
Abstract
Objective:
Sex-specific differences in the epidemiology of chronic kidney disease, such as higher prevalence of women on pre-dialysis and men on chronic dialysis treatment, have been reported worldwide. In this regard, data from non-high-income countries are scarce. We aimed to compare the demographic, clinical, and dialysis characteristics of incident dialysis patients, both men and women, in a large cohort of Brazilian patients over a 12-year period.
Methods:
This was a multicentric retrospective cohort study coordinated by the Brazilian Society of Nephrology. The study included all adult incident dialysis patients in the Brazilian Dialysis Registry from January 2011 to December 2022. The variables studied encompassed age, skin color, education, CKD etiology, predialysis nephrologist care, dialysis characteristics, and geographic region. Additionally, the sample was analyzed for each of the three 4-year periods over the 12 years of data collection.
Results:
A total of 24,632 incident dialysis patients were included. Men were 59.1% of the dialysis population, remaining stable over the three 4-year periods. Besides other differences, women started dialysis younger (58.5 ± 16.2 years vs 59.5 ± 14.4 years; p < 0.001), had a lower educational level (less than 8 years at school: 54% vs 44%; p < 0.001), received more predialysis nephrologist care (46.2% vs 44.2%; p = 0.04), and had a higher prevalence of peritoneal dialysis (4.4% vs 3.5%; p = 0.03).
Conclusion:
We consistently observed a higher prevalence of men on dialysis and differences in demographic, clinical, and dialysis characteristics. The underlying reasons for these sex differences still necessitate further clarification.
Introduction
Sexes may exhibit different experiences and manifestations of the same disease, presenting varying clinical findings, pathophysiology, therapy response, and abilities to tolerate/cope with it. 1 This is evident among people with chronic kidney disease (CKD), where sex differences are observed in both predialysis and kidney failure stages.
Pooled data from 33 international population-based studies revealed that CKD is more prevalent in women, with an age-standardized global prevalence of 10.4% in men and 11.8% in women. 2 However, it is noteworthy that 60% of those initiating renal replacement therapy are men,3,4 a pattern also seen in the Brazilian population.5,6
Biological, cultural, and behavioral factors and their complex interaction have been proposed to account for the enduring sex disparities in predialysis and renal replacement therapy worldwide. For instance, differences in life expectancy and disease progression between sexes; inaccuracies in GFR estimate equations leading to CKD overdiagnosis; and sociocultural attributes of masculinity and femininity whereby men and women might be treated and cope with their disease differently.1,7 It is conceivable that women are more likely to die before reaching renal replacement therapy or may not have equal opportunities to initiate it. 7
Epidemiological and clinical differences are also observed between incident dialysis men and women. In some international studies, primarily from developed regions, women initiate dialysis at an older age than men, 8 and catheter use at dialysis initiation is slightly more common in women than in men. 9
Data regarding sex differences in dialysis patients from non-high-income countries are limited. This manuscript aims to compare the demographic, clinical, and dialysis characteristics of incident dialysis men and women in a large cohort of Brazilian patients spanning a 12-year period.
Methods
This is a retrospective analysis of the Brazilian Dialysis Registry (BDR), an electronic database created in 2010, coordinated by the Brazilian Society of Nephrology (BSN) to collect clinical and epidemiological information from patients undergoing dialysis therapy. Patients from 108 dialysis centers were included in this analysis, corresponding to approximately 13% of the current total number of Brazilian centers (20% from the South, 13% from the Southeast, 13% from the Midwest, 9% from the Northeast, and 6% from North dialysis centers). The methods for data collection have been published in detail elsewhere. 10 The study was approved by the ethical committee of the Universidade Federal de São Paulo in 2013, August 16, n. 362.578.
In this study, we analyzed data from all incident dialysis patients included in the BDR from January 2011 to December 2022. We excluded those younger than 18 years old (n = 171) and without sex information (n = 24).
We compared differences between men and women for the variables: age, self-declared skin color, education, CKD etiology, predialysis nephrologist care, first dialysis characteristics, first chronic dialysis program, dialysis funding, and geographic region. We also conducted cross-sex and within-sex comparisons in each of the three 4-year periods over the 12-year data collection (2011–2015; 2016–2019; and 2017–2021).
Statistical analysis
Variables are reported as means and standard deviations or as percentages, as appropriate. Means were compared using the t-test or ANOVA; the chi-squared test was used to assess differences between categorical variables.
