
Abstract
Acute respiratory distress syndrome (ARDS) can develop early in burn patients with inhalation injury in the presence of cytokine storm and the proinflammatory response can be a supplemental factor for ARDS aggravation. We report the case of a 41-years old male with 25% total body surface area deep partial thickness burns to upper body extremity and grade II inhalational injury who developed severe ARDS, nosocomial pneumonia, and septic shock. Veno-venous extracorporeal membrane oxygenation (VV ECMO) and continuous renal replacement therapy (CRRT) with hemoadsorption were successfully used at different moments to overcome critical situations. Although debatable, the use of ECMO in burn patients with severe ARDS could be considered when conventional treatment fails. The use of CRRT combined with hemoadsorption may limit the proinflammatory response sustained by the combination between major burn, ECMO and sepsis.
Keywords
Introduction
Mortality from burn trauma is high, despite optimal fluid resuscitation, respiratory management, and early surgical excision of burned areas. Respiratory complications are one of the major determinants of mortality in burn patients, particularly if associated with inhalation injury. 1
The incidence of inhalational injury following exposure to smoke or chemical products of combustion is as high as 14% in patients with more than 80% total body surface area (TBSA) burn injury. 2 The risk for pneumonia increases by 42% per day in its presence. 2 Chest radiography can have a normal appearance after an inhalational injury and bronchoscopy remains the gold standard for assessing its presence and severity. 3 Exposure to smoke or chemicals in an enclosed space, as well as extensive facial and neck burns could indicate inhalational injury and need for intubation. 4
