
Abstract
Introduction:
Severe COVID-19 is associated with a dysregulated immune response that usually leads to cytokine release syndrome. This study aimed to compare the use of extracorporeal blood purification therapy (Oxiris®) versus standard continuous renal replacement therapy (CRRT) in critically-ill patients with severe COVID-19.
Methods:
This was a national, multicenter, retrospective study of patients with COVID-19 admitted to the intensive care unit (ICU) between March and October 2020 who required CRRT. Patients were categorized into two groups: Oxiris® CRRT and standard CRRT. The primary outcome was the number of patients alive and ventilator-free at 30-days post-CRRT treatment. Key secondary endpoints included change in inflammatory markers, Sequential Organ Failure Assessment (SOFA) scores, and PaO2/FiO2 ratio at 24- and 72-h post Oxiris® initiation.
Results:
Thirty-five patients received Oxiris® CRRT and 23 patients received standard CRRT. The primary outcome was 31.4% in the Oxiris® group versus 4.3% in the standard CRRT group (adjusted odds ratio 5.97, 95% confidence interval [CI], 0.64–55.6; p = 0.117). In the Oxiris® group, interleukin-6 (IL-6) concentrations significantly decreased at 24 and 72-h (p = 0.033) and PaO2/FiO2 ratio significantly increased at 24 and 72 h after Oxiris® initiation (p = 0.001). There was no significant change in SOFA scores at 24- and 72-h after Oxiris® initiation.
Conclusion:
The number of patients alive and ventilator-free at 30-days was higher in the Oxiris® group than that in the standard CRRT group; however, the difference did not reach statistical significance after adjusting for the baseline severity of illness. There was a significant reduction in IL-6 and significant improvement in PaO2/FiO2 ratio after Oxiris® CRRT initiation.
Introduction
One of the hallmarks of severe coronavirus disease (COVID-19) is a dysregulated immune response against severe acute respiratory syndrome coronavirus 2. 1 The dysregulation in immune response usually leads to cytokine release syndrome (CRS), which can result in several complications that include acute respiratory distress syndrome, septic shock, intractable metabolic acidosis, coagulation dysfunction, and multiple organ failure. 1
Several large randomized controlled trials have demonstrated the effectiveness of immunomodulatory therapies such as corticosteroids, tocilizumab (interleukin-6 inhibitor), and baricitinib (Janus tyrosine kinase [JAK] inhibitor) in reducing mortality and improving outcomes in patients with severe COVID-19 pneumonia.2–4 Currently the World Health Organization and National Institute of Health guidelines recommend the use of dexamethasone and immunomodulatory drugs in patients with severe COVID-19. 5
Acute kidney injury (AKI) is common in critically ill patients hospitalized with COVID-19 with incidence ranging 6%–78%.6,7 The incidence of AKI requiring kidney replacement therapy ranges between 6% and 73% in critically ill patients with COVID-19.6 –8 The most common modality used for renal replacement therapy (RRT) in critically ill patients with COVID-19 is continuous renal replacement therapy (CRRT; 52.4%). 8 The Oxiris® filter (Baxter, IL, USA) is a heparin-coated hemofilter that is also used for CRRT. 9 Extracorporeal blood purification (ECBP) using Oxiris® unselectively removes cytokines and endotoxin. 10 The Food and Drug Administration has approved Oxiris® filter for the treatment of severe COVID-19 under an emergency use authorization. 9 Few studies have evaluated the efficacy of ECBP therapy using Oxiris® in critically ill patients with COVID-19.10–15 These studies have shown a significant decrease in inflammatory markers as well as a significant decrease in organ dysfunction scores with the use of Oxiris® filter.10 –14 However, most of these studies were limited by the small sample size and the lack of a comparator group.
This study aimed to evaluate the use of Oxiris® compared to standard CRRT in critically ill COVID-19 pneumonia patients with AKI requiring CRRT.
Materials and methods
This was a national, multicenter, retrospective cohort study that included critically ill patients with COVID-19 pneumonia requiring CRRT. This study compared the efficacy of CRRT and ECBP therapy using Oxiris® filter to that of standard CRRT in critically ill patients with COVID-19. The study period was between March and October 2020. This study was approved by the Hamad Medical Corporation Institutional Review Board (MRC-01-20-1117).
