
Abstract
In recent years, normothermic machine perfusion (NMP) has emerged in conversation surrounding organ preservation and transplantation techniques with the goal of improving patient and clinical outcomes. This is in great attempt to address the rate of non-utilization and the shortage of available organs in kidney transplantation. This focus in mind, normothermic perfusion presents itself as a potential tool to mimic physiological conditions and improve current preservation methods, such as static cold storage. This review serves to improve understanding of the observed connection between the consequences of ischemia and reperfusion injury and traditional preservation techniques as well as how renal NMP may mitigate these issues. Previous studies suggest that reducing time in static cold storage methods by promoting the normothermic perfusion model results in decreased delayed graft function and post-transplant complications. This review also aims to present the immense clinical potential NMP has on future kidney transplantation success and what this means for the fields of nephrology and transplantation. While great strides have been made to evaluate normothermic perfusion’s impact on kidney graft viability and transplant success, future research into unified protocol, clinically relevant biomarkers, cost-utility analysis, and use with associated therapeutic and imaging modalities is paramount.
Highlights
The organ supply shortage is a major challenge facing the field of organ transplantation. Normothermic machine perfusion (NMP) has emerged in a growing conversation surrounding organ preservation and transplantation techniques with the goal of improving patient and clinical outcomes.
Growing evidence suggests NMP as a promising new mechanism to improve post-transplantation kidney success and improve patient outcomes. As the shortage of available organs for kidney transplantation only worsens, normothermic perfusion has taken center focus as a potential mitigation tool to mimic physiological conditions and improve current preservation methods, such as static cold storage.
Currently there is no nationally-available NMP kidney pump system that can replicate the improved kidney transplant outcomes. Thus, such a platform for kidneys is of great national importance to assess true organ viability, and it could allow for rehabilitation and rescue of those organs before transplant.
Although multiple aspects of NMP prove promising, great variation still exists amidst protocol and practice leaving behind limitations to the feasibility of NMP becoming common clinical practice.
Introduction
Transplant nephrology has faced an increasing demand for innovative practices to optimize kidney graft success. The high rate of discard in kidney transplantation has created discussion on improving transplant outcomes of kidneys from expanded criteria donors (ECD) and donation after circulatory death (DCD).1,2 Growing research suggests that expanding the criteria for optimal kidney donation increases survival rates amongst waiting kidney recipient candidates 3 although this presents an increased risk for graft loss. 4 At a lower estimated longevity rate and a greater risk of warm ischemia (WI) time, complications associated with ECD kidneys are unavoidable consequences. 5 Ischemia and reperfusion injury (IRI) is also relevant to the discussion, a process causing great disturbance to the natural performance and physiological processes of the kidney allograft.6–10 The effects of total ischemia time are shown to be exacerbated by other donor characteristics such as age. In a comprehensive database study, Wong et al demonstrated a significantly greater interaction of over 14 h of total ischemia time on graft loss with increased donor age. 11 This multifactorial complexity requires innovation in therapeutic approaches to improve ischemia time in organ transplantation.
Normothermic machine perfusion (NMP) of the kidney, often referred to as ex-vivo normothermic perfusion (EVNP), or normothermic ex-vivo kidney perfusion (NEVKP) has been studied as a possible tool to mitigate ECD-associated complications.12,13 This perfusion method holds further possibilities with respect to the procurement, transplantation, and post-transplantation success. As a preservation technique, NMP mitigates the presentation of ischemia-related complications often seen in grafts preserved via static cold storage (SCS).14–16 Thus, NMP can promote kidney function and suppress consequences related to SCS. As a potentially new assessment tool, NMP may serve as a more accurate screening mechanism to assess graft potential and viability, and lower the number of discarded kidneys at risk for delayed graft function (DGF) and graft failure.13,17–22 Beyond these boundaries, NMP may also serve as a reconditioning mechanism.23,24 Given these possibilities, a better understanding of not only NMP, but its relation to involved pre- and post-transplantation complications will allow for improved patient outcome within multiple domains.
NMP contrasts with the standard mechanism of SCS as well as hypothermic machine perfusion (HMP). Variations of machine kidney perfusion exist including: hypothermic perfusion, sub-normothermic perfusion (SNMP), and NMP. Comparisons of each variation also help to differentiate NMP from SCS. Although differing protocol exists when conducting NMP, it serves as a technique establishing near-physiological temperature conditions.19,22,25–31 This temperature prevents drastic disruption of cellular metabolic processes. 23 Interest in utilizing NMP following other preservation techniques, such as SCS is also rising with studies demonstrating potential efficacy in graft repair. Studies also suggest NMP is an effective method on its own. 17
Large animal models, including both human and porcine kidney model studies, are used in pretransplant NMP protocols to assess clinical and functional outcomes for recipients.19,21,22,27,28,30–33 Recently, a study from Mazilescu et al. 28 demonstrated that among DCD kidneys, patients in the NMP group (in which NMP was preceded by deoxygenated HMP) had a lower incidence of DGF compared to that of the control group undergoing only anoxic HMP.