Statistical analyses were performed with Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows software, version 21.0, Armonk, New York, United States). p Values <0.05 were considered statistically significant except for comparisons between three periods, with a significance of p < 0.017 according to Bonferroni adjustment for multiple comparisons.
Results
Sex distribution in study participants by time period
A total of 24,623 incident dialysis patients were included in the analysis, 14% in the first 4-year period (2011–2014), 38% in the second (2015–2018), and the remaining 48% in the last period (2019–2022). Of the total population, 59.1% were men, and 40.9% were women. The sex distribution of the dialysis population was similar over the three 4-year periods (59.5% and 40.5%, 58.3% and 41.7%, and 59.6% and 40.4% for men and women in each study period, respectively, p = 0.15).
General characteristics of participants by sex
The comparisons of the general characteristics between the men and women total population, and over the three 4-year periods, are shown in Tables 1 and 2, respectively.
Comparisons of the general characteristics between men and women starting chronic dialysis.
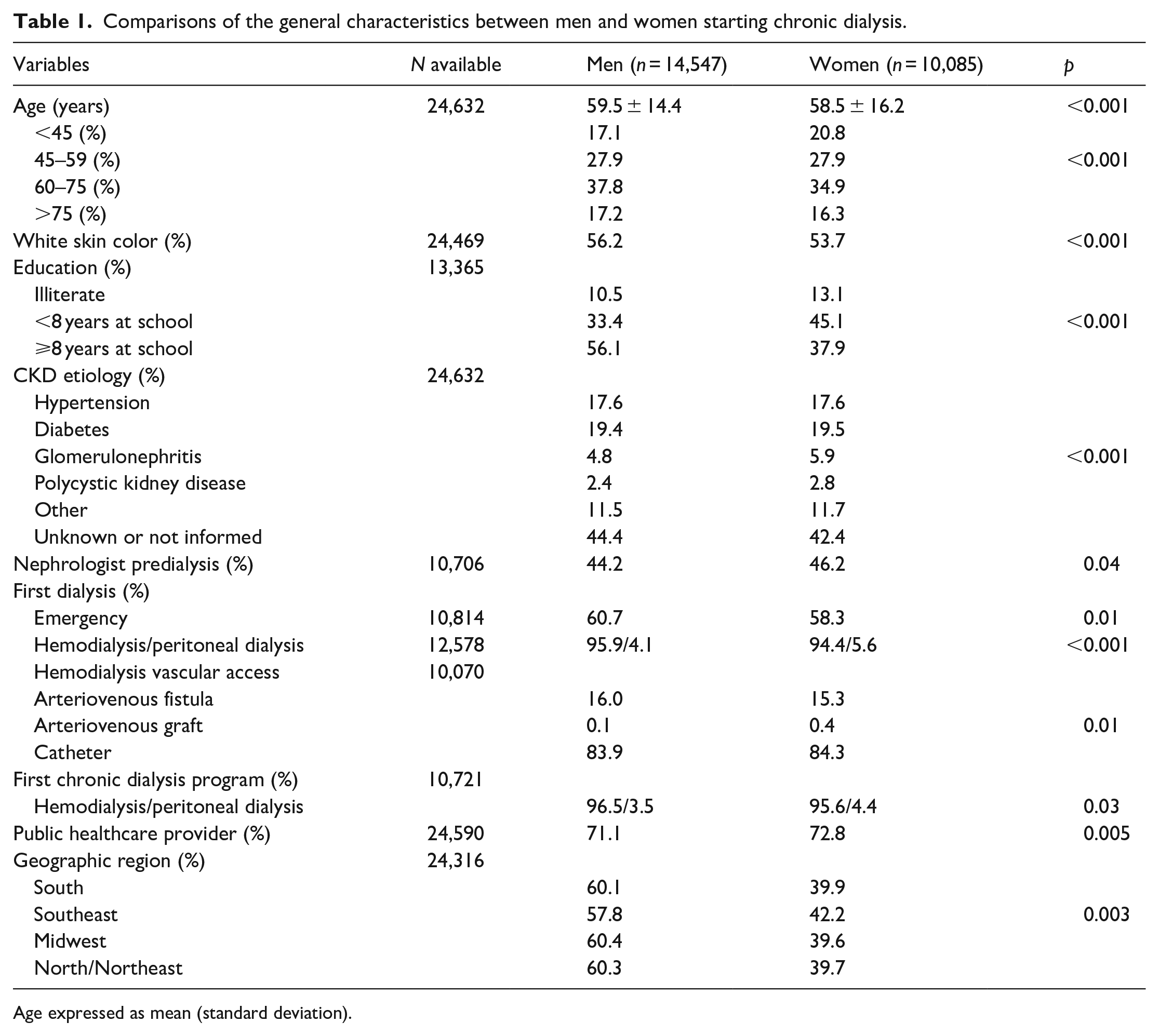
Age expressed as mean (standard deviation).