The inclusion criteria were as follows: (1) age >16 years, (2) positive COVID-19 polymerase chain reaction results, and (3) intensive care unit (ICU) admission. The exclusion criteria were as follows: (1) pregnancy or (2) use of a CytoSorb filter.
The primary outcome was the number of patients who survived and were ventilator-free after 30 days of treatment. Secondary outcomes were in-hospital mortality, 30-day mortality, time to death from treatment initiation, ICU duration of stay (DOS), hospital DOS, change in sequential organ failure assessment (SOFA) score at 24 and 72 h, and change in the ratio of oxygen partial pressure to fractional inspired oxygen (PaO2/FiO2) at 24 and 72 h. Other outcomes included changes in inflammatory markers, including C-reactive protein, D-dimer, ferritin, and interleukin-6 at 24 and 72 h, and filter clotting/clogging.
The data collected included baseline demographics and medical histories. Laboratory data were collected at baseline and at the initiation of CRRT and 24 and 72 h after CRRT initiation. Inflammatory markers and baseline neutrophil, lymphocyte, platelet, and lactate levels were also assessed. SOFA scores were collected at baseline, initiation of CRRT, and 24 and 72 h after CRRT initiation. The data on the level of respiratory support was collected at ICU admission, initiation of CRRT, and 24 and 72 h after CRRT initiation.
CRRT was initiated in critically ill patients who had an indication for RRT by the primary team. An ECBP utilizing Oxiris® was used based on filter availability. Nephrology services were consulted for CRRT initiation, and the initial effluent dose was 25–30 mL/kg/h.
Statistical analysis
Baseline characteristics, inflammatory markers, and primary and secondary endpoints are presented as mean ± standard deviation for normally distributed data or median (interquartile range) for non-normal continuous data, and number (%) for categorical data. Mann-Whitney U test was used to compare non-normally distributed continuous data between the two group. Wilcoxon signed-rank test and Friedman test were used for non-normally distributed continuous data before and after the Oxiris® CRRT. Chi-squared test or Fisher’s exact test was used to compare categorical data.
The primary outcome was adjusted for the SOFA score at the time of treatment initiation. Multivariable logistic regression was used for the adjustment. For patients who died within 24 and 72 h of CRRT initiation, the maximum SOFA score (24) was used at these time points, respectively. Two-sided p-values less than 0.05 were considered statistically significant. Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 27.0 (IBM Corp, Armonk, NY).
Results
Of 63 patients assessed for eligibility, 58 met the inclusion criteria. Five patients were excluded because they were started on the CytoSorb filter. Thirty-five patients received Oxiris® and 23 patients received standard CRRT. The median age was 58 years (interquartile range [IQR], 48–69.25) years and 75.9% of the patients were males. Only eight patients had a history of end-stage renal disease and were receiving RRT prior to admission, while 27.6% had a history of chronic kidney disease. The most common comorbidities were hypertension and diabetes mellitus (63.8% and 55.2%, respectively). Most patients were of Asian (51.4%) and Middle Eastern (45.7%) ethnicities. The baseline characteristics are summarized in Table 1. The median duration from admission to Oxiris® initiation was 11 (IQR, 7–17) days.
Patient characteristics at baseline and ICU admission.