Acute respiratory distress syndrome (ARDS) can develop early in patients with major burn injury and inhalation injury in the presence of cytokine storm. Mechanical ventilation, nosocomial pneumonia and transfusion are independent risk factors for late onset ARDS in this population. While protective ventilation, prone positioning, neuromuscular blockade, and extracorporeal membrane oxygenation (ECMO) demonstrated favorable outcome in severe ARDS management, ECMO is not a conventional therapy. 5 In burn patients with ARDS, the evidence for ECMO-related benefits on survival is limited by the shortcomings of small case series reports with variable outcomes; no randomized controlled trials of ECMO versus conventional therapy have been undertaken in this population up to this point.
Case report
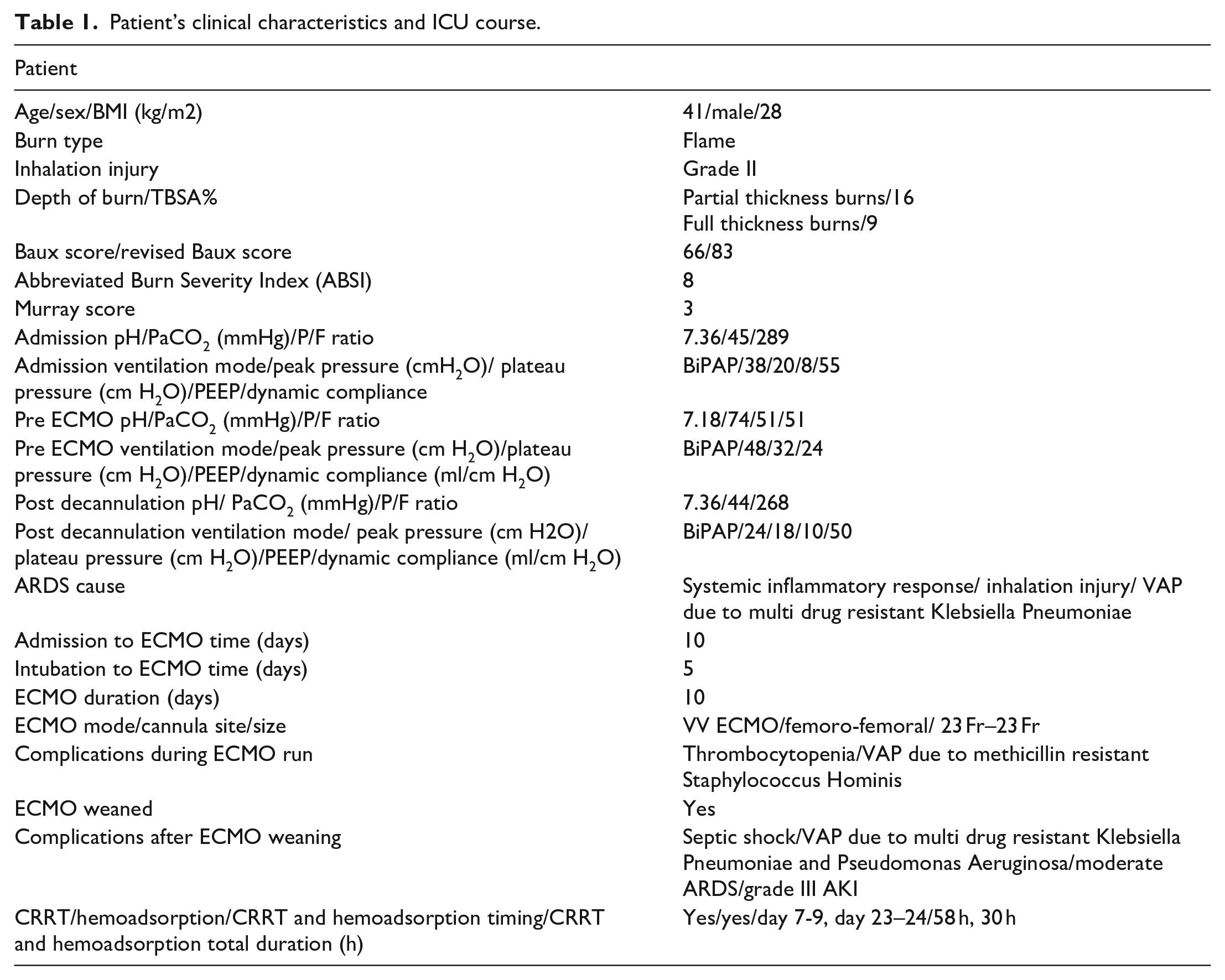
A 82 kg, 1.82 m, 41-years old male with no significant medical history was admitted to the emergency room following 25% TBSA deep partial thickness burns to face, head and bilateral upper extremities. The patient was exposed to fire followed by an explosion in an enclosed night club, with a high suspicion of thermal and chemical inhalational injury. The patient’s clinical characteristics and ICU course are summarized in Table 1.
Patient’s clinical characteristics and ICU course.
On admission, the patient was intubated and underwent emergent right hand and forearm escharotomy with decompression fasciotomies. The bronchoscopy showed grade II inhalational injury with moderate degree of mucosal erythema, predominantly on the trachea and right main bronchia and diffuse alveolar hemorrhage. The bronchoalveolar lavage (BAL) was negative at this point. Apart from a mild ARDS, the patient presented no other organ dysfunction and was extubated on day 4.