Hence, NMP promises innovation within the field of solid organ transplantation and boasts a promising future in improving the organ utilization rate and advancing transplantation outcomes. Despite the ongoing research of NMP, further studies are necessary to establish standardizable protocol before common practice. A conclusive understanding of the key biomarkers to analyze during NMP as well as the composition of perfusate solutions is also lacking. The scarcity of NMP kidney studies in the United States highlights the further need for research in this domain. Therefore, the aim of this review is to present the state of NMP in its current and future capability, and potential applications within clinical practice in the domains of organ assessment, preservation, and kidney reconditioning. Literature searches were conducted in PubMed using the search strategy summarized in Supplemental Table 1. A detailed examination of NMP protocol characteristics, and recently published findings are shown in Tables 1 and 2, respectively.
Recent clinical models of NMP, respective protocols, and perfusion characteristics.
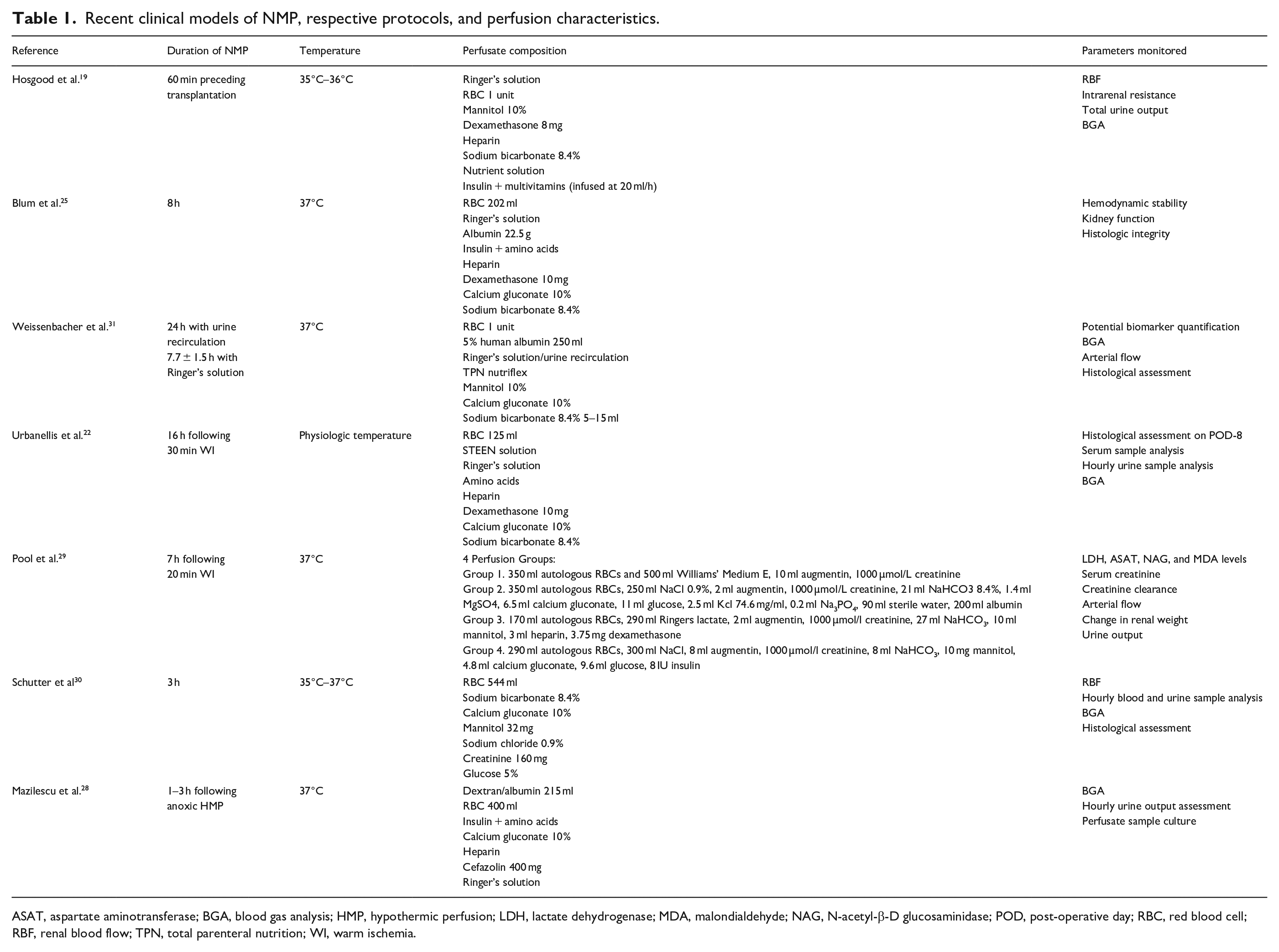
ASAT, aspartate aminotransferase; BGA, blood gas analysis; HMP, hypothermic perfusion; LDH, lactate dehydrogenase; MDA, malondialdehyde; NAG, N-acetyl-β-D glucosaminidase; POD, post-operative day; RBC, red blood cell; RBF, renal blood flow; TPN, total parenteral nutrition; WI, warm ischemia.