Comparisons of general characteristics according to sex across the three 4-year periods of data collection.
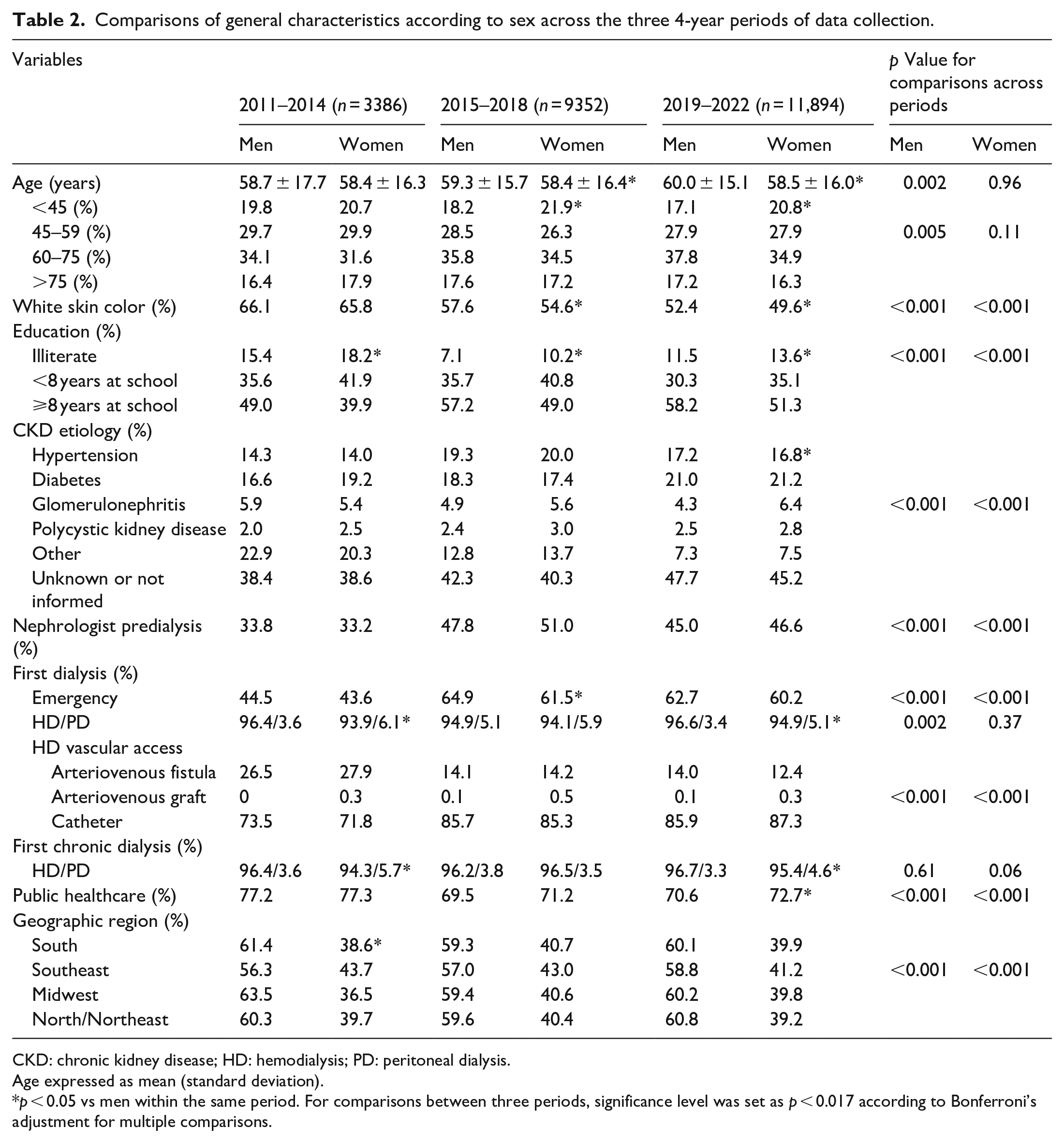
CKD: chronic kidney disease; HD: hemodialysis; PD: peritoneal dialysis.
Age expressed as mean (standard deviation).
p < 0.05 vs men within the same period. For comparisons between three periods, significance level was set as p < 0.017 according to Bonferroni’s adjustment for multiple comparisons.
