
Abstract
Background:
The aim of the study is to compare the results of patients who had moderate or severe tricuspid insufficiency (TI) at the time of left ventricular assist device (LVAD) implantation that did not undergo intervention.
Methods:
Between October 2013 and December 2019, 144 patients who did not undergo tricuspid valve repair (TVR) during LVAD implantation in our department were included in the study. The patients were divided into two groups according to the TI grade; Group 1: 106 patients (73.6%) with moderate TI and Group 2: 38 patients (26.4%) with severe TI. All patients were evaluated for mortality, need of inotrope, blood product transfusion, intensive care unit (ICU) stay, duration of mechanical ventilation, and early and late right ventricular failure (RVF). Minimally invasive technique was favored in patients with worse right ventricular (RV) function to prevent the need for postoperative RV support and bleeding.
Results:
The mean ages of the patients in the Group 1 and Group 2 were 46 ± 15 years (82% male), and 45 ± 11.2 years (81.5% males), respectively. Post-operative duration of mechanical ventilation, ICU stay, blood loss, and reoperations were similar (p > 0.05). There was no significant difference in early RVF, pump thrombosis, stroke, bleeding, and 30-day mortality between groups (p > 0.05). Incidence of late RVF was higher in Group 2 (p < 0.05).
Conclusion:
Although the risk of late RVF may increase in patients with preoperative severe TI, not intervening in TI during LVAD implantation does not cause adverse clinical outcomes in the early period.
Introduction
The need of LVAD implantations is increasing in patients who cannot receive a heart transplant. 1 In this view, the need for LVAD implantation increases in patients with various valve pathologies beyond isolated left ventricular failure. In patients living with heart failure for a long time, the pulmonary artery pressure rises due to the increase in left atrial pressure, and this situation may reflect on the right ventricle and cause tricuspid valve insufficiency (TI). 2
The optimal management of TI in patients undergoing LVAD implantation is controversial. Although there are studies3,4 showing that tricuspid valve repair (TVR) protects from postoperative right ventricular failure (RVF) in advanced valve insufficiency during LVAD implantation, studies5,6 showing the opposite have also been published in recent years. The aim of this study was to evaluate the clinical outcomes of patients who had severe TI at the time of LVAD implantation but did not undergo tricuspid valve intervention.
Materials and methods
Between October 2013 and December 2019, 144 patients (over 18 years of age) underwent LVAD implantation without TVR. Before the surgery, transthoracic echocardiography (TTE) was performed in all of the patients and 106 (73.6%) of the patients had moderate TI as “Group 1,” and the remaining 38 (26.4%) patients had severe TI as “Group 2.” Patient data were obtained retrospectively using the hospital data system. We assessed pre-operative demographics, clinical, and laboratory data of the patients such as age, sex, body mass index, Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) profiles, etiology, right heart catheterization, blood count, kidney and liver functions, electrolytes, NT-proBNP, TTE parameters, and device and incision type. Exclusion criteria were TVR at the time of LVAD implantation, previous tricuspid valve surgery, and LVAD implantation with no long-term success. In Group 1, patients with moderate and severe TI before IABP and ECMO were implanted for this group were excluded from the study.
In all patients, pre-operative and periodically post-operative TTE was performed to assess the valve pathology, left ventricle ejection fraction, tricuspid annular plane systolic excursion (TAPSE), right ventricle fractional area change, and right ventricles’ and left ventricle end diastolic diameter by an expert cardiologist. The severity of TI was determined based on the preoperative TTE and defined according to the appropriate guidelines, 7 ranged from grade 1 to 3: “1” for mild TI, “2” for moderate TI, and “3” for severe TI. Late RVF was defined as any readmission for right- sided heart failure after LVAD implantation, requiring medical treatment with diuretic agents or inotropes or surgical implantation of a right ventricular assist device. 8
All of the surgical procedures were performed by the same surgical team. Patients underwent LVAD implantation under cardiopulmonary bypass (CPB) either by median sternotomy or minimally invasive left thoracotomy. Transesophageal echocardiography was performed intraoperatively in all patients and TI was confirmed. Aorto-unicaval or aorto-femoral cannulation were performed according to the previous surgical history. Apical ring was inserted after “sew and cut” method without fibrillation and cross-clamping.