Normothermic perfusion models: Graft success and recipient outcomes.
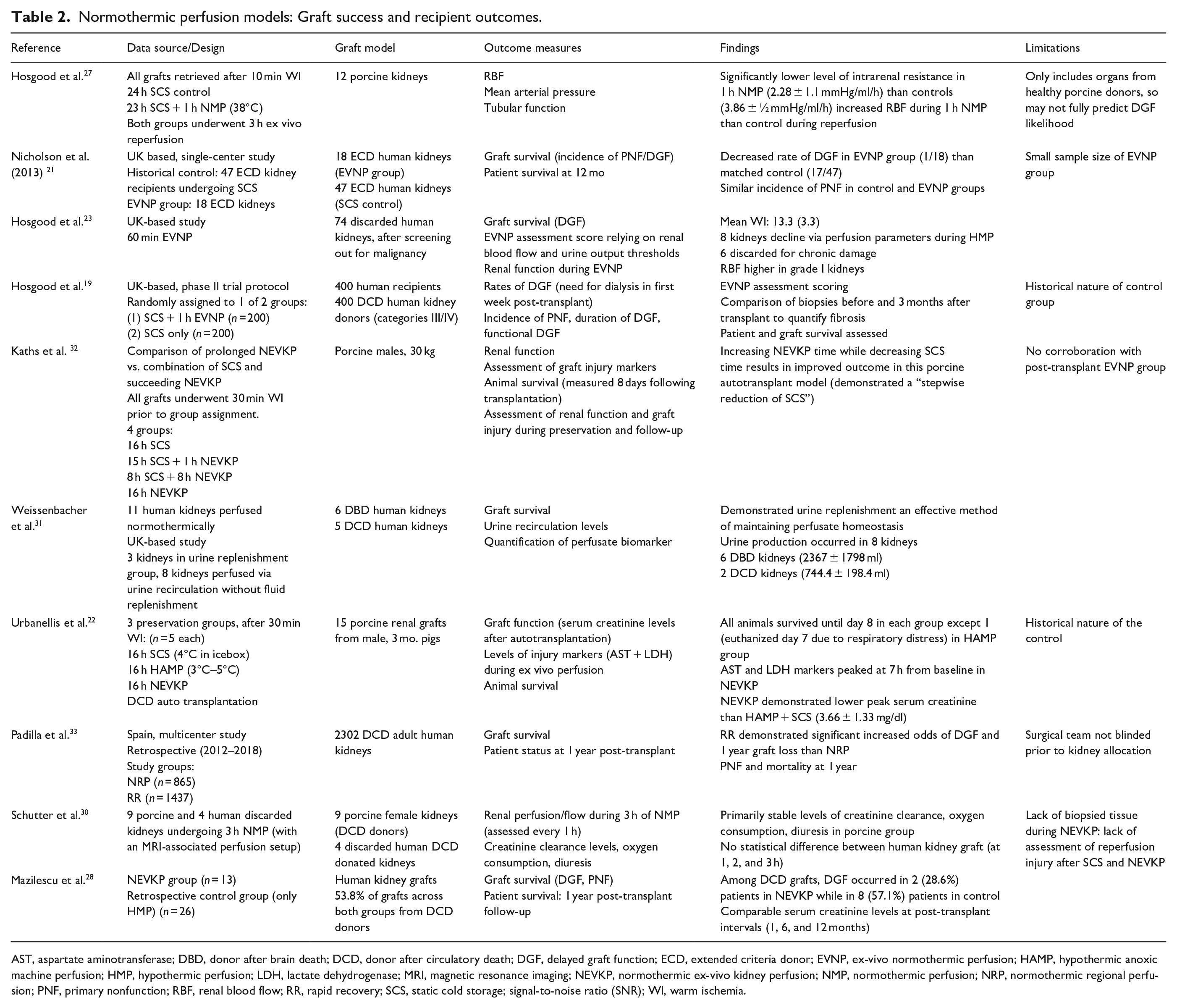
AST, aspartate aminotransferase; DBD, donor after brain death; DCD, donor after circulatory death; DGF, delayed graft function; ECD, extended criteria donor; EVNP, ex-vivo normothermic perfusion; HAMP, hypothermic anoxic machine perfusion; HMP, hypothermic perfusion; LDH, lactate dehydrogenase; MRI, magnetic resonance imaging; NEVKP, normothermic ex-vivo kidney perfusion; NMP, normothermic perfusion; NRP, normothermic regional perfusion; PNF, primary nonfunction; RBF, renal blood flow; RR, rapid recovery; SCS, static cold storage; signal-to-noise ratio (SNR); WI, warm ischemia.
