
Abstract
Objective:
To investigate the effects of low-calcium and standard-calcium dialysate in patients with chronic kidney disease on peritoneal dialysis, and find out which dialysate has less vascular calcification effect.
Methods:
A total of 141 patients who had undergone peritoneal dialysis (PD) for 2 years in the PD centre from January 2012 to December 2017 were included and divided into two groups according to the calcium concentration of the PD fluid used. There were 79 cases in the low-calcium group, with a dialysate calcium concentration of 1.25 mmol/L and 62 cases in the standard-calcium group, with a dialysate calcium concentration of 1.75 mmol/L. The demographic characteristics and clinical information before initiation of PD were collected and compared between the two groups. Information on the serum calcium, phosphorus and PTH, systolic and diastolic blood pressures and the use of antihypertensive and phosphate-lowering drugs in the second year of dialysis was also collected and compared between the two groups. Vascular calcification was assessed in patients on PD treatment.
Results:
The mean serum calcium concentrations before initiation of PD in the low- and standard-calcium groups were 1.94 ± 0.27 and 1.89 ± 0.28 mmol/L, respectively. The serum calcium concentrations after PD were 2.30 ± 0.21 and 2.41 ± 0.23 mmol/L, respectively. After PD, the serum calcium concentration in both groups was significantly increased (p < 0.05). The serum calcium concentration in the low-calcium group after PD treatment was lower than that in the standard-calcium group, and the difference was statistically significant (p < 0.05). Compared with the standard-calcium group, patients in the low-calcium group had significantly higher parathyroid hormone concentrations (p < 0.05). More types of phosphate-lowering drugs were used (59.49%) in the low-calcium group than that in the standard-calcium group (35.48%; p < 0.05). The number of antihypertensive drug usage were also higher in the low-calcium group, and the difference was statistically significant (p < 0.05). As for the vascular calcification effect, the two groups have shown no statistical difference in abdominal aortic calcification rate, carotid arteriosclerosis rate and aortic arch calcification rate (p < 0.05).
Conclusion:
We found that low-calcium PD fluid may increase the PTH level and the proportion of CKD patients using antihypertensive drug and phosphorus-lowering drug, but the vascular calcification effect of the low and standard calcium PD fluid needs further exploration. This paper provides new evidence for the choice of dialysate for PD, low-calcium dialysate has no outstanding advantages for long term dialysis.
Keywords
Introduction
Chronic kidney disease (CKD) is a common condition, which can cause an irreversible decline in renal function and may progress to chronic renal failure or uraemia in the later stages. 1 Chronic kidney disease-mineral and bone disorder (CKD-MBD) is a common complications, 2 which encompasses abnormal calcium, phosphorus, parathyroid hormone (PTH) and vitamin D metabolism, and further induces renal osteodystrophy and calcification of blood vessels and other soft tissues for CKD patients.3,4 Hypo-calcaemia, hyperphosphataemia and secondary hyperparathyroidism (SHPT) are the most frequently detected abnormal indicators of CKD-MBD in clinical practice. 5 High phosphorus also triggers and accelerates vascular calcification. 6 CKD, along with CKD-MBD, associated with poor quality of life, 7 and CKD is also seen as a risk factor of certain psychiatric diseases such as depression and anxiety.8,9
Peritoneal dialysis (PD) is a standard, economic, convenient and effective renal replacement therapy for patients with CKD. 10 Adjusting the calcium ion concentration in PD fluid is essential to correct the calcium and phosphorus balance in PD patients. 11 Studies have pointed out that using low-calcium dialysate combined with phosphate-lowering drugs and active vitamin D can better control blood calcium, phosphorus and PTH in patients and prevent and treat hyperphosphataemia, negative calcium balance, SHPT, renal failure and bone disease.12–14
However, a retrospective study showed no significant difference in mineral and bone metabolism between two groups of patients on continuous ambulatory PD after 2 years of treatment with low-calcium dialysate versus a standard-calcium dialysate. 15 Yamamoto et al. 16 found that PD patients using low-calcium PD fluid (approximately 1.8–2.5 mEq/L)required higher doses of phosphate binders and had significantly higher PTH than target levels (approximately 3.25–4.0 mEq/L). And low-calcium PD fluid is a risk factor for decreased bone mineral density in PD patients. 17 Therefore, whether PD based on low calcium dialysate has a more significant clinical effect on CKD patients is still different, which needs to be discussed through more clinical studies.