We analyzed operative data, duration of mechanical ventilation and intensive care unit (ICU) stay, post-operative bleeding and blood transfusion, RVF, intraaortic balloon pump (IABP), transient mechanical support for right ventricle, duration of hospital stay, follow-up, clinical outcomes, and adverse events (pump thrombosis and stroke). Primary endpoints were mortality and orthotopic heart transplantation. Secondary endpoints were adverse events like, readmissions due to late RVF, device failure, pump thrombosis, inflow or outflow obstruction, gastrointestinal bleeding, driveline fracture or infection, or pulmonary disease.
Statistics
IBM SPSS 20 program (IBM Corp., Armonk, NY, USA) was used for analysis. Numeric variables were shown as mean ± standard deviation and categorical variables were given as frequency and percentage. Normality of quantitative variables was evaluated with Kolmogorov–Smirnov test. For normally and non-normally distributed data; Student t test and Mann–Whitney U test were used for two independent group comparisons, respectively. The relationship between qualitative variables was evaluated with chi-square analysis. Kaplan–Meier test used for survival analysis. p < 0.05 was considered as statistically significant.
Results
The demographics of the patients were given in Table 1. The mean age of the patients was 46 ± 15 years (82.0% male) in Group 1, and 45 ± 11.2 years (81.5% males) in Group 2 (p = 0.677 and p = 0.946, respectively). Baseline characteristics were similar between groups, such as height, weight, etiology, history of cardiac surgery, and cerebrovascular events. Pre-operative clinical status like INTERMACS profiles, pulmonary artery catheterization, and laboratory values were also similar. There was no difference between the groups in right and left ventricular functions before the operation (Table 1).