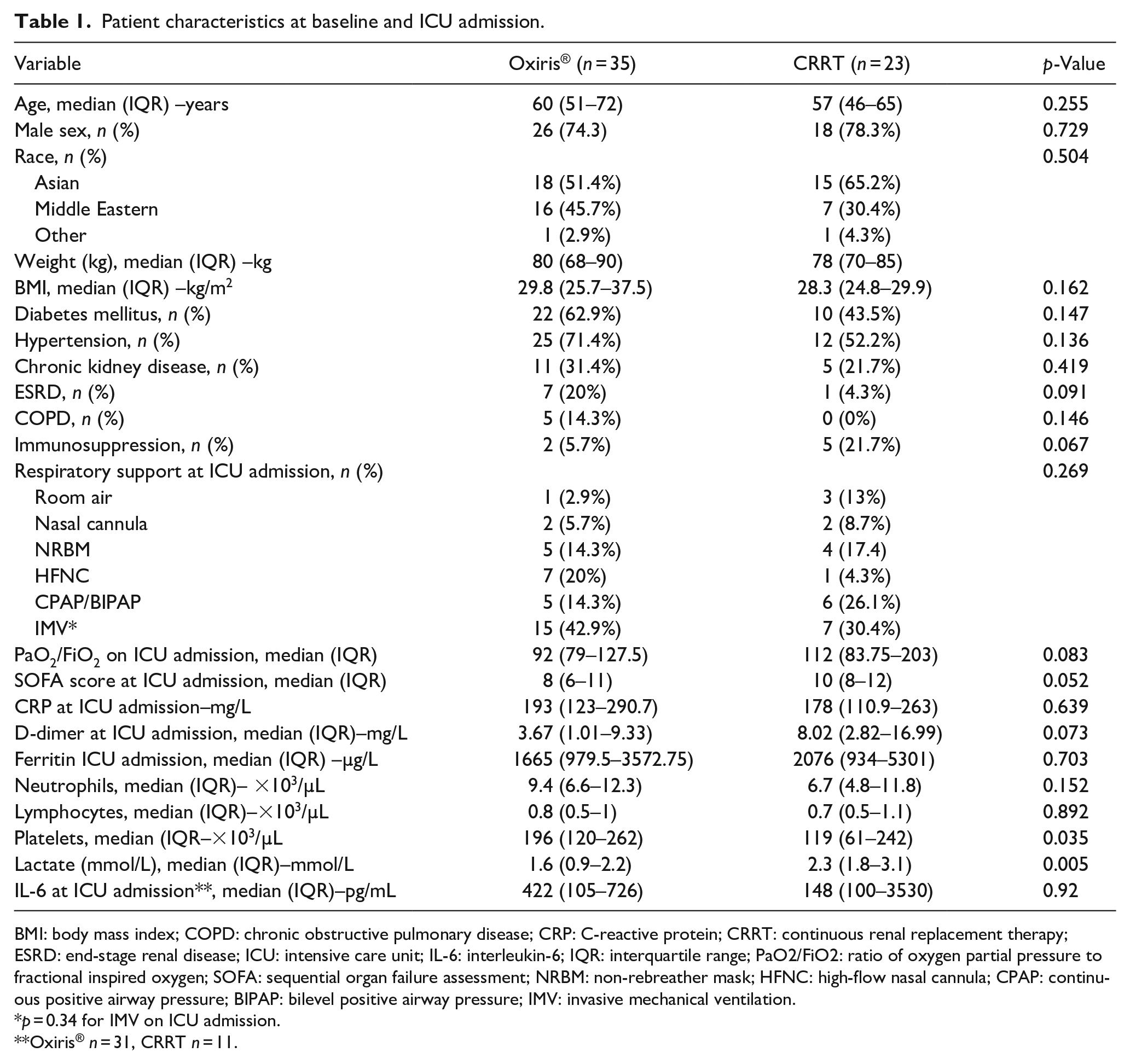
BMI: body mass index; COPD: chronic obstructive pulmonary disease; CRP: C-reactive protein; CRRT: continuous renal replacement therapy; ESRD: end-stage renal disease; ICU: intensive care unit; IL-6: interleukin-6; IQR: interquartile range; PaO2/FiO2: ratio of oxygen partial pressure to fractional inspired oxygen; SOFA: sequential organ failure assessment; NRBM: non-rebreather mask; HFNC: high-flow nasal cannula; CPAP: continuous positive airway pressure; BIPAP: bilevel positive airway pressure; IMV: invasive mechanical ventilation.
p = 0.34 for IMV on ICU admission.
Oxiris® n = 31, CRRT n = 11.
Continuous veno-venous hemodiafiltration (CVVHDF) was the most common treatment modality (n = 50, 86.2%). The use of CVVHDF was similar between the two groups (Oxiris®: 85.7% vs. standard CRRT: 85.7%, p = 0.97). The median initial blood flow rate was 150 (IQR, 150–150) mL/min. The median initial pre-blood pump fluid replacement rate was 250 (IQR, 250–500) mL/h, median initial dialysate rate was 750 (IQR, 750–1000) mL/h, and median initial post-filter fluid replacement rate was 500 (IQR, 250–500) mL/h. The initial CRRT modalities and their characteristics are summarized in Table 2.
CRRT modalities, patient characteristics, inflammatory markers, and COVID-19 therapeutics at treatment initiation.
