. Logistic regression analysis, showed that HC, systolic BP, and BDI scores were independently associated with poor sleep quality (p = 0.001, p = 0.020 and p < 0.001, respectively).
Conclusion:
Prevalence of poor sleep quality in our pre-dialysis CKD patients was 42.5%. Systolic BP, depression and HC, all of these are potentially correctable factors, were associated with poor sleep quality independently.
Introduction
Sleep is very important for the physiological recovery of the body, and sleep disorders are common and complex problems. In patients with chronic kidney disease (CKD), sleep disturbances are related to decreased quality of life, increased health-related risks (cardiovascular risks, impaired immune system, progression of CKD to end-stage renal disease (ESRD) and even mortality).1–3
Sleep disorders include insomnia, excessive sleepiness, sleep apnea, restless legs syndrome/periodic limb movement disorder. 1 Sleep disturbances in ESRD may be under-recognized by healthcare providers 4 and mean prevalence have been reported as 44% (20%−83%). 5 Prevalence of poor sleep quality (SQ) ranges from 41% to 83% in hemodialysis patients, 49%−85% in peritoneal dialysis patients and 14%−85% in pre-dialysis chronic kidney disease.6–8 Poor SQ in CKD may result from multiple complex interactive processes (CKD-related factor such as uremia and anemia, psychosocial factors, lifestyle factors, medication side effects, other comorbid conditions, etc.). 1 In the elderly with poor SQ, long sleep duration is associated with higher risk of cardiovascular mortality. 9 Also, short sleepers with poor SQ have an increased risk of total cardiovascular disease and coronary heart disease. 10 Insufficient sleep and poor SQ promote the development and exacerbate the severity of hypertension, type 2 diabetes, and obesity and might be a risk factor for the development and progression of CKD. 8 Optimizing sleep duration and quality and treating sleep disorders may reduce the severity and may delay the progression of CKD. 8
Sleep quality and its correlates in patients with pre-dialysis CKD is relatively less investigated and there is insufficient data about actual prevalence and related factors of poor sleepers in that group of patients. In this study, we aimed to investigate prevalence and related risk factors of self-reported poor SQ in Turkish patients with pre-dialysis CKD.
Methods
In this cross-sectional study, 259 patients with pre-dialysis CKD, who had follow-up visits in Nephrology Department of Konya Training and Research Hospital between January 2015 and June 2015, were included. Study protocol was approved by the Medical Ethics Committee of Necmettin Erbakan University Meram Faculty of Medicine (approval number: 2014/78) and written informed consent was obtained from all patient included in the study.
For the CKD diagnosis, clinical practice guidelines of National Kidney Foundation Disease Outcomes Quality Initiative (NKF-K/DOQI) was used. 11 Pre-dialysis CKD patients with the calculation of estimated glomerular filtration rate (eGFR) under 60 ml/min/1.73 m2, aged ⩾18 years and who could complete the sleep questionnaire and who provided written informed consent were included in the study.
The exclusion criteria were as follows: (1) patients who underwent renal replacement therapy (hemodialysis, peritoneal dialysis, renal transplant); (2) patients with chronic obstructive pulmonary disease and sleep apnea, acute cardiovascular disorders or uncontrolled heart failure, acute infection or cerebrovascular disease, (3) patients with dementia or psychotic disease.