Less than 24 h after extubation, the patient developed a septic shock and was reintubated due to severe hypoxemia. A steep increase in C-reactive protein (CRP) and procalcitonin (PCT) levels was noted (Figure 1). Chest radiograph demonstrated increased pulmonary interstitial edema, with new onset basal and perihilar bilateral alveolar infiltrations. The bronchoscopy showed diffuse alveolar hemorrhage, severe mucosal erythema and edema on the trachea and left superior bronchia and hypovascular mucosa on the right superior bronchia. BAL cultures and rectal swab were positive for multi drug resistant Klebsiella Pneumoniae. A 7-day antibiotic course with tigecycline and colistin was initiated according to antibiogram, but the patient developed severe ARDS within the following days. Protective ventilation and neuromuscular blockade were initiated on day 8, when FiO2 requirement escalated more than 70%. Prone position was considered but was technically impossible due to burn lesions. Tracheostomy was performed on day 7. A transthoracic echocardiography performed on day 8 showed a 60% left ventricle ejection fraction with mild right ventricle dysfunction and a pulmonary artery systolic pressure (PAPS) of 55 mmHg. The maximum noradrenaline dose was 0.5 µg/kg per min. Inhaled nitrous oxide therapy was initiated on day 8 to improve ventilation-perfusion mismatch, right ventricle function and to lower the PAPS. Continuous veno-venous hemofiltration (CVVH) combined with hemoadsorption (Cytosorb®; CytoSorbents Europe) was performed on days 7–9 on a Prismaflex® system (Baxter, USA) using a Prismaflex® ST150 set (Baxter, USA). The circuit was primed with normal saline and Phoxillum® solution was used as substitution fluid. The procedure was performed by a subclavian catheter with systemic heparin anticoagulation, with a blood flow of 200 mL/min, ultrafiltrate of 100 mL/h, substitution of 1800 mL/h and predilution of 500 mL/h. The vasopressor infusion was no longer necessary on day 9. Grafting of the right hand and forearm were performed on day 7.
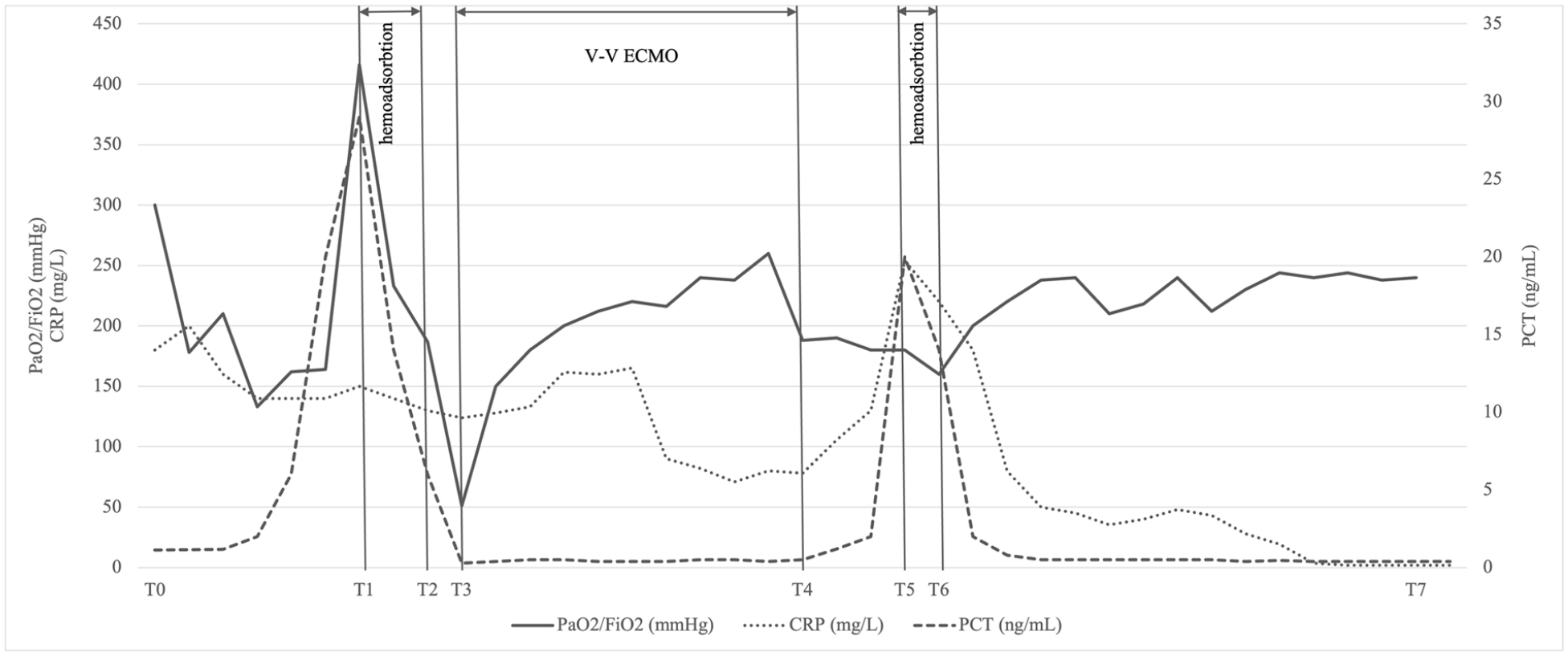
Trajectories of CRP, PCT and PaO2/FiO2 during the ICU stay. Dynamics of CRP and PCT at the time of ICU admission (T0), before and after the first (T2-T3) and the second hemoadsorbtion treatment (T5-T6) and at ICU discharge (T7); dynamics of PaO2/FiO2 at the time of ICU admission (T0), before and after V-V ECMO (T4-T5) and at ICU discharge (T7). T0-ICU day 1, T1-ICU day 7, T2-ICU day 9, T3-ICU day 10, T4-ICU day 20, T5-ICU day 23, T6-ICU day 24, T7-ICU day 71.