Demographics of the patients.
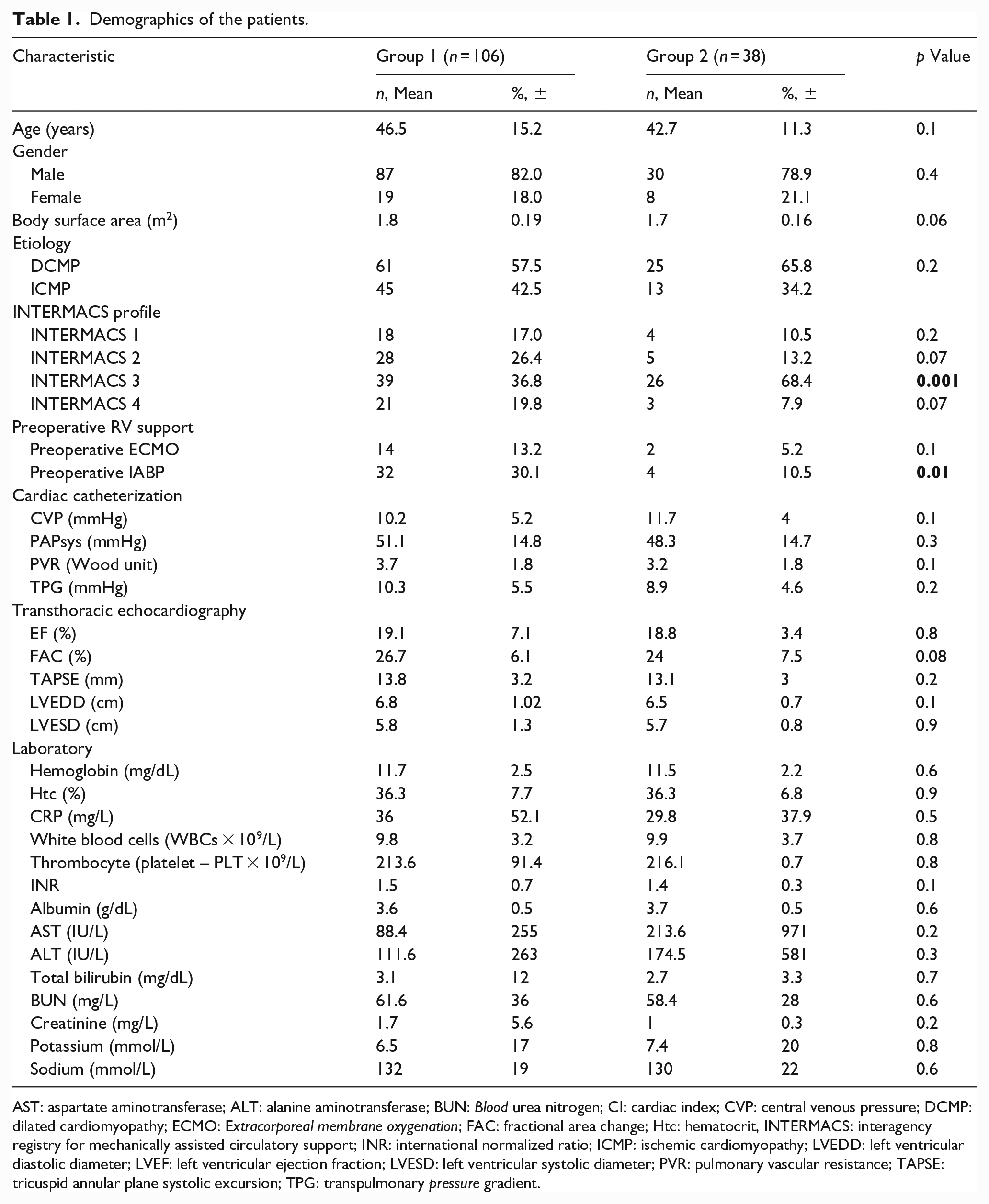
AST: aspartate aminotransferase; ALT: alanine aminotransferase; BUN: Blood urea nitrogen; CI: cardiac index; CVP: central venous pressure; DCMP: dilated cardiomyopathy; ECMO: Extracorporeal membrane oxygenation; FAC: fractional area change; Htc: hematocrit, INTERMACS: interagency registry for mechanically assisted circulatory support; INR: international normalized ratio; ICMP: ischemic cardiomyopathy; LVEDD: left ventricular diastolic diameter; LVEF: left ventricular ejection fraction; LVESD: left ventricular systolic diameter; PVR: pulmonary vascular resistance; TAPSE: tricuspid annular plane systolic excursion; TPG: transpulmonary pressure gradient.
Clinical outcomes were summarized in Table 2. In Group 1, 77 (72.6%) of the patients were operated via median sternotomy, whereas in Group 2, minimally invasive implantation was preferred in 17 (44.7%) patients. There was no difference between CPB times in both groups (p = 0.635). Heartware (HeartWare®, Medtronic, MN, USA), and Heartmate 3 (Abbott, Burlington, MA, USA) devices comprised the majority of our cohort, with no difference between groups (p = 0.3). Post-operative duration of mechanical ventilation, ICU stay, blood loss, and reoperations were also similar (p > 0.05). There was no significant difference in post-operative RVF and need of IABP/extracorporeal membrane oxygenation
Comparison of the outcomes of the groups.