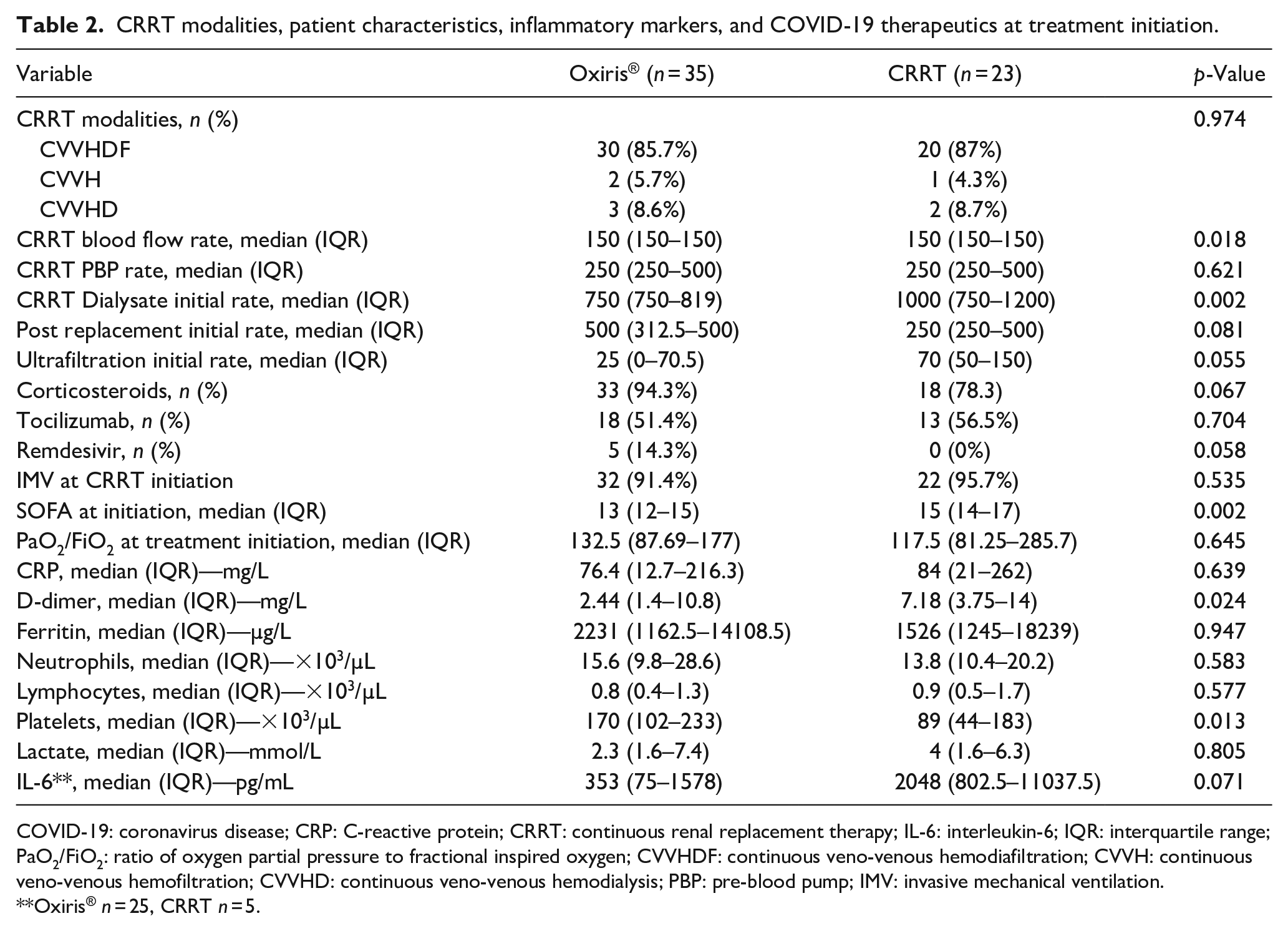
COVID-19: coronavirus disease; CRP: C-reactive protein; CRRT: continuous renal replacement therapy; IL-6: interleukin-6; IQR: interquartile range; PaO2/FiO2: ratio of oxygen partial pressure to fractional inspired oxygen; CVVHDF: continuous veno-venous hemodiafiltration; CVVH: continuous veno-venous hemofiltration; CVVHD: continuous veno-venous hemodialysis; PBP: pre-blood pump; IMV: invasive mechanical ventilation.
Oxiris® n = 25, CRRT n = 5.