Ischemia and reperfusion injury and its relation to preservation/storage techniques
Pathophysiology of ischemia and reperfusion injury
To optimize therapeutic approaches in mitigating kidney IRI and its resulting transplant consequences, it is important to acknowledge its complexity. Ischemia is the discontinuance of blood flow to a particular organ or tissue and reperfusion injury is the organ damage succeeding re-establishment of perfusion. 7 While ischemia and reperfusion injury are not solely associated with organ transplantation and post-operative kidney outcomes, substantial research exists to strengthen knowledge of this connection. This research focuses on a goal to understand the molecular and cellular effects of IRI. Most notably, IRI affects total protein (TP) levels thereby resulting in a lack of ATP re-synthesis which cascades into energy depletion in the injured tissue or organ. This ATP depletion is preceded by an abnormally high production of reactive oxygen species (ROS) within the injured tissue. 9 An additional hallmark of IRI relates to the distinct isoforms of nitric oxide synthase (NOS), the enzyme responsible for the synthesis of nitric oxide (NO). Its isoform inducible NOS (iNOS) produces free radicals in hypoxic cells and works as a toxic agent that elicits an adverse kidney response while endothelial NOS (eNOS) causes vasodilation and serves as a reno-protective enzyme. 9 Previously, Chatauret et al. 34 demonstrated that HMP is better than SCS at improving microcirculation via stress-induced NO release by increasing activation of eNOS phosphorylation, in turn showing that machine perfusion is a valuable tool for preserving the reno-protective capability of the NO signaling pathway. The cellular effects of IRI are also marked by a substantial and adverse increase in intracellular ion levels of calcium (Ca2+) and sodium (Na+). 7 Additional research is concerned with the influence of regulated cell death pathways on tubular cell death in IRI, such as ferroptosis. 35 Remaining largely unknown, these regulated cell death pathways are focus points for ongoing research surrounding kidney IRI and transplant outcomes.
Consequences of ischemia and reperfusion injury on kidney transplant outcomes
IRI is a significant factor in kidney transplant outcomes. IRI-specific implications on the kidney, of the most serious, include acute kidney injury (AKI), delayed graft function (DGF), and damaging activation of innate immunity. DGF is caused by the combination of ischemia and reperfusion. Ischemia makes renal cells vulnerable to oxidative stress. Reperfusion supplies oxygen to the kidney, but it causes inflammation via a white blood cell and cytokine response, and induces oxidative stress in renal cells.9,10 Lindeman et al. 36 demonstrated that DGF is preceded by a post-reperfusion metabolic collapse using a comparative analysis of biopsied human tissue and arterio-venous blood sample before and after reperfusion. Episodes of AKI following IRI can very rapidly progress to chronic kidney disease (CKD), and this is a complex, yet important mechanistic transition that requires identification and exploration for potential therapeutic innovations with NMP.37,38 Activation of innate immunity, which plays a crucial role in inflammation, is guided by toll-like receptors (TLRs). TLRs are upregulated by AKI, but they also recognize endogenous molecules known as damage-associated molecular patterns (DAMPs) that are released by cells of injured tissues. 10 Improper activation of innate immunity is a complicated IRI-related consequence to control with pre-transplant intervention; however, growing investigation is emerging into potential therapeutic strategies. 39
Mitigation of renal consequences from ischemia and reperfusion injury
There are multiple options to minimize allograft injury throughout the transplantation process with respect to donor and recipient management prior to transplantation and graft management during the storage/preservation period. This includes graft reconditioning which consists of a determined time of WI for the donor graft to undergo, adequate perfusion of the graft, and ensured proper hydration of the recipient to prevent hypovolemia post-transplant. 10