Men started dialysis treatment on average 1 year older than women. Older men were also observed in the latter two 4-year periods, and their age increased significantly over time, while no difference was observed in women. Age categories distribution also differed in the whole population and the latter periods. We found a higher prevalence of women younger than 45 years and men older than 60 years in the most recent periods (Table 2).
There was a significantly higher prevalence of white men than women in the total population and in the second and third periods. The percentage of white skin color patients of both sexes decreased over time.
Men had a higher educational level than women in the general sample and in all 4-year periods.
Concerning CKD etiology, significant differences between sexes were found in the whole sample and the third period, mainly due to the higher prevalence of women with glomerulonephritis. Over time, both sexes had significant changes in etiology distribution.
The distribution of sexes was different across geographical regions in the total population and during the first period, with a higher prevalence of women in the Southeast compared to other regions.
A higher percentage of women had predialysis nephrologist care in the total sample and there was an increase in the prevalence of care after the first period.
Dialysis features by sex
More men initiated dialysis on an emergency basis in the total sample and during the second period. Emergency dialysis start increased for both sexes after the first period.
Peritoneal dialysis (PD) as the first dialysis of life was slightly more common in women than men in the whole sample, particularly in the first and third periods. Over time, the distribution between both modalities tended to change only in women. Similarly, women also used PD as the first dialysis program at a slightly higher proportion than men.
In the whole population, a slightly higher proportion of men started hemodialysis (HD) with arteriovenous fistula (AVF) than women, particularly during the third period. The use of central venous catheters increased over time in both sexes.
A slightly greater proportion of women than men had public maintenance dialysis funding in the entire sample and during the last period. However, public funding decreased over time for both sexes.
Discussion
Brazil ranks third in the number of chronic dialysis patients globally, with 153,831 patients as of July 2022. 6 Eighty percent of the patients on chronic dialysis are financed by the public health system and 20% by private health insurance companies. Approximately 75% of dialysis clinics are privately owned. Most dialysis centers (65%) assist patients from the public health system and private health insurance companies. However, 19% and 16% only care for patients from the public or private system, respectively. 6
In this retrospective analysis of a large Brazilian cohort, we observed that a sustained higher prevalence of men initiating dialysis was maintained over a 12-year period, along with distinct characteristics between the sexes regarding the age at which dialysis was initiated, educational levels, and other factors. The higher prevalence of men receiving dialysis (58%–60%) as reported in our cohort, has remained stable over the decades, 11 consistent with findings worldwide. 12 The reasons why the prevalence of CKD is higher in women, but they are not the majority in RRT around the globe, are not well elucidated. 13 Besides potential epidemiological and biological rationales, this phenomenon might also be partially attributed to factors such as reduced access to expensive care for women, especially when costs are out-of-pocket. 14 Additionally, women may be more inclined to opt for conservative kidney care rather than undergoing dialysis. 7 Also, more women live in poverty, receive less education, are more dependent on others for healthcare decision-making, and suffer from entrenched discrimination and vulnerability. 15 Nevertheless, men experience a faster decline in kidney function, more frequently progress to kidney failure, 16 are more exposed to occupational risks, and have less access to screening, prevention, and primary care. 13
Women starting dialysis treatment slightly younger than men was a pattern also observed in Australian dialysis patients, 12 but not in a European cohort where they were significantly older than men (61.8 ± 14.9 vs 60.2 ± 14.8). 8 Likewise our population, in the European Registry, the prevalence of men also increased in older age groups. 4 The rising trend, particularly in elderly men undergoing dialysis over the last decade, was similarly observed in Taiwan. 17
The higher prevalence of white men starting dialysis cannot be solely explained by Brazil’s skin color distribution by sex. According to the 2010 demographic census, 48.7% of women had white skin color against 46.7% of men. 18 In our sample, there were more white color patients than in the Brazilian population. This disparity can be attributed to the over-representation of participants from the Southeast and South regions, mainly in the first 4-year period, known for their higher European colonization.
Men had higher educational levels than women, and both genders showed improvement in education levels over the decade of study reflecting the national trend. Until the 80s Brazilian women had fewer years of formal education than men, but both genders increased their educational level mainly in the last decades of the last century. 19
Regarding CKD etiology, women had a slightly higher prevalence of glomerulonephritis than men, as shown in a previous national biopsy register. 20 However, the high proportion of individuals with unknown or not informed etiology (43%) prevents us from a proper analysis.