We provide a theoretical basis for choosing PD fluid in CKD by comparing the key indicators on serum calcium, phosphorus, full-segment parathyroid hormone level and rate of vascular calcification between the low-calcium or standard-calcium dialysate, in order to provide evidence on dialysate selection for CKD patients.
Materials and methods
Patients
A total of 141 patients who received PD and were followed up for at least 2 years regularly, from January 2012 to December 2017, were included. There were 79 cases in the low-calcium group and 62 in the standard-calcium group. The inclusion criteria were: (1) patients who underwent PD regularly in our hospital from January 2012 to December 2017; (2) patients received the calcium ion concentration of the PD fluid for the first time and were not changed during the course; and (3) patients whose treatment data, examination data and medical history data were complete. The exclusion criteria were: (1) patients under 18 years of age; (2) patients on Glucocorticoids therapy; (3) patients switched to haemodialysis or those receiving a combination of PD and haemodialysis; (4) patients with tumors; and (5) patients received parathyroidectomy. The ethics committee of our hospital approved this study. The patient details were anonymized. Informed consent was signed by all participants in this study before the study began.
Treatment
The low-calcium group received a dialysate with a calcium ion concentration of 1.25 mmol/L, whereas the standard-calcium group received a PD solution with a calcium ion concentration of 1.75 mmol/L.15,18 During PD, all patients received drug therapy such as phosphate-lowering agents, active vitamin D, antihypertensive drugs and erythropoietin in strict accordance with the guidelines and per the patient’s condition. Since active vitamin D inhibits PTH, increases calcium concentrations and regulates bone metabolism and possibly arterial calcification, the dosing regimen of active vitamin D was adjusted according to changes in the patients’ condition. In addition, the phosphate-lowering drugs received by all patients during dialysis were calcium-free.
The intact parathyroid hormone (iPTH) was determined by the chemiluminescence method with an Access Intact PTH assay (A16972, Beckman Coulter, USA), which is a two-site immune-enzymatic (sandwich) assay. The sample is added to a reaction vessel, along with a monoclonal anti-PTH antibody conjugated to alkaline phosphatase and tris-buffered saline with proteins and paramagnetic particles coated with a goat polyclonal anti-PTH antibody. After incubation in the reaction vessel, materials bound to the solid phase are held in a magnetic field, while unbound materials are washed away. The chemiluminescent substrate is then added to the vessel, and the light generated by the reaction is measured with a luminometer. The light production is directly proportional to the concentration of PTH in the sample. The amount of analyte in the sample is determined from a stored, multi-point calibration curve. The normal range of iPTH is 12–88 pg/mL.
Observation indicators
All patients were received PD and followed up for at least 2 years, the clinical data of patients were collected by the same research assistant through our hospital information system (HIS), and another research assistant is responsible for all data quality control:
(1) The demographic characteristics and clinical information collected included the sex, age, underlying disease, residual renal function, serum calcium, serum phosphorus, PTH, hemoglobin (Hb), systolic and diastolic blood pressure and Kt/V of the patients before initiation of PD. (2) Information on the serum calcium, phosphorus and PTH, systolic and diastolic blood pressures and the use of antihypertensive and phosphate-lowering drugs in the second year of dialysis was also collected. (3) For patients on PD for more than 1 year, the following investigations were done: chest X-ray, lateral abdominal X-ray and carotid artery colour Doppler ultrasound to evaluate calcification. The abdominal aortic calcification score (ACCS) is based on a semi-quantitative scoring method described by Kauppila et al. 19 The abdominal aortic calcification corresponding to the patient’s first to fourth lumbar vertebral bodies is determined, and the ACCS is calculated. According to the length of the calcified plaques on the anterior and posterior walls of the abdominal aorta corresponding to the first to fourth lumbar vertebrae, 0–3 points are assigned: The severity of each section of abdominal aorta was ranked by calcium score. Minor calcification as 1 point (calcifications range less than 1/3 of the corresponding arterial wall length), Moderate calcification as 2 point (calcification ranges from 1/3 to 2/3 of the corresponding arterial wall length), Moderate calcification as 3 point (calcification ranges from 1/3 to 2/3 of the corresponding arterial wall length). The total score is 0–24 points, and the calcification degree is finally divided into I, II and III grades according to 1–8 points, 9–16 points and 17–24 points respectively (Figure 1).