On day 10, the patient was progressively acidemic from hypercapnia and the PaO2/ FiO2 could not be improved above 51 mmHg, despite protective ventilation, neuromuscular blockade and nitrous oxide. Given the single organ failure, the ECMO mobile team decided to initiate veno-venous (VV) ECMO. The patient was cannulated at bedside using transesophageal echocardiographic guidance. Both internal jugular veins were inaccessible to cannulation due to burn injuries, so the left femoral vein was cannulated with a 23 Fr multistage access canula (Medtronic, USA) and the left femoral vein with a 23 Fr return canula (Medtronic, USA). Initial VV ECMO (Maquet Cardiohelp System, Gettinge, Sweden) flows of 4.2–4.4 L/min were required to keep oxygen saturation levels higher than 95%. After VV ECMO initiation, the patient was transferred to a tertiary cardiac intensive care unit with experienced staff in ECMO management.
Following VV ECMO initiation, ultraprotective lung ventilation was employed and neuromuscular blockade was discontinued on day 14. A bronchoscopy performed on day 17 revealed a normal aspect of the tracheal and bronchial mucosa. The BAL was positive with methicillin resistant Staphylococcus Hominis and a 7-day antibiotic course with Linezolid was initiated according to antibiogram. VV ECMO support was progressively titrated down and the patient was decannulated on day 20. Tube thoracostomies were placed bilaterally for pleural effusions before decannulation. Except for thrombocytopenia, no other organ dysfunction was documented during the ECMO course.
Two days after decannulation, the patient developed a septic shock following a ventilator associated pneumonia with multi drug resistant Klebsiella Pneumoniae and Pseudomonas Aeruginosa, which was treated with a 7-day course of tigecycline and colistin according to antibiogram. The maximum dose of noradrenaline was 0.6 µg/kg per min. Increased levels of CRP and PCT were noted and CVVH with hemoadsorption (Cytosorb®) was performed on days 23–24. The CVVH prescription, the system and the circuit were the same as for the first CRRT. The use of CVVH with Cytosorb® was associated with decreased CRP and PCT levels (Figure 1). The vasopressor infusion was no longer necessary on day 26.
Following consecutive trials of spontaneous breathing, the tracheostomy canula was removed on day 33. After 38 days of respiratory physiotherapy, the patient left the intensive care unit on day 71 following his initial hospital admission (day 61 following admission to tertiary cardiac intensive care unit). The patient underwent full recovery with good mobility of both upper extremities and successful skin grafting and was discharge from hospital on day 73. All microbiological samples of his burn wounds remained negative during the hospital stay.
Discussion
The place for ECMO in burn patients with inhalational injury and severe ARDS is still debatable at this point and the literature on the use of ECMO in this population is limited. While some case report series present encouraging results,6–11 others advocate the need of conducting randomized controlled trials evaluating the outcomes of ECMO use in burn trauma related ARDS 12 or even recommend against its use 13 (Table 2).