Overall, corticosteroids were administered to 51 patients (87.9%), and 53.4% received tocilizumab. Invasive mechanical ventilation was provided as respiratory support at ICU admission in 42.9% of patients in the Oxiris® group compared to 30.4% in the standard CRRT group, and 91.4% of patients in the Oxiris® group received invasive mechanical ventilation at the initiation of RRT compared to 95.7% in the standard CRRT group. The PaO2/FiO2 ratio was similar between the two groups; however, the median SOFA score was higher in the standard CRRT group at treatment initiation (p = 0.002). Table 2 summarizes CRRT modalities, patient characteristics, inflammatory markers, and COVID-19 therapeutics at treatment initiation.
For the primary outcome, 31.4% (n = 11) in the Oxiris® group were alive and ventilator-free at 30 days compared to 4.3% (n = 1) in the standard CRRT group with an adjusted odds ratio of 5.97 (95% confidence interval, 0.64–55.6; p = 0.117).
The 30-day mortality was 60% in the Oxiris® group compared to 78.3% in the standard CRRT group (p = 0.147). Hospital DOS was similar between the two groups. Patients in the CRRT group had a significantly greater reduction in the SOFA score at 24 h than those in the Oxiris® group, but the change in SOFA score at 72 h was not significantly different between the two groups. There were no significant differences in other secondary outcomes (Table 3).
Secondary outcomes.
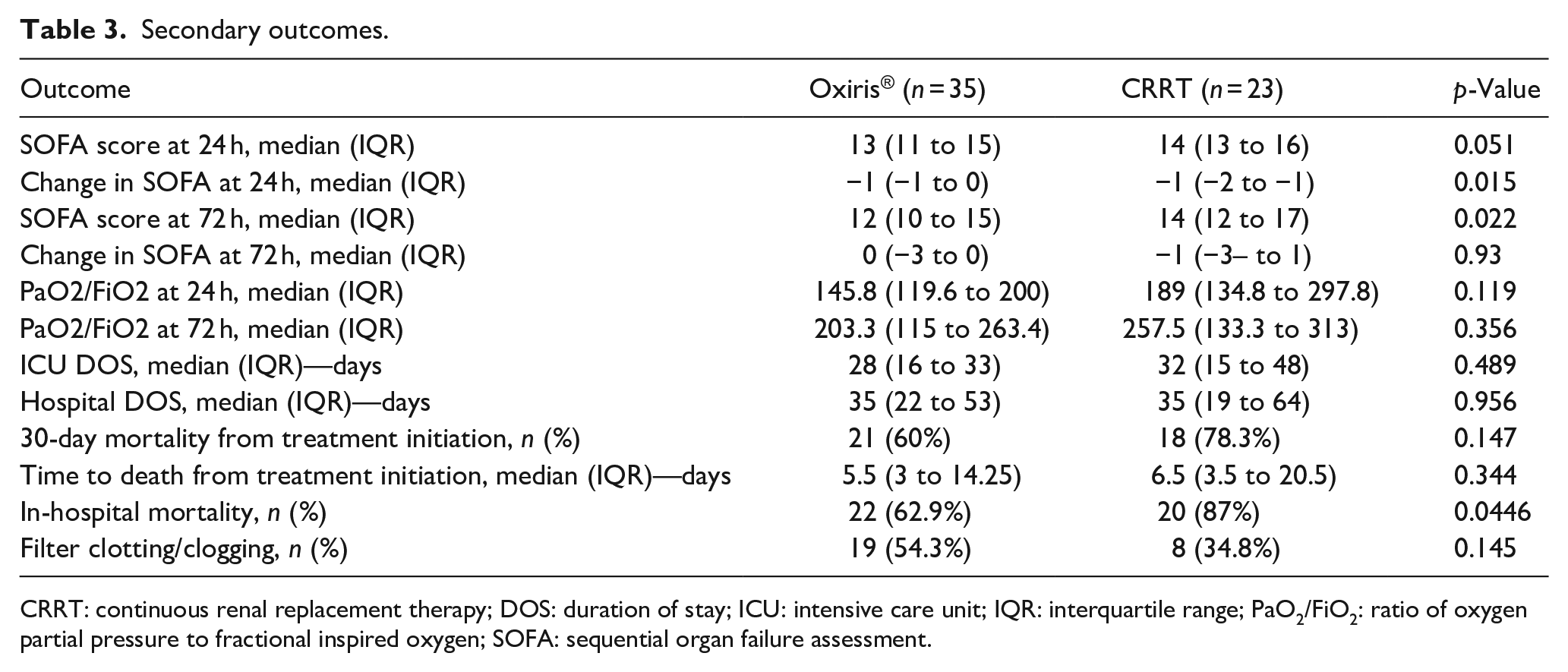
CRRT: continuous renal replacement therapy; DOS: duration of stay; ICU: intensive care unit; IQR: interquartile range; PaO2/FiO2: ratio of oxygen partial pressure to fractional inspired oxygen; SOFA: sequential organ failure assessment.