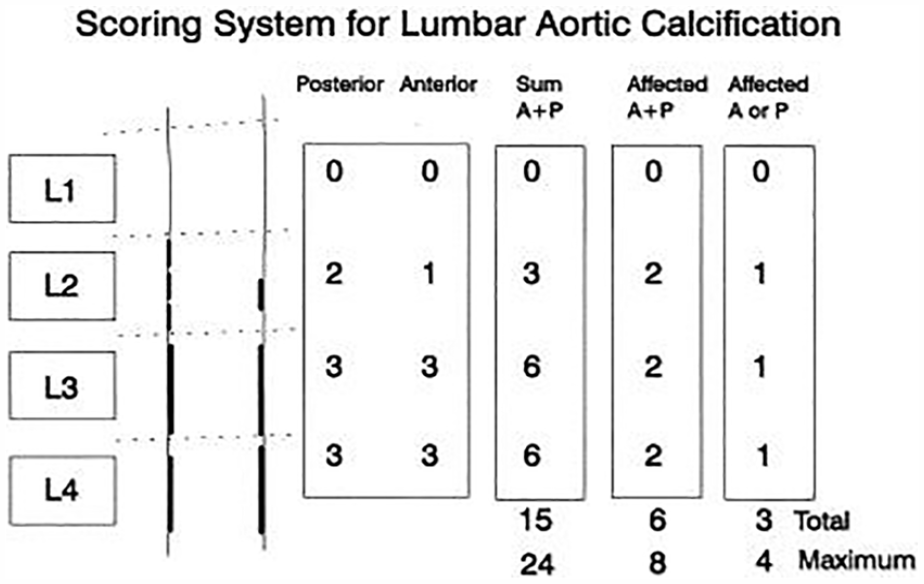
Schematic diagram of abdominal aorta score.
(4) The carotid plaque score was determined with the patient in the supine position during the examination of the left and the right carotid arteries. The carotid plaque score is a semi-quantitative estimate of the severity of the carotid plaque: The carotid plaque was semi-quantitative graded, Grade 0 (no calcification), Grade I (unilateral plaque ⩽2 mm), Grade II (unilateral plaque > 2 mm or both sides with plaques and at least one plaque ⩽2 mm) and Grade III (both plaques were larger than 2 mm). 20 The number of cases with aortic arch calcification, as seen on the chest X-ray, was also determined.
Statistical methods
The IBM SPSS Statistics for Windows, Version 23.0. (Armonk, NY) software was used for statistical analysis of the data. Continuous data conforming to a normal distribution (including age, serum calcium, serum phosphorus, Hb, eGFR, systolic blood pressure, diastolic blood pressure and Kt/V) were expressed as the mean ± standard error, and the independent-samples t-test and paired t-test were used for the comparison of groups and within groups. Non-normally distributed continuous data (including PTH) were expressed as median and interquartile range, and the Wilcoxon signed-rank test and the nonparametric Mann–Whitney U-test were used for intra- and inter-group comparisons. The categorical data (including gender, number of underlying diseases, previous medication history, current medication usage, antihypertensive drug usage, phosphorus-lowering drug usage, abdominal aortic calcification and carotid atherosclerosis) were expressed as frequencies or percentages, and the chi-squared test was used to compare groups. A value of p < 0.05 was considered statistically significant.