Recent studies addressing the use of ECMO in adult burn patients (chronological order).
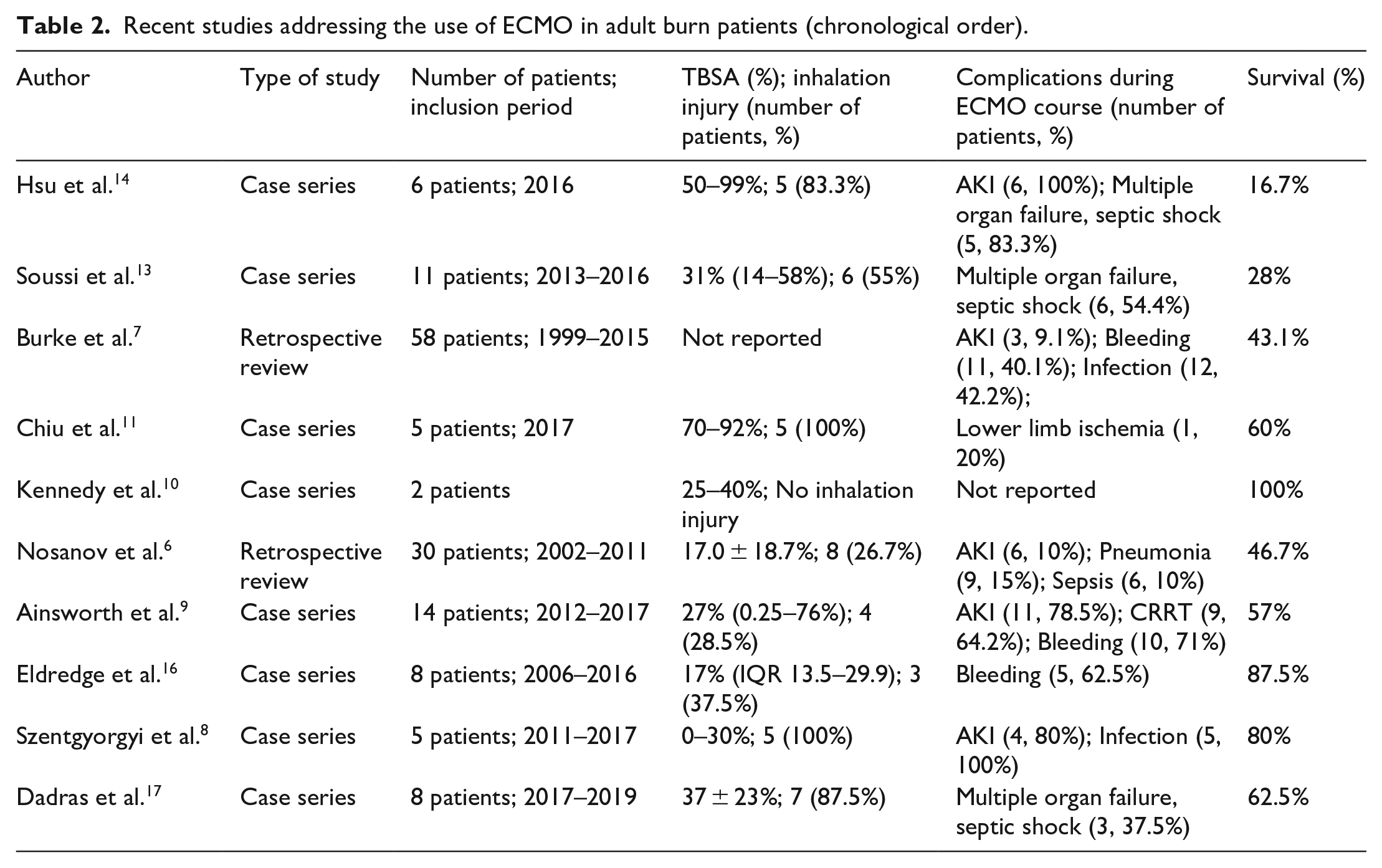
A systematic review and meta-analysis assessing the level of evidence for the use of ECMO in hypoxemic respiratory failure resulting from burn and smoke inhalation injury found no improvement in survival with the use of ECMO. 12 In 2016, the French PROBURN group recommended against ECMO use in burn patients with severe ARDS until further evidence is obtained, reporting in-hospital mortality of 91% for 11 burn patients. 13 Similarly, Hsu et al. reported an overall survival rate of 16.7% in an analysis of six burn patients with ECMO for severe ARDS 14 Caution should be taken when evaluating the results of these case series, since all non-survival patients had already very high Baux scores 14 and predicted mortality risk prior to ECMO initiation.13,14
However, the largest cohort of patients who received ECMO following burn related injuries comes from the ELSO database. 7 Between 1999 and 2015, 58 patients were identified, with a reported survival to hospital discharge of 43.1%. The need for CRRT during ECMO was associated with negative outcome and survival was higher in patients with lower TBSA, but lower in patients in inhalational injury. Another retrospective analysis from the American Burn Association reported an overall survival rate to discharge of 47%, similar to that reported by ELSO. 6
Recent case series also report survival rates similar or higher than those reported by the ELSO registry analysis.8,9,11,15 Moreover, survival rates in other recent case series nearly match those reported for non-burn injured patients with severe ARDS treated with ECMO, suggesting that the presence of burn injury should not exclude ECMO as treatment option for patients with severe ARDS related to burn injuries.16,17 More likely, caution should be taken when evaluating the indication for ECMO, especially in patients with high predicted mortality rates, as ECMO for circulatory support should not be used as final solution in patients with non-reversible causes. Randomized control trials of ECMO versus conventional therapy in severe ARDS following severe burn injuries will probably address the problem in the future but the limit remains the low number of patients recruitable.