Specific benefits of NMP as they relate to IRI and other techniques such as SCS or HMP include decreasing CIT, restoring ATP depletion, and decreasing apoptotic and oxidative distress markers. 40 Hamar et al. 8 demonstrated that porcine kidneys with 8 h NMP had lower serum creatinine levels and lower tubular injury and inflammation scores following perfusion compared to the groups without preservation or static cold storage. Results also suggest the possibility of additional strategies administered in concordance with NMP. For example, Lohmann et al. 41 demonstrated the use of mesenchymal stromal cells (MSCs) on a porcine kidney model undergoing 240 minutes of NMP, concluding that administration of these cells during perfusion had no harmful effect on other perfusion factors. The use of MSCs with NMP is noteworthy in that these cells induce anti-inflammatory effects directly at the site of tissue injury, potentially helping to mitigate the detrimental effects of kidney IRI. In a similar therapeutic strategy, Thompson et al. demonstrated the use of Multipotent Adult Progenitor Cells (MAPC) as a potential tool to modulate the effects of IRI in declined human kidneys that were not transplanted. Outcome measures occurred ex vivo and compared to the control group, kidneys receiving MAPC treatment demonstrated improved urine output, decreased levels of the injury marker, NGAL, and downregulation of interleukin (IL)-1β. 42 These types of cellular therapy techniques are pivotal for advancing the clinical understanding of kidney NMP. The assessment of metabolic homeostasis and the emphasis on optimal metabolic support during NMP is of pivotal importance to ensuring graft quality. 43
Normothermic machine perfusion technique
Temperature conditions
NMP is of significant value to the future of kidney transplantation because it provides near-physiologic conditions (35°C–37°C).19,22,25,28,30,31 Differing from SCS and HMP (4°C), NMP can support optimal metabolic function by ensuring the replenishment of ATP and preventing ischemic injury.20,26 In sub-physiological temperature conditions, the depletion of ATP by means of reduced metabolic function which in turn, slows or inactivates additional cellular processes. Table 1 shows the temperature conditions chosen in recent clinical studies.
Perfusate composition
While perfusate composition varies amongst currently published protocols (Table 1), major commonalities still exist. Typically, the perfusate for NMP contains an oxygen carrier, priming solution, fluid replacement, a colloid, nutrient supplementation, anticoagulant, and protective additives. 26 In a porcine kidney model, Pool et al. 29 demonstrated use of varying volumes of red blood cells (RBCs) ranging from 350 to 170 ml among their four different perfusion solution groups (Table 1) undergoing 7 h of NMP. They assessed variation in the levels of injury marker N-acetyl-β-D glucosaminidase (NAG), NMP flow patterns, and thiobarbituric acid reactive substance levels amongst each perfusion group. They further emphasized that varying perfusate composition affects interpretation of perfusion parameters. 29 NMP can also be conducted with or without urine recirculation. In studies demonstrating feasibility of urine recirculation, Ringer’s lactate solution is the chosen solution for fluid replacement.19,31 We-issenbacher et al. 31 compared perfusion of human kidneys in a urine replenishment group (n = 3) and a urine recirculation group without urine replenishment (n = 8) and showed that urine recirculation provides an effective method of maintaining perfusate homeostasis. On the other hand, Urbanellis et al. 22 utilized NMP on porcine grafts for 16 h without the use of urine recirculation. Kidneys undergoing NMP are primarily perfused with a plasma-free RBC solution. Different volumes of RBC solution may be used in different models (Table 1). An optional alternative to an RBC solution is an artificial oxygen carrier, although not as commonly used. Bhattacharjee et al. 6 demonstrated the use of hemoglobin-based oxygen carrier (HBOC-201), a bovine-derived alternative to the use of RBC units, as a suitable artificial alternative based on a porcine kidney model undergoing ex-vivo SNMP.
Perfusate composition may also involve the delivery of a therapeutic agent during perfusion. In a porcine kidney perfusion model, Mellati et al. 16 demonstrates the feasibility of introducing alpha-1 antitrypsin (AAT) during NMP after the priming solution begins circulating through the perfusion circuit. A protease inhibitor, AAT, may offer a potential therapeutic mechanism to respond to kidney inflammation and immune activation from IRI.
Perfusate composition may also depend on the purpose of NMP. For purposes of assessment, preservation, or repair, the perfusate contents are often chosen accordingly. The variability of perfusate contents may also be chosen differently based on whether NMP is preceded by other storage mechanisms, such as SCS or HMP, prior to transplantation.