Changes in inflammatory markers before and after initiation of therapy were assessed in the Oxiris® group. IL-6 levels significantly decreased at 24 and 72 h after the initiation of treatment. The median C-reactive protein level decreased from 110 mg/dL at treatment initiation to 46 mg/dL at 72 h. Changes in inflammatory marker levels are shown in Table 4.
Change in disease severity and inflammatory markers at 24 and 72 h in the Oxiris® cohort.
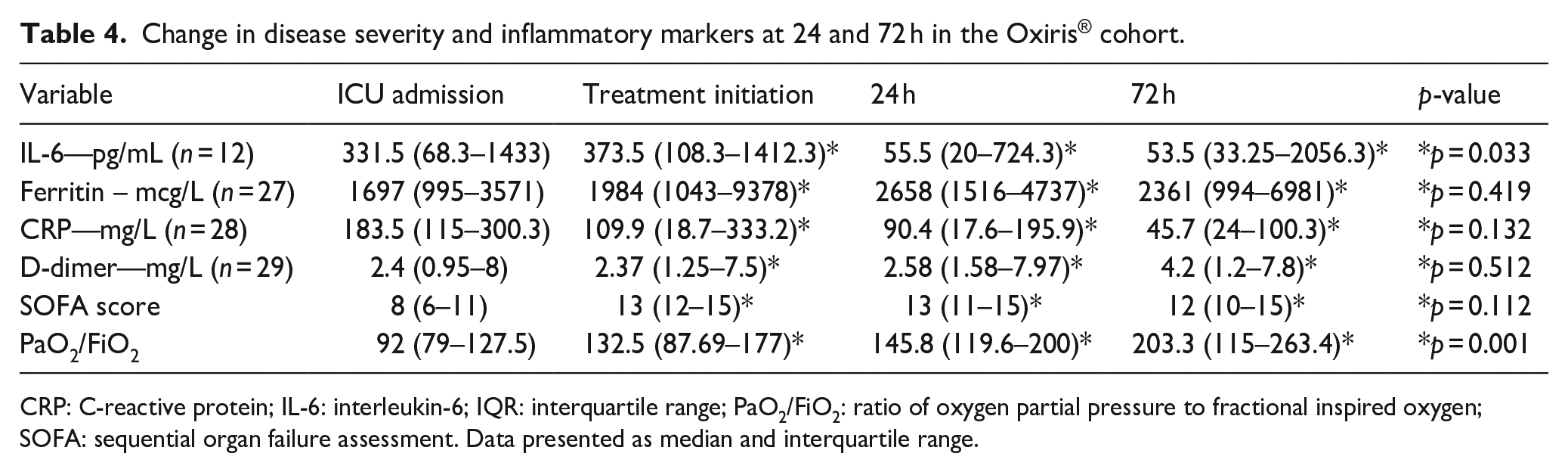
CRP: C-reactive protein; IL-6: interleukin-6; IQR: interquartile range; PaO2/FiO2: ratio of oxygen partial pressure to fractional inspired oxygen; SOFA: sequential organ failure assessment. Data presented as median and interquartile range.
The median PaO2/FiO2 ratio was 146 (IQR, 119.6–200) at 24 h and 203 (IQR, 115–263) at 72 h compared to 132 (IQR, 88–177) at the Oxiris® initiation (p < 0.001 and p = 0.004, respectively). There was no difference in SOFA scores at 24 and 72 h compared to the SOFA score at Oxiris® initiation.
Discussion/conclusion
This national, multicenter, retrospective study compared the use of Oxiris® to standard CRRT in critically ill patients with COVID-19 pneumonia. After adjusting for baseline organ dysfunction score, was no statistically significant difference in the percentage of patients who were alive and ventilator-free at 30 days after treatment initiation; however, the percentage was higher in the Oxiris® group (31.4%) than that in the standard CRRT group (4.3%). The 30-day mortality rate from treatment initiation was also lower in the Oxiris® group (60%) than that in the standard CRRT group (78.3 %).