Results
The demographic characteristics and clinical information of patients on PD for more than 2 years
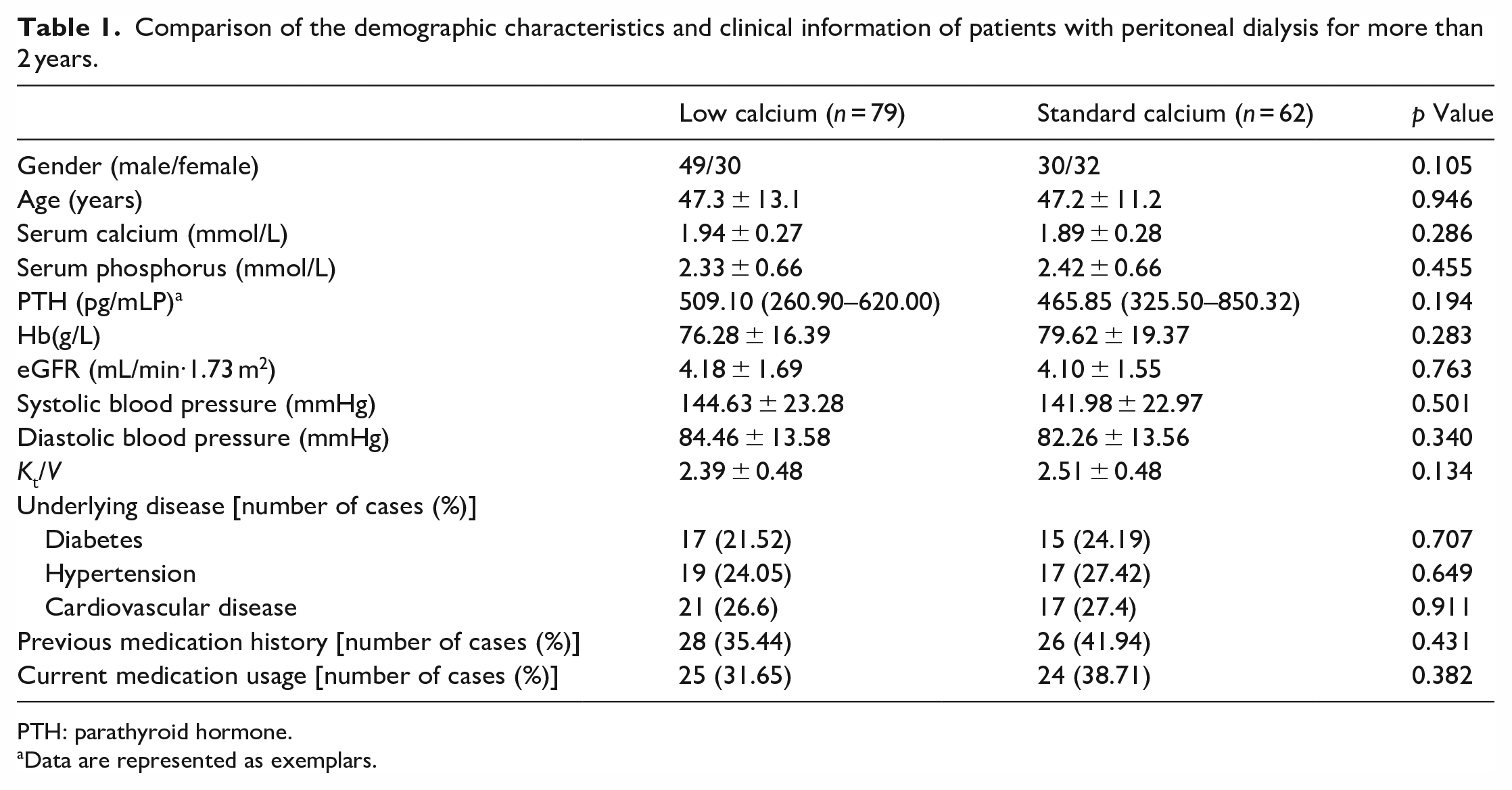
There were 79 patients in the low-calcium group, including 49 males and 30 females, with an average age of 47.3 ± 13.1 years. The standard-calcium group had 62 patients, including 30 males and 32 females, with an average age of 47.2 ± 11.2 years. There was no significant difference in gender, age, underlying diseases, previous medication history, current medication usage and the pre-dialysis residual renal function, serum calcium, phosphorus, PTH, Hb, systolic blood pressure, diastolic blood pressure, Kt/V and cardiovascular disease between the two groups (p > 0.05; Table 1), indicating that the two groups of patients were otherwise comparable.
Comparison of the demographic characteristics and clinical information of patients with peritoneal dialysis for more than 2 years.
PTH: parathyroid hormone.
Data are represented as exemplars.
Calcium and phosphorus metabolism indices and blood pressure of patients after PD for 2 years
After 2 years of PD treatment, the serum calcium levels of the two groups were significantly higher than those before dialysis (p < 0.05). The serum calcium in the standard-calcium group was higher than that in the low-calcium group (2.41 ± 0.23 vs 2.30 ± 0.21), and the difference was statistically significant (p < 0.05). The serum phosphorus in the two groups was significantly lower than before dialysis (p < 0.05). There was no significant difference in serum phosphorus between the two groups (p > 0.05). The PTH of the patients in the standard-calcium group was lower than before dialysis. After dialysis, the PTH was 360.10 (183.50–780.20) pg/mL in the low-calcium group and 262.25 (120.45–488.37) pg/mL in the standard-calcium group, and the difference between the two groups was statistically significant (p < 0.05). There was no significant difference in the systolic and diastolic blood pressures between the two groups before and after dialysis (p > 0.05; Table 2).