Demographical and laboratory parameters including blood pressure (BP), pulse pressure (calculated as systolic BP - diastolic BP), height, body weight, body mass index (BMI), waist circumference (WC) and hip circumference (HC); serum urea, creatinine, uric acid, glucose, sodium, potassium, calcium, phosphorus, albumin, ferritin, parathormon (PTH), total cholesterol, low-density lipoprotein cholesterol (LDL-cholesterol), high-density lipoprotein cholesterol (HDL-cholesterol), triglyceride, C-reactive protein (CRP), hemoglobin levels and eGFR values were all recorded. Body mass index (BMI), in kg/m2, was calculated as weight (kilogram, kg) divided by squared height (meter, m); eGFR was calculated by the Modification of Diet in Renal Disease (MDRD) formula. 12 SQ was assessed by Pittsburgh Sleep Quality Index (PSQI), self-rated questionnaire. This index has high validity and reliability for evaluating sleep disorders and contains 19 self-related questions to evaluate SQ during the previous month. These questions are related to seven components: subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbances, use of sleep medications, and daytime dysfunction. Each component was scored from 0 to 3, resulting a global PSQI score between 0 and 21. Patients with a global PSQI score >5 were defined as “poor sleepers” and those with a global PSQI score ⩽5 were defined as “good sleepers.” 13 Depression was evaluated using the Beck Depression Inventory (BDI) of which the validation and reliability study in a Turkish population was made by Kapci et al. 14 BDI is a 21-items, multiple-choice self-report inventory; contains 21 questions, each answer is given a score on a scale value of 0–3. Higher total scores of BDI indicate more severe depressive symptoms. 15
Statistical analyses were carried out using the Statistical package for Social Sciences for Windows version 15.0 (SPSS, Chicago, IL, USA). Data were expressed as mean ± SD and median (min-max). Student’s t-test was used to compare the means of normally distributed variables between groups and the Mann-Whitney U-test was used for variables that were not normally distributed. The differences among the categorical variables were analyzed using the X2 test or the two-tailed Fisher’s exact test, as appropriate. The relationship between the variables was evaluated using Pearson’s or Spearman correlation coefficient. Multiple logistic regression with forward stepwise selection was performed to identify factors independently associated with “poor sleep.”