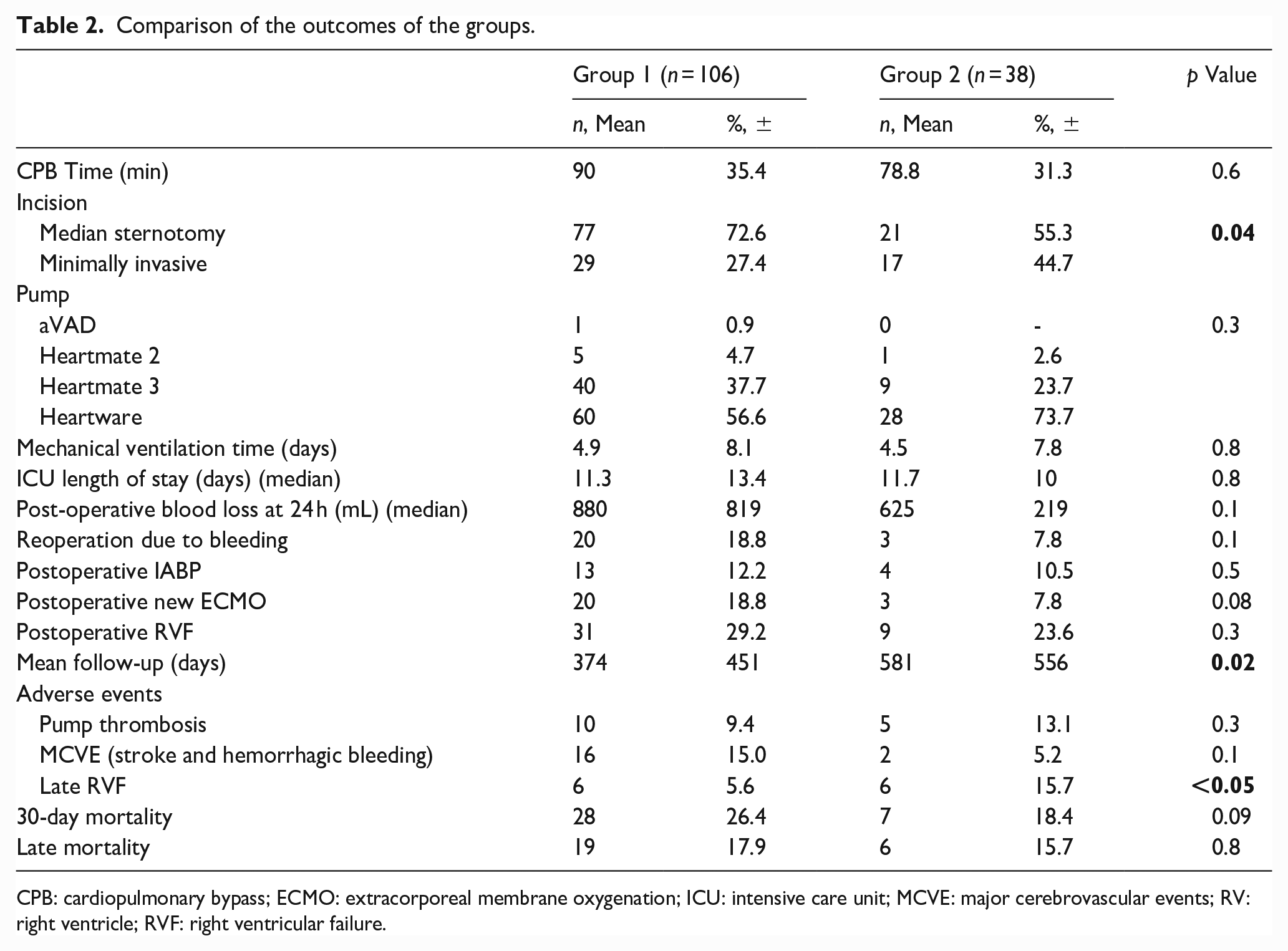
CPB: cardiopulmonary bypass; ECMO: extracorporeal membrane oxygenation; ICU: intensive care unit; MCVE: major cerebrovascular events; RV: right ventricle; RVF: right ventricular failure.