Oxygenation conditions
Suitable oxygenation conditions are a fundamental requisite in maintaining cellular metabolic function and preventing injurious renal complication. Although ideal conditions and the effect of oxygenation conditions on kidney graft function remain unclear, many NMP systems utilize a gas mixture of 95% O2–5% CO2 or even 100% O2 (Table 1). These high levels of oxygen delivered throughout NMP are a means to maintain blood pH through the duration of perfusion. 26 Although discussion regarding oxygen partial pressures varies as some studies suggest maintaining oxygen partial pressures (PO2) within physiological limits is preferential, many current studies report successful use of physiological oxygen concentrations.21,24 There is yet to be consensus on whether physiological oxygenation levels are preferential to supra-physiological conditions. Blood gas analysis and arterial pressures (PO2 and PCO2) are among the most reported parameters monitored in recent studies (Table 2). Reducing oxygen level throughout perfusion to assess its effect on kidney function demonstrated by Adams et al. 44 provides evidence that although oxygen kinetics was altered, reduced oxygen levels did not disrupt tubular function in a porcine ex-vivo perfusion model.
When to begin NMP and perfusion duration
The initiation and duration of NMP is another factor often tailored to the purposes of NMP (kidney assessment, preservation, and repair). Several recent studies demonstrate an NMP model in which a shorter perfusion duration is utilized immediately preceding transplantation at the recipient transplant site.19,28 This model of NMP allows for pre-transplant assessment in proximity to the potential recipient. In contrast, prolonged NMP as an alternative to traditional SCS has also been studied as a viable tool on its own. Studying perfusion in porcine DCD kidney grafts, Kaths et al. 32 demonstrated that grafts undergoing NMP alone showed significantly lower peak serum creatinine levels relative to the SCS only group at post-operative day 3 after transplantation. Furthermore, a comparison between the groups undergoing 16 h NMP, 8 h NMP, and 15 h SCS with 1 h NMP revealed that grafts with 16 h of NMP exhibited a trend of lower serum creatinine levels following transplantation when compared to other groups (SCS 16 h; 8 h SCS + 8 h NMP, and 15 hSCS + 1 h NMP). These observations suggest not only that NMP has benefits as a sole alternative to SCS, but also that a prolonged duration of NMP may be advantageous. Variability in the duration of NMP is shown in Table 1.
Perfusion parameters and biomarkers
Biochemical injury markers are an important source of information for the assessment of kidney function and performance both during and after NMP. Measurements of relevant biomarkers can be taken from perfusate, blood, or urine samples depending on the marker of interest. These measurements provide informative values of kidney quality and serve as an aid in the decision-making process for acceptability of transplant.
Various markers of injury have been reported as assessment tools in kidney perfusion, and thus there is not a unified consensus on which are most important to observe in relation to kidney NMP. Although consensus is lacking, several notable biomarkers are frequently reported in literature. Aspartate aminotransferase (AST), lactate dehydrogenase (LDH), kidney injury molecule-1 (KIM-1), and neutrophil gelatinase-associated lipocalin (NGAL) have important applications to kidney NMP and assessment of graft function. KIM-1 and NGAL are two of the most recognized markers of kidney injury. NGAL is an injury marker for acute renal injury. 45 Similarly, KIM-1 has been shown as a marker for human renal proximal tubule injury. A study from Han et al. 46 demonstrated that based on urine collection from 32 adult patients with various renal complications, KIM-1 had increased expression levels in those with ischemic acute tubule necrosis (ATN) than those with other forms of AKI. Both KIM-1 and NGAL are markers measured via a urine sample. Weissenbacher et al. 31 used a human kidney NMP model to show that NGAL and KIM-1 had a clear decrease as the duration of NMP increased. The extensive use of KIM-1 and NGAL as an assessment measure in NMP protocols allows for a reliable understanding of kidney perfusion. AST and LDH are also widely common markers of cellular damage and a means of assessing tissue injury. In a porcine perfusion model, Kaths et al.14,24 showed in their studies from 2016 and 2017 that respectively, (1) levels of AST and LDH were below detectable levels at each hourly perfusion assessment, and (2) although increased in all groups, AST and LDH remained lowest during NMP in all groups. Perfusion solution creatinine levels are also useful parameters for assessment of kidney function.47,48 During EVNMP, creatinine should be added to the circuit to enable subsequent quantification of creatinine clearance.