Results
In this study, 259 pre-dialysis CKD patients (123 female, 47.5%; 136 male, 52.5%) with a median age 56 years (range, 19–85) were included. Median eGFR was 27.6 (9–56) ml/min/1.73 m2. Of these patients, 72 (27.8%) had diabetes mellitus; 46 (17.8%) had hypertension; 33 (12.7%) polycystic kidney disease; 27 (10.4%) chronic interstitial nephritis; 26 patients (10%) had glomerulonephritis; 4 (1.5%) amyloidosis and 51 (19.7%) patients had unknown underlying etiologies. Median PSQI score of all study group was 4.69 (range, 0–19). Of the 259 patients, 110 (42.5%) were poor sleepers with global PSQI score >5. Demographical and laboratory parameters of all patients and that of the poor SQ group and the good SQ group were summarized in Table 1.
Demographic, clinical and laboratory characteristics of all study group, poor sleepers group and good sleepers group.
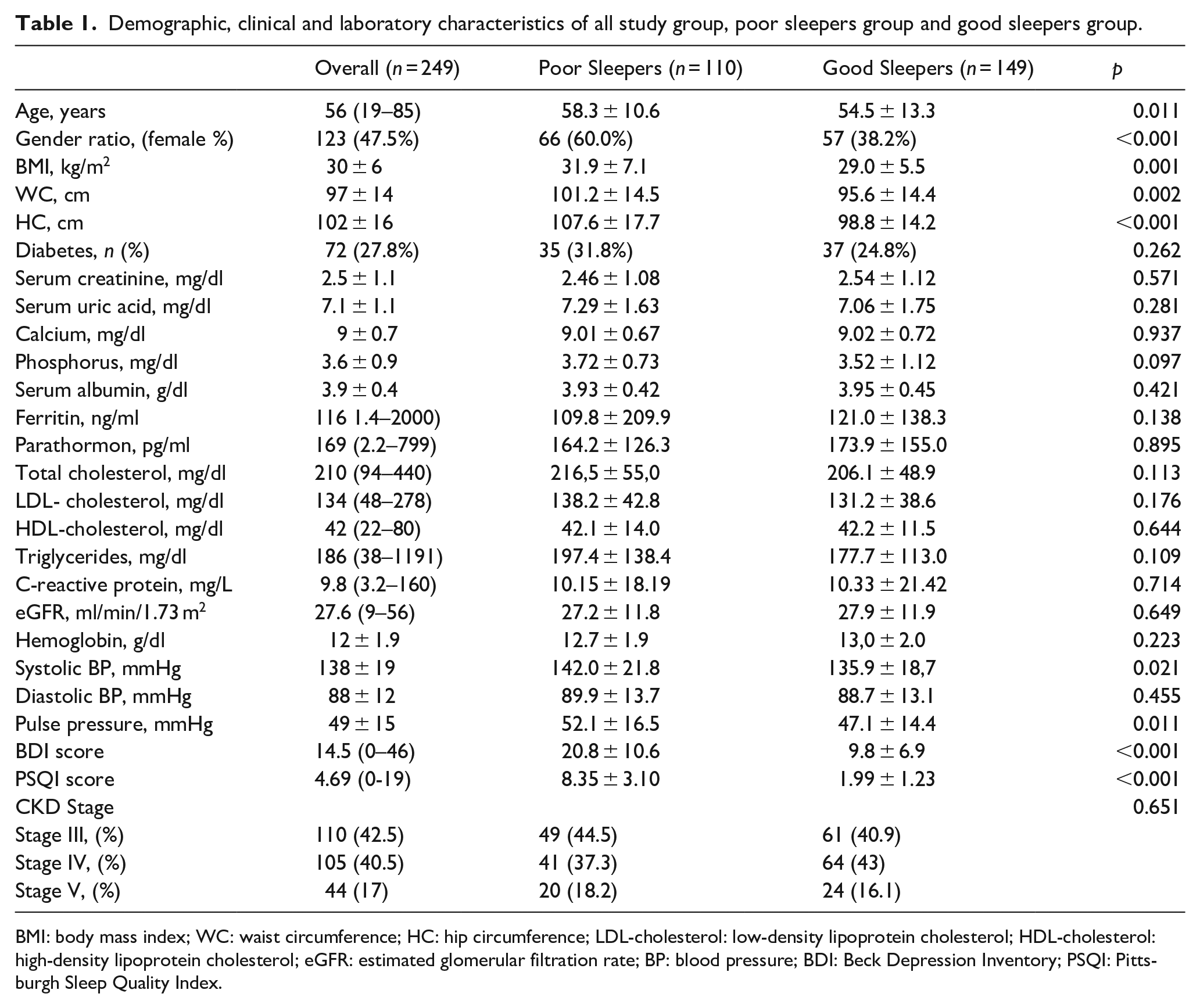
BMI: body mass index; WC: waist circumference; HC: hip circumference; LDL-cholesterol: low-density lipoprotein cholesterol; HDL-cholesterol: high-density lipoprotein cholesterol; eGFR: estimated glomerular filtration rate; BP: blood pressure; BDI: Beck Depression Inventory; PSQI: Pittsburgh Sleep Quality Index.
Compared with good SQ group, the patients in poor SQ group had older age (58.3 ± 10.6 vs 54.5 ± 13.3, p = 0.013), higher female/male ratio (66/44 vs 57/92, p < 0.001), higher serum phosphorus level (3.72 ± 0.73 mg/dl vs 3.52 ± 1.12 mg/dl, p = 0.003), higher systolic BP and pulse pressure measurements (142.0 ± 21.8 mmHg vs 135.9 ± 18.7 mmHg, p = 0.034; 52.1 ± 16.5 vs 47.1 ± 14.4 mmHg, p = 0.014, respectively), higher BDI score (20.9 ± 10.6 vs 9.8 ± 7.03, p < 0.001). And compared with good sleepers, obesity measures such as BMI, WC, and HC values in poor SQ group were all higher (31.9 ± 7.1 vs 29.0 ± 5.5 kg/m2, p = 0.001; 101.2 ± 14.5 cm vs 95.6 ± 14.4 cm, p = 0.002; 107.6 ± 17.7 cm vs 98.8 ± 14.2 cm, p < 0.001, respectively). Good SQ group and poor SQ group were similar for the other variables (urea, uric acid, calcium, hemoglobin, ferritin, PTH, CRP, albumin, triglyceride, and cholesterol levels). The results were shown in Table 1. In addition, there was no difference between two groups in respect to CKD stage of patients (stage III, IV, V).