Comparison of calcium and phosphorus metabolism indexes and blood pressure in patients after 2 years of dialysis.
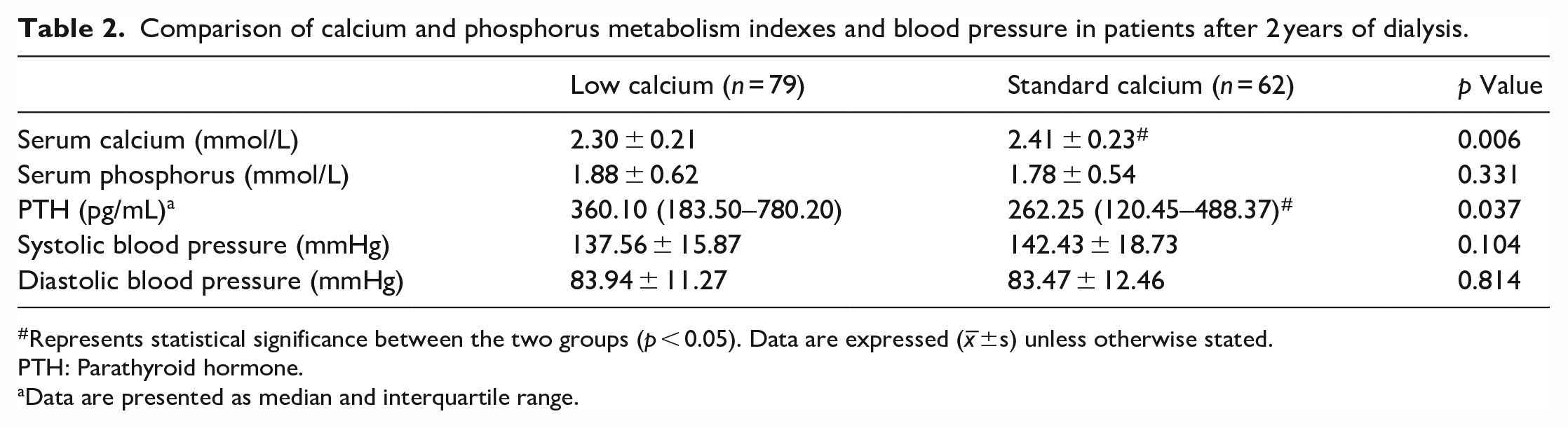
Represents statistical significance between the two groups (p < 0.05). Data are expressed (x–±s) unless otherwise stated.
PTH: Parathyroid hormone.
Data are presented as median and interquartile range.
Comparison of drug use in patients after PD for 2 years
After 2 years of PD, the proportion of patients using phosphate binders in the low-calcium group (59.49%) was significantly higher than that in the standard calcium group (35.48%; p < 0.05), After 2 years of dialysis, the proportion of patients using antihypertensive drugs in the low-calcium group was significantly higher than in the standard calcium group (86.07% vs 70.97%; p < 0.05; Table 3).
Comparison of drug use in patients after peritoneal dialysis for 2 years.

Represents statistical significance between the two groups (P < 0.05). Data are expressed (±s) unless otherwise stated.
Data are represented as exemplars.
Abdominal aortic calcification in patients with PD for 1 year
Because some patients did not undergo a lateral abdominal X-ray after a year on PD, some data were missing. Therefore, 57 patients in the low-calcium group and 56 patients in the standard-calcium group were evaluated for calcification. The overall incidence of abdominal aortic calcification was 50.88% in the low-calcium group and 39.29% in the standard-calcium group. Although the overall incidence of abdominal aortic calcification in the low-calcium group was higher than in the standard-calcium group, the difference was not statistically significant. In addition, there was no significant difference in the degree of calcification of the internal abdominal aorta between the two groups (p > 0.05; Table 4).
Abdominal aortic calcification in patients with peritoneal dialysis for 1 year.