NMP in combination with diagnostic and functional imaging
As the quantification of biomarkers and monitoring of parameters throughout NMP is pivotal to assess, imaging techniques may also enhance understanding of kidney physiology during perfusion. Various diagnostic and functional imaging techniques can be used in association with NMP. As the first study to utilize magnetic resonance imaging (MRI) techniques to understand renal perfusate flow distribution, Schutter et al. 30 utilized arterial spin labeling (ASL) using water molecules as the contrast agent to visualize flow distribution at intervals of 15 min for the entire duration of the 3 h NMP protocol, assessing both porcine and human kidneys. This study showed that beginning perfusion, kidneys were centrally perfused while the cortex reached a physiological perfusion level after hours 1 and 2. 30 In this circumstance, functional imaging in conjunction with NMP must be utilized with caution as results might not always reflect physiological accuracy. Nonetheless, MRI imaging allows for time-interval comparisons of physiological changes throughout the duration of NMP.
Diagnostic and functional imaging in association with NMP is a clinical avenue that must be explored in more detail before its findings provide substantial physiological evidence. Although, these techniques offer major potential as visualization tools for understanding the mechanism of NMP on physiological kidney processes, especially as they are non-invasive. Applying these to a standard NMP protocol may help optimize the assessment process and decision-making model for determining viable kidney donations acceptable for transplantation.
Logistical considerations
In connection to the clinical capabilities of NMP, there are logistical and financial considerations that must not be ignored. While several studies have weighed the cost-utility benefits for NMP of liver, demonstrating cost-effective implications following implementation into a public healthcare payer perspective, this type of analyses has not been performed with respect to kidney perfusion. 49 A cost-utility analysis will provide further information to transplant centers about the cumulative effectiveness of NMP with respect to all involved parties, including patients, surgeons, and transplant centers.
Potential clinical use of kidney NMP
IRI is a significant barrier to graft success and longevity. NMP may offer potential mitigation of this issue in a variety of manners. Namely, NMP presents as a new technique for (1) kidney quality assessment, (2) kidney preservation, and (3) kidney repair or reconditioning. The purpose of NMP guides its use and often informs the duration of perfusion. Clinical studies demonstrating these uses, done on both porcine and human kidney models, are shown in Table 2.
Kidney quality assessment
Assessment of organ quality is an essential step in deciding the acceptability and viability of the donor kidney. This ensures best graft and patient outcomes. NMP reveals itself as a solution for assessment of quality in donor kidney grafts, especially as more ECD and DCD kidneys are being allocated. 5 Hosgood et al. demonstrated the feasibility of using NMP in this capacity in association with a scoring system of kidney quality as a determinant of suitability before transplant. The score assessment developed factors renal blood flow thresholds, urine output assessment, and macroscopic appearance grading with a score of 1 designating highest graft quality and a score of 5 designating lowest graft quality. 13 Of the 74 previously discarded human kidneys, this study assessed 81% (n = 60) with scores of 1–4 and 19% (n = 14) with scores of 5. This application of a kidney quality scoring system in conjunction with NMP may help to lower the challenges that waiting recipients face in receiving a kidney transplant as well as a possible tool for transplant centers to utilize in assessing graft suitability. In turn, this may prevent unnecessary discard of kidneys. In an additional UK-based study from Hosgood et al., a quality assessment score (QAS) was again used to determine which previously rejected human kidneys could be transplanted. Using this scoring system, kidneys identified with a score of 3 or less were deemed acceptable for transplant. 20 The QAS was composed of mean renal blood flow, macroscopic assessment of perfusion, and urine output assessment. 20 Human kidneys underwent 60 min of NMP, and five total kidneys were transplanted only one of which demonstrated DGF and had the highest QAS score (3) of those transplanted kidneys. As the only report that employed NMP on previously discarded human kidneys followed by transplantation, this study further demonstrates the capability of utilizing NMP as an assessment.