The univariate correlation analysis revealed that global PSQI score was positively correlated with age (r = 0.163, p = 0.008), BMI (r = 0.213, p = 0.001), WC (r = 0.205, p = 0.001), HC (r = 0.222, p < 0.001), serum phosphorus levels (r = 0.212, p = 0.001), triglyceride levels (r = 0.154, p = 0.014), systolic BP (r = 0.136, p = 0.030), pulse pressure (r = 0.137, p = 0.030) and BDI score (r = 0.572, p < 0.001), and negatively correlated with male gender (r = −0.216, p < 0.001) and hemoglobin level (r = −0.129, p = 0.038) (Table 2). Multivariate logistic regression analysis including age, gender, BMI, HC, WC, serum triglycerides, phosphorus, hemoglobin levels, systolic BP, pulse pressure, and BDI score showed that HC (OR = 1.035, p = 0.001), systolic BP (OR = 1.020, p = 0.020) and BDI scores (OR = 1.158, p < 0.001) were independently associated with poor SQ (R2 = 0.331) (Table 3).
Univariate correlation of PSQI score (Pittsburgh Sleep Quality Index) with other variables in overall study population.
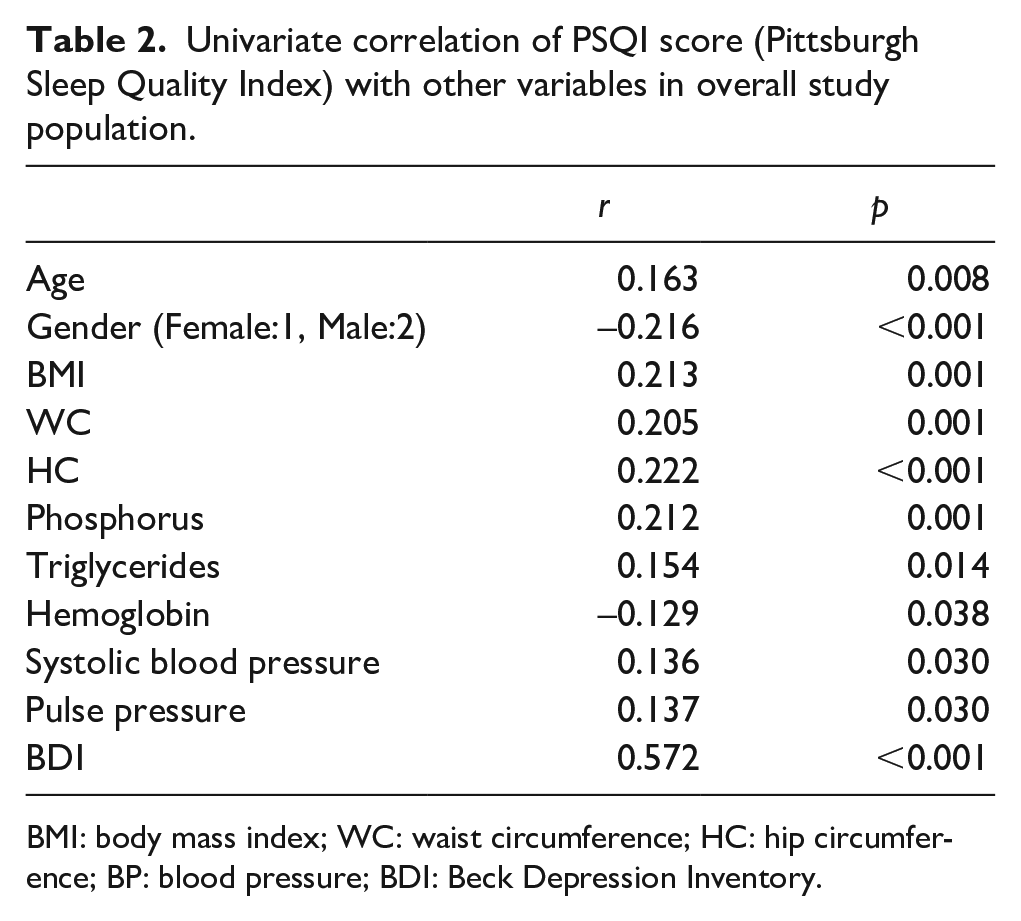
BMI: body mass index; WC: waist circumference; HC: hip circumference; BP: blood pressure; BDI: Beck Depression Inventory.