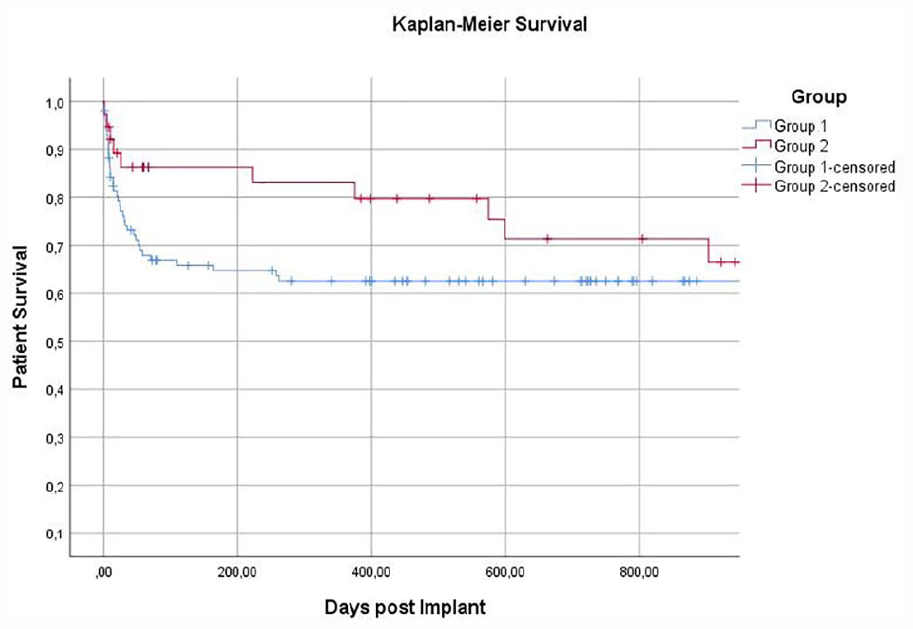
Kaplan–Meier survival analysis.
Discussion
Severe TI is a condition that can complicate postoperative management in patients with LVAD and prior studies have shown the rate of severe TI to be up to 14% in patients with advanced heart failure undergoing continuous flow LVAD implantation. 9
Right ventricular (RV) dysfunction and severe TI are commonly associated with a failing left ventricle. Presence of preoperative TI and its persistence after surgery have been described as risk factors for a poor late outcome. 10 For these patients, there is controversy over the intervention of TI during LVAD implantation. Previously, there were studies 2 showing that mid-term mortality increases if the valve with severe TI is not treated at the time of LVAD implantation, and studies 3 have also been published showing that patients who underwent concomitant tricuspid valve replacement survived longer than those who underwent LVAD alone. Conversely, concomitant tricuspid valve replacement has not been shown to be beneficial in patients with grade >2 tricuspid valve regurgitation undergoing LVAD implantation. 11 Filsoufi et al. 12 reported that TVR has a high mortality when combined with other concomitant procedures. Zhigalov et al. 13 reported that survival was not significantly different between the groups. In TVR group, there was a higher need for open chest after surgery and a prolonged inotrope use because of RVF, a higher incidence of acute kidney dysfunction requiring dialysis, and a higher blood transfusion rate due to postoperative bleeding. Robertson et al. 14 reported outcomes in 2,196 patients with moderate or severe TI who underwent LVAD implantation in an analysis of the Society of Thoracic Surgeons database. After propensity score adjustment, concurrent tricuspid valve surgery was associated with significantly longer ICU (>72 h) and hospital (>3 weeks) stay, higher transfusion requirement, new renal failure rates, new dialysis requirements, and any reoperation.
Our study supports “do not touch the tricuspid valve” strategy. Most patients with severe TI secondary to a left-sided pathology have functional TI, characterized by a markedly enlarged annulus with a relatively normal leaflet anatomy. 2 TI secondary to left heart failure may tend to improve in the short and long term due to a sudden drop in left atrial pressure after the LVAD implantation, unless there is a primary valve pathology. Lee et al. 15 reported significant reductions in pulmonary capillary wedge pressure during LVAD support. As a result of increased cardiac output, a decrease in ventricular stroke work, ventricular stroke work index, and TAPSE indicates that the unloaded RV does not need to contract so vigorously to pump enough blood to the left side of the heart.