Carotid arteriosclerosis in patients with PD for1 year
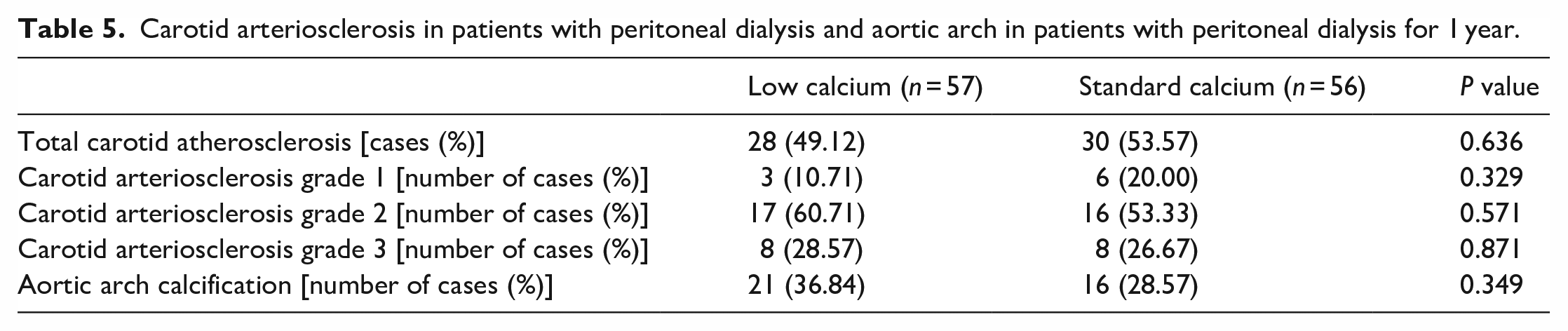
Table 5 shows the incidence of carotid atherosclerosis in patients after a year of PD. The total incidence of carotid atherosclerosis in the low-calcium group was 49.12%, and 53.57% in the standard-calcium group. There was no statistical difference in the incidence or extent of carotid atherosclerosis in the two groups (p > 0.05; Table 5).
Carotid arteriosclerosis in patients with peritoneal dialysis and aortic arch in patients with peritoneal dialysis for 1 year.
Aortic arch calcification in patients after PD for a year
As shown in Table 5, there were 21 (36.84%) cases of aortic arch calcification in the low-calcium group and 16 (28.57%) in the standard-calcium group. There was no statistically significant difference in the incidence of aortic arch calcification between the two groups (p > 0.05).
Discussion
In this study, we found that low-calcium PD fluid maintains the patient’s blood calcium at a slightly lower level in the normal range comparing with standard-calcium PD fluid, while the PTH level and the proportion of patients using antihypertensive drug is higher. Furthermore, the low-calcium PD fluid associates with increasing the proportion of patients using phosphorus-lowering drug. As for the vascular calcification effect of the low and standard calcium PD fluid needs further exploration.
Blood calcium concentrations decreased after dialysis in both low calcium PD and standard calcium groups. We believe it’s about PD helping the overall ion metabolism including calcium. 21 Compared with the standard-calcium group, the serum calcium in the low-calcium dialysate group could be maintained at a low value within the normal range. This suggests that using low-calcium PD fluid may provide more space for calcium-containing phosphate binders, which is consistent with the results reported in the literature. 22
Approximately 70%–80% of the dietary phosphorus intake in adults is excreted by the kidneys. 23 With the loss of renal function, hyperphosphataemia becomes a significant problem. Studies have shown that for every 1 mg/dL increase in serum phosphorus levels, coronary artery calcification increases by 21% and thoracic aortic arch calcification by 33%. 24 In addition, the risk of death in CKD patients increases linearly with increasing serum phosphorus levels. 25 Although PD can remove phosphorus, the protein intake of these patients is significantly higher than before dialysis, with a corresponding increase in phosphorus intake, making them prone to hyperphosphataemia. However, excessive use of calcium-containing phosphate binders can increase the patient’s calcium burden. Studies have shown that using low-calcium PD fluid can better control the serum phosphorus levels of patients and more effectively avoid cardiovascular complications.26–28 In this study, the serum phosphorus of the two groups of patients after PD treatment was significantly lower than before, but there was no significant difference in serum phosphorus levels between the two groups. This may be related to the adjustment of phosphate-lowering drugs and active vitamin D medication according to the patient’s blood phosphorus level as per the guidelines to be followed during PD.