Multivariate logistic regression analysis for poor sleep quality.
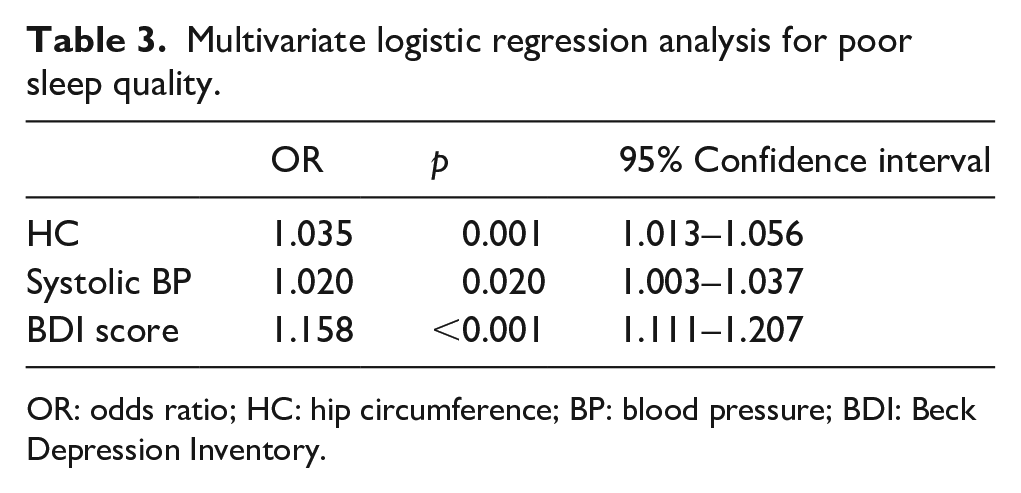
OR: odds ratio; HC: hip circumference; BP: blood pressure; BDI: Beck Depression Inventory.
Discussion
This study is one of the large studies which investigate SQ in patients with pre-dialysis CKD. In this study, it was found that the prevalence of poor SQ in predialysis CKD was 42.5%. In previous studies, prevalence of sleep disorders based on questionnaires ranged from 14 to 85% in pre-dialysis CKD.2,8,16,17 The prevalence of poor sleepers in our study group was somewhere near the middle of this range. This wide range may be due to heterogeneity of the study populations (different primary cause of CKD, different life styles, environmental conditions, genetic factors in the study populations), non-uniform subjective methodology (different questionnaires) rather than objective sleep measures like polysomnographic or actigraphic measures.
Similar to the prevalence of poor SQ, the findings of previous studies about related factors of it have yielded mixed results in CKD patients. Heterogeneity of the study populations and methodology and different measurement tools may cause these mixed results.
In an epidemiological study, in the general population, sleep disorders were seen more frequently in female. 18 Similarly, our poor sleeper group had a higher female/male ratio. In a study with CKD patients including both pre-dialysis patients and the patients on renal replacement therapy, it was found that female gender was associated with lower SQ. 19 But the study of Iliescu et al., failed to show any relation between SQ and gender. 20 Our findings showed that poor sleepers group had older age. Some studies found significant relation between age and SQ,17,21 some studies didn’t show the correlation between SQ and age in CKD patients. 19
Kurella et al. 22 reported a significant association between eGFR and SQ in CKD patients. But, other studies didn’t show such relation,2,16,17,19,21 consistent with our study. We found no association between SQ and degree of renal failure, in accordance with the findings of Iliescu et al. 16 and Zhang et al. 17 It is suggested that SQ may decrease at a very early stage in CKD without direct effect of decreased renal function.16,17 Disruption of the circadian rhythm by internal factors such as melatonin might lead to sleep disturbances in CKD. 23 Determining the melatonin levels of both groups would be useful.