Since renal failure is associated with negative outcome in burn patients7,18 and multiple organ failure due to sepsis is reported as a major cause of mortality in recurrent studies, the use of hemofiltration combined with hemoadsorption may prove to have beneficial effects on outcome. Cytokine reduction during CRRT in the setting of inflammatory response associated ARDS is reported to result in rapid and significant reduction in the levels of IL-6 and IL-8, improvement in hemodynamic stability, increase in P/F ratio and diminution of capillary leak syndrome. 19 Controlling proinflammatory response with hemoadsorption during ECMO has been reported to result in reduced levels of IL-6, IL-8, PCT and reduced vasopressor need in various categories of patients. 20
In this case, circulatory support proved to be an asset and partial respiratory function recovery was achieved after 10 days of VV ECMO. VV ECMO and CRRT with hemoadsorption were used at different moments to overcome critical situations in a severe burn patient with inhalation injury who developed septic shock, nosocomial pneumonia and severe ARDS.
Due to the complex mechanical and pharmacological support that was employed in this case, it is however difficult to conclude that hemoadsorption before VV ECMO initiation was a major determinant of the successful clinical course, especially since cytokines levels were not determined. Nonetheless, significant hemodynamic improvement and reduction in inflammatory markers were observed during CRRT combined with hemoadsorption and probably limited the cytokine storm which could have resulted in multiple organ dysfunction following VV ECMO initiation.
Conclusions
The use of ECMO in selected burn patients with severe ARDS can be considered when conventional ARDS management fails. The use of CRRT combined with hemoadsorption can be of particular interest in this case, since the proinflammatory response is sustained by a combination between major burn, ECMO and sepsis and can on its own be a supplemental factor for ARDS aggravation.
Footnotes
Author contributions
Conceptualization, S.-I. B.-T., D.C. and L.V.; writing—original draft preparation, S.-I. B.-T., D.C, S.B., P. M., L.V.; writing—review and editing, S.-I. B.-T., L.V. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Informed consent statement
Written informed consent has been obtained from the patient to publish this paper.