The mortality in critically ill patients with COVID-19 pneumonia requiring CRRT ranges from 63% to 64.1% and up to 71.6% in critically ill patients requiring invasive mechanical ventilation, vasopressors, and RRT, which is similar to the overall mortality in this study, which was 67.2%.6,8,16
Mortality in the Oxiris® group was similar to that reported by Villa et al. (56.4%).13 The decrease in inflammatory markers after the initiation of Oxiris® treatment in this study was similar to that reported in other studies. A significant decrease in IL-6 was observed at 24, 48, and 72 h, which is consistent with the findings of this study. We also observed a significant increase in PaO2/FiO2 ratio at 24 and 72 h after Oxiris® initiation, which is similar to the findings by Premužić et al. 10
In contrary to our study findings, the SOFA score significantly decreased at 24, 48, and 72 h in the studies by Villa et al. and Premužić et al.10,13 This difference in results can be explained by the difference in the patient population between the two studies, such as all the patients included in our study had AKI or end-stage renal disease and required CRRT compared to 70.3% in Villa et al.’s cohort and 46.7% in the study by Premužić et al.10,13 Additionally, the median duration to Oxiris® initiation was 11 days compared to 3.6 and 3.2 days in the study by Villa et al. and Premužić et al., respectively.10,13
Kang et al. 15 did not observe a significant decrease in IL-6 in the Oxiris® group compared to the control group. Unlike our study as well as other published studies, the patient included in the study by Kang et al. did not have AKI and was started on CRRT with Oxiris® filter for ECBP.10 –15 Additionally, the median baseline IL-6 at admission was 13.88 pg/mL, and the mean at day 1 was 3.41 pg/mL. The large difference in IL-6 levels between admission and on day 1 could not be explained by the authors. The authors did not report the duration from admission to the initiation of Oxiris®. Other vital information such as the use of corticosteroids or immunomodulators was not presented by the authors. All the aforementioned reasons limit the ability to extrapolate or compare the results of the study by Kang et al. 15 to ours and the available literature.
Most patients in this study received corticosteroids (88%), and 53% received tocilizumab. This highlights the additional benefit of using the Oxiris® filter in critically ill patients with AKI who require CRRT. The majority of previous studies did not report corticosteroid or tocilizumab use.11,12,14,15 Villa et al. 13 reported that none of the included patients received corticosteroids, and 40.5% received tocilizumab. Premužić et al. 10 reported 100% use of corticosteroids but did not report the use of other immunomodulators.
Study limitations
As previously mentioned, the median duration to Oxiris® initiation was 11 days, which was longer than that reported in other studies. This may explain the lack of improvement in SOFA scores at 24 and 72 h. Several studies have reported improved outcomes with early initiation of ECBP in critically ill patients with COVID-19 pneumonia. The baseline SOFA score was higher in the control group; however, we attempted to control for differences by adjusting the primary outcomes for the SOFA score at treatment initiation. The small sample size is also one of the main limitations of this study, but our data are unique as they represent a direct comparison between Oxiris® and standard CRRT, which should pave the way for a more robust randomized controlled trial. Other limitations include the retrospective design of the study, being a single health system experience, missing data on inflammatory markers at 24, 48, and 72 h after Oxiris® initiation, and inability to adjust for the use of COVID-19 directed therapies prior to initiation of RRT because of small sample size.
Conclusion
After controlling for baseline organ dysfunction score, there was no significant difference in the percentage of patients who were alive and ventilator-free at 30 days between the Oxiris® and standard CRRT groups; however, the percentages were numerically higher in the Oxiris® group. There were significant improvements in IL-6 levels and the PaO2/FiO2 ratios after the initiation of ECBP using Oxiris®. Further well-powered randomized controlled trials are needed to evaluate ECBP using Oxiris® compared with standard CRRT.
Footnotes
Author contributions
All the authors contributed substantially to the conception and design of the study. AM, MA, MS, and HM contributed substantially to data acquisition and analysis. AM, MA, MS, and HM made substantial contributions to data interpretation. AM, MA, MS, and HM drafted the manuscript. All the authors revised the manuscript substantially. All the authors have read and approved the final manuscript for publication.
Data availability statement
All data generated or analyzed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Hamad Medical Corporation Medical Research Centre.