Kidney preservation
A potential alternative to SCS and HMP, NMP is further widely studied as a storage and preservation tool for grafts awaiting allocation and transplant. Studies have been done to compare the preservation potential of NMP to both HMP and SCS. Kaths et al. studied post-perfusion and transplant outcomes for porcine kidney models undergoing either 8 h of NMP or SCS. Comparison of kidney grafts amongst both groups showed that the NMP group exhibited acid-base parameters in stable homeostatic range as well as a high renal O2 consumption. 14 The injury markers, LDH and AST, were not seen in the NMP group and there was no impact on patient survival amidst grafts that underwent perfusion prior to transplant. These findings suggest the potential of NMP as a replacement preservation option to SCS. Using a porcine autotransplant model, Kaths et al. showed that increasing duration of NMP while subsequently decreasing the duration of SCS resulted in lower peak serum creatinine levels for porcine kidneys in the 16 h NMP group compared to all other groups (16 h SCS, 15 h SCS + 1 h NMP, and 8 h SCS + 8 h NMP) following transplantation. 32 This is a porcine autotransplant model in kidneys subjected to 30 min of warm ischemia at retrieval. It is debatable whether this is a good model of DCD kidney transplantation as the kidneys came from young, healthy pigs. Similarly, Urbanellis et al. 22 (Table 2) utilized three preservation groups where porcine kidneys were exposed to 30 min WI followed by 16 h of either SCS, HMP, or NMP. Results of the NMP group showed an improvement in creatinine clearance on post-operative day 3 while the SCS and HMP groups showed a significant decrease in creatinine clearance. Furthermore, the NMP group also demonstrated lower mean peak serum creatinine levels at an earlier post-transplant timepoint than that of either SCS or HMP groups. Amongst all three groups, tubular injury was equally low. These studies highlight the potential feasibility of NMP use for a duration longer than 8 h. Recently in the first randomized controlled 2 to compare traditional SCS (n = 168) with SCS + 1 h NMP (n = 170) in DCD human kidney transplantations, Hosgood et al. 50 demonstrated that 1 h of perfusion does not reduce the occurrence of DGF. Kidney repair and reconditioning
Recent studies also demonstrate the use of NMP subsequently following time periods of SCS and/or a period of WI as a means of showing its graft reconditioning capabilities. In a single-center, UK-based study (Table 2), Hosgood et al. 27 showed that levels of heat-shock protein-70 (HSP-70) and interleukin-6 (IL-6), two markers of cellular repair pathways, were upregulated in porcine kidneys undergoing 60 min of NMP thereby demonstrating repair capabilities. Kaths et al. demonstrated the use of NMP as a successor to WI time and SCS amongst three groups of porcine grafts undergoing 30 min induced WI time and 8 h SCS followed by either 1, 8, or 16 h of NMP. 24 Hosgood et al. 18 also showed in a 2015 study that of 22 discarded human kidneys undergoing 60 min NMP, 19 received an NMP assessment score of 1–4, and they note their belief that these 19 kidneys would be potentially usable. These studies demonstrate the capability of using NMP for graft repair, but the duration of NMP for optimal repair ultimately remains unknown.
Conclusion and future directions
Growing evidence suggests NMP as a promising new approach to improve post-transplantation kidney success and improve patient outcomes. With the rising need for kidney donations and the growing waitlist for acceptable donor kidneys, action is needed to mitigate this issue as the demand grows for use of ECD kidneys. Currently there is no nationally-available NMP kidney pump system that can replicate the improved kidney transplant outcomes. Thus, such a platform for kidneys holds great national importance to assess true organ viability, and it could allow for rehabilitation and rescue of those organs before transplant.
Although multiple aspects of NMP prove promising, great variation still exists amidst protocol and practice leaving behind limitations to the feasibility of NMP becoming common clinical practice. Previously described perfusion characteristics (Table 1) and large animal models of NMP (Table 2) demonstrate that consensus has not been reached on the most advantageous parameters for implementing NMP into widespread clinical practice. Additionally, the determination of optimal perfusate composition and perfusion durations will provide valuable insights into the use of NMP for various applications of preservation, kidney assessment, and repair. Further studies are also needed to enhance our understanding of NMP in the context of interrelated complications such as kidney IRI. Establishing consensus and gaining deeper insight into both issues will progress the future of nephrology and therapeutic practice. Although these conclusions are not fully made by previous studies, NMP model outcomes demonstrate success with decreasing the rate of DGF and thus, improving patient and graft survival post-transplantation.21,28,33 Our group will investigate the safety and efficacy of using NMP as a viability assessment and rehabilitation tool for non-utilized organs. The knowledge gained through this work will help to develop tools for predicting non-utilized kidney functioning capacity under NMP.
An NMP setup with MRI compatibility also offers a unique clinical mechanism for assessing intrarenal physiology throughout the progression of NMP. 30 Increasing the combined use of NMP and diagnostic imaging techniques holds great potential in achieving consensus on relevant biomarkers, optimal protocol, and the most important parameters to monitor. Further investigations are needed to explore the potential of NMP with related therapeutic modalities, including antioxidant therapy and nutrients, administration of MSCs, and therapeutic gases during kidney perfusion. These avenues should be prioritized as future focus points for better understanding of NMP and development of therapeutic interventions.
Supplemental Material
sj-docx-1-jao-10.1177_03913988231207719 – Supplemental material for Normothermic ex vivo perfusion of deceased donor kidneys and its clinical potential in kidney transplantation outcomes
Supplemental material, sj-docx-1-jao-10.1177_03913988231207719 for Normothermic ex vivo perfusion of deceased donor kidneys and its clinical potential in kidney transplantation outcomes by Meghan Unes, Kento Kurashima, Yasar Caliskan, Edward Portz, Ajay Jain and Mustafa Nazzal in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.