Hypocalcaemia, hyperphosphataemia and deficiency of active vitamin D that occur in the progression of renal disease can lead to secondary hyperplasia of the parathyroid glands and elevated PTH levels. Secondary hyperparathyroidism can lead to severe bone damage, anaemia, nervous system damage and cardiovascular disease. 27 Studies have shown that prolonged use of low-calcium PD fluid can aggravate SHPT in patients. 28 This study also found that PTH levels in the low-calcium group were significantly higher than in the standard-calcium group. Moreover, though the serum calcium and PTH levels of the two groups of patients were statistically different, the serum phosphorus level was not statistically different, possibly due to the use of phosphate-lowering drugs. However, the serum phosphorus level cannot be maintained in the normal range by using phosphate-lowering drugs in the low-calcium group; hence, the PTH level cannot be effectively controlled.
Vascular calcification is widespread in patients with CKD. 29 The incidence of vascular calcification in non-dialysed CKD stage V patients is 79%. After 1 year of dialysis treatment, 80% of patients have coronary arteriosclerosis and 60%–70% of patients with stage 5 CKD die of cardiovascular disease. 30 Low-calcium peritoneal dialysate has been reported to delay the progression of vascular calcification. 31 However, the results of this study suggest no significant difference in the incidence or extent of visible abdominal aortic calcification and aortic arch calcification between the low-calcium and the standard-calcium groups. Moreover, the two groups had no significant difference in the incidence and degree of carotid atherosclerosis. It is possible that baseline characteristics, such as the patient’s calcification status before dialysis, affected the results.
Phosphate-lowering therapy, including phosphate-lowering drugs, is crucial for PD patients. In addition, patients with CKD often have renal hypertension, so several antihypertensive drugs are used, 32 increasing the pain and economic burden of medication for patients. Our study found that the use of phosphate-lowering drugs was higher in the low-calcium group than in the standard calcium group, indicating that more patients in the low-calcium group need to use phosphate-lowering drugs to maintain the balance of calcium and phosphorus. There was no significant difference in systolic and diastolic blood pressure between the groups before and after PD. However, after 2 years of PD, the usage and cost of antihypertensive drugs in the low-calcium group were significantly higher than those in the standard-calcium group. According to the pre-dialytic results of serum calcium, phosphorus and PTH, the authors speculate that this may be due to the long-term use of low-calcium PD fluid, aggravating the patient’s secondary hyperparathyroidism and leading to vascular sclerosis (calcification) and reduced vascular compliance, which increased the incidence of transient increase in blood pressure or hypertension, and eventually leads to an increase in the usage of antihypertensive drugs. This study has some limitations. First, this was a retrospective study with a limited sample size. A prospective, double-blind, randomized, controlled trial with a large sample size is needed to verify the results. Second confounding factors such as primary disease, drug treatment and lifestyle may influence serum phosphate and blood pressure and lead to bias in the results of the study. Finally, comparisons of vascular calcification in patients before and after treatment are lacking. Moreover, we should not only examine the calcium score of the abdominal aorta but also use the coronary artery calcium score to evaluate coronary artery calcium in dialysis patients. Future studies will consider these deficiencies, and more rigorous clinical trials will be designed to verify the conclusions.
Conclusion
We found that low-calcium PD fluid may increase the PTH level and the proportion of CKD patients using antihypertensive drug and phosphorus-lowering drug, but the vascular calcification effect of the low and standard calcium PD fluid needs further exploration. This paper provides new evidence for the choice of dialysate for PD, low-calcium dialysate has no outstanding advantages for long term dialysis.
Footnotes
Author contributions
Conception and design of the work: An N and Zhou HS; Data collection: Li XH, Yu XY, Yang HJ, Zhai LP and Huang YH; Supervision: An N and Zhou HS; Analysis and interpretation of the data: Li XH, Yu XY, Yang HJ, Zhai LP and Huang YH; Statistical analysis: An N, Zhou HS and Yao CW; Drafting the manuscript: An N and Zhou HS; Critical revision of the manuscript: An N, Zhou HS and Yao CW; Approval of the final manuscript: all authors.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by National Clinical Key Specialty Construction Project (Institute of Nephrology, Affiliated Hospital of Guangdong Medical University), the Affiliated Hospital of Guangdong Medical University Clinical Research Programme (LCYJ2018C008 and LCYJ2017A002), Science and Technology Development Special Fund Competitive Allocation Project of Zhanjiang City (2021A05083), Science and Technology Planning Project of Zhanjiang City (2018A01040) and the Natural Science Foundation of Guangdong Province (2021A1515011581).
Ethics approval and consent to participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Affiliated Hospital of Guangdong Medical University (PJKT2022-064).