In essence, the unloading provided by LVAD has a lusitropic effect on the RV. In our two-group comparison, the lack of difference between clinical findings such as post-operative mechanical ventilation time, ICU length of stay, need for mechanical circulatory support, and blood transfusion showed that the right ventricle adapts quickly to the new situation independent of TI after LVAD implantation and that the “untouched” valve was not associated with adverse events, especially in the early period. In cases of concomitant tricuspid valve surgery, an increase may be seen in adverse events as the complexity of the case increases. In concomitant cases, the duration of cardiopulmonary bypass may be prolonged and the amount of bleeding may increase accordingly.9,13,16
In addition to the mechanical reduction of left atrial pressure by the LVAD, the drugs we use in the per-operative period also help to reduce the load on the right ventricle. First of all, we use levosimendan for patient optimization in all eligible patients before the operation and try to relieve congestion as much as possible with diuretics. We attempt to minimize CPB times by performing the outflow graft anastomosis off-pump, reserving CPB only for the inflow portion of the procedure. When weaning from CPB during the operation, inhaled nitric oxide is started and continued until extubation. When oral intake started, we use sildenafil and continue with the inhaler iloprost for at least 2 weeks. In this way, we try to reduce the load on the right ventricle and thus on the tricuspid valve. These manipulations protect the patients from the adverse events of advanced TI in the early post-operative period.
This study presents that, in cases with severe TI, during LVAD implantation, not to intervene in this valve does not cause an additional adverse event in the early period, but may cause RVF in the long term. Although TI is severe, “do not touch the valve” option caused neither early RVF nor higher mortality post-operatively. In published reports, the incidence of late RVF in patients undergoing LVAD implantation ranges from 11% to 16%.17–19 Barac et al. 20 reported results of tricuspid valve repair in patients with LVAD. Of the total, 59 patients (37.8%) had a failed TVR. They showed the relationship between durability of TVR and outcomes, specifically for readmission for late RVF, and reported the incidence of late RVF as 36.3%. As shown in the final multivariate model, TVR failure was identified as an independent risk factor for the development of late RVF. In our study, the incidence of late-stage RVF in group 2 was 15.7%, and according to literature data, it was similar to late-stage RVF in patients with LVAD. The reason for this is that patients with TR can tolerate late RVF less frequently.
With the use of LVAD in destination therapy, the implantation of these devices in all age groups has increased worldwide. 21 Although overall mortality could be higher in elderly, RV dysfunction was not effected by age in a large study. 22 In our cohort, our patients were relatively young and this could be a reason of progression of TI within time.
The risk factors associated with early RVF are very well described in published reports, however, there is limited information regarding risk factors associated with late RVF. Our strategy is “do not touch the tricuspid valve” even if the patient has severe TI. We are very sensitive in patient selection, timing, and surgical treatment. Our aim is to prevent early RVF. Preload of RV is increased after LVAD implantation. RV cannot easily unload in situation of increasing afterload of RV after TVR. This causes early complications and right heart failure.
Limitations
This study is a retrospective study. This non-randomized single center study needs to be supported by randomized double-blind studies with larger numbers of patients. This study includes nonprotocolized echocardiographic follow-up and did not consider preoperative tricuspid valve annular geometry in our analysis.
Conclusion
In case of advanced TI, “not touching” to this valve during LVAD implantation does not lead to an increase in early adverse events. Maybe not touching TI act as a fuse of the right ventricle in the early stages and can help the LVAD running, acting as an escape window against a possible increase in pulmonary artery pressure. Our observations after LVAD implantation showed a trend towards a reduction in TI severity as loading conditions improved. However, reasons of late RVF would need to be confirmed in larger, prospective studies.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.