Our poor sleeper group had higher serum phosphorus levels, despite not statistically significant in comparison. While it had significance in univariate analysis, its significance was not retained after multivariate regression analysis. Calcium and PTH levels similar in both good sleeper and poor sleeper groups. Sabbatini et al. 21 did not find any relation between SQ and PTH levels in CKD patients in various stages. But Li et al., reported an association between calcium × phosphate product and poor SQ in continuous ambulatory peritoneal dialysis patients. 24 One hypothesis about this relation is that elevated calcium × phosphate product is related with secondary hyperparathyroidism, coronary calcification and increased cardiovascular mortality. 25 Poor SQ in these patients might be caused by underlying vascular calcification and atherosclerosis. Second hypothesis, increased calcium × phosphate product or phosphorus cause pruritis 26 and pruritis lead to poor SQ. Third hypothesis, just an our speculation, is elevated phosphorus or elevated calcium × phosphate product might cause pineal gland calcification which may result in decrease melatonin secretion. And the decrease in melatonin secretion may cause poor SQ.
This study also showed that HC, systolic BP and BDI scores were independently associated with poor SQ. HC is an obesity measure and obesity may be a risk factor for progression to ESRD. 8 Decrease in sleep quantity may promote weight. 8 In healthy adults, short sleep has an important effect on the neuroendocrine control of appetite. 27 At the same time, obesity is the major cause of obstructive sleep apnea. 8 Poor sleep can promote risk of hypertension and increase its severity. 8 In CKD patients, there may be sympatho-vagal imbalance due to baroreceptor reflex dysfunction with hyperactivity of sympathetic nervous system and decreased vagal tone. 1 In healthy individuals, during sleep, sympathetic activity decrease and vagal tone increase resulting in nocturnal dipping of BP. The patients with sleep disorders sympathetic nervous system stimulation increases and parasympathetic activity decreases which results in reduced nocturnal dipping of blood pressure. 1 Sleep deprivation may also interfere the oscillatory nature of cardiac sympatho-vagal balance and plasma renin levels. Lack of nocturnal BP dipping is a risk factor for progression of CKD and antihypertensive therapy in the evenings may reduce this risk. 1
In some previous studies, it was reported that depression was independent predictors of SQ in hemodialysis patients,6,28,29 peritoneal dialysis patients 7 and pre-dialysis CKD patients. 16 Relation between SQ and depression is also well-known in general populatin. 30 Causal relations of poor SQ with depression, obesity and hypertension may be bidirectional, becoming a vicious cycle and the aim should be to break this cycle.
Knowing the importance of preventive medicine (in this situation secondary prevention) and the data that improving SQ may delay the progression of CKD, 19 the clinician should take into account the modifiable factors related with poor SQ, such as HC, BP and depression found in our study, while mapping out the interventions to retard the progression to ESRD and to defer the need of renal replacement therapies. As the first step, clinician could assess sleep complaints and disorders of all patients with CKD by using PSQI, and then determine the accurate diagnostic procedures and interventions related to specific sleep disorders (e.g. somnography for assessment of sleep apnea, using continuous positive airway pressure (CPAP) machines; evaluation of sleep hygiene for insomnia and excessive sleepiness, recommendations about good sleep habits, physical exercise, etc.). And also, with the additional data from the findings of our study, dealing with potentially correctable factors related with poor SQ including hypertension, depression and obesity should be recommended.
There are some limitations in our study: first, this study yielded no causal relationship due to cross-sectional design. Second, we analyzed the data of self-reported SQ by the use of the PSQI, a subjective assessment and we used single time point measurements. Using objective measures such as polysomnogram would preclude reporting bias and define specific forms of sleep disorders. Strengths of our study were quite large sample size, with homogen study population (only patients with non-dialysis-dependent CKD) from a single center (precluding potential variability between different centers).
In conclusion, findings of our study showed that, prevalence of poor SQ quality in pre-dialysis CKD patients was 42.5% and systolic BP, depression and HC, all of these are potentially correctable factors, were associated with poor SQ independently. Longitudinal well-designed larger clinical studies are required to determine actual prevalence of poor SQ and the complex interrelationship between SQ and other factors and to evaluate the interventions for improving SQ in CKD patients, especially in pre-dialysis stage.
Footnotes
Author contributions
R.Y. conducted the study and wrote the manuscript with support from I.G. I.G. supervised the project and conceived the original idea.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.