Less than half of our participants had predialysis nephrologist care, with women having a slight advantage over men (46.2% vs 44.2%, respectively, p = 0.04). This finding may in part be explained by the women’s greater tendency to seek healthcare services in Brazil. According to the 2019 National Health Survey, the proportion of women who consulted a physician in the 12 months before the interview was 82.3% versus 69.4% of men. 21 In the United States, no difference was observed in the sexes’ access to predialysis nephrologist care in the latest years. 22 We previously showed in an analysis of the same cohort that a higher percentage of women also had predialysis dietitian follow-up, an advantage not observed after adjustment for predialysis nephrologist care. 23 The second 4-year period had a higher prevalence of nephrologist follow-up compared to the first and third for both sexes. For reasons yet to be clarified, this relatively higher women’s predialysis care did not reflect in a greater percentage of them on renal replacement therapy. The slightly higher prevalence of men that had an emergency dialysis start might be a consequence of their less frequent predialysis care.
Overall, women had a somewhat higher use of a central venous catheter for the first hemodialysis vascular access than men, a pattern observed in other international cohorts.9,22 Nephrologists’ perceptions about the smaller vascular diameters in women and patients’ cosmetic concerns may explain this finding. 7
A higher proportion of women on PD was also captured in a large cohort of Brazilian patients, which had 52% of women out of 7007 incident patients. This imbalance was not observed in the United States or European registries.4,24 Social and cultural factors may underlie this feature.
The difference regarding dialysis funding might be attributed to men’s higher education levels, which can directly influence family income and access to private healthcare funding. Moreover, the lower eligibility for private healthcare dialysis funding may eventually have impacted the purported lower acceptance rate of women to RRT.
Regional differences also played a role, with the Southeast having a higher proportion of women in dialysis compared to other regions (42.2% vs 39.6%–39.9%). The Brazilian population consists of 51.1% women (95.6 men/100 women). Notably, the Southeast region has a lower proportion of men (94.2 men/100 women), which may partially explain the relatively higher representation of women on dialysis in the area. Unaddressed residual confounders could also contribute to this observation. Other regional similarities and differences concerning demographics, laboratory parameters, and drug prescription in the BDR were recently published elsewhere. 25
Our study has some limitations, including the missing data from some of the variables analyzed and the retrospective study design, which may have introduced some selection bias. Moreover, the BDR relies on voluntary participation, with only 13% of dialysis centers taking part. Despite this limitation, it includes patients from all regions, although there is under-representation of dialysis centers from the North/Northeast. However, the proportion of patients on dialysis per sex aligns with the most recent Brazilian Dialysis Surveys. 11 As strengths, we emphasize the large nationwide sample and the novelty of exploring factors associated with sex distribution in dialysis therapy in a middle-income country,
Conclusion
In conclusion, our study reveals a consistently higher prevalence of men undergoing dialysis, along with differences in demographics, clinical profiles, and dialysis characteristics between the sexes. The underlying reasons for these sex differences still necessitate further clarification.
Footnotes
Acknowledgements
Brazilian Dialysis Registry Investigators: Beatriz Veneza; Carlos Comin; Yoshimi Watanabe; João Biernat; Patrícia Teixeira; Sérgio Bucharles; Elzo Ribeiro Junior; Geraldo Córdova; Marcelo Gonçalves; Gisele Furtado; Roberto Salon; Milene Guilhem; Hotone Dallacosta; Marco Túlio; Renato Medeiros; Elisa Sampaio; Jorge Z Ramos; Gelson Santos; Orlando Junior; Neyde Pontes; Ana C. Matos; Ciro Costa; Luiz F. Figueiredo; Sílvia Medeiros; Cyro Moreira Filho; Homero Sul; Wagner Santa Catharina; Sandra Souza; Neiva Coelho; Manif Jorge; Mendell Lemos; Rodrigo Pereira; Maziael Moraes; Helio Galvão; Rosilene Coelho; Ronaldo Allão; Luiz Claudio Gonçalves; Jair Miguel; Rosa Malta; Jorge Menezes; Raimundo Martins Neto; Maria Emilia Diniz; Sinaria A Ojeda; Flávio Moura; Luciana Serpa; Tania Sobral; Marcos Mura; Ana Cláudia Barbosa; Marcos Gevert; Nelson José; Zita Leme; Márcio Moraes; Fabia Fernandez; Natasha Constancio; Roberto Benvenutti; Ian Rehfeldt; Julio Cesar; Marilia Oliveira; Flavio Paula; Nilsa Martins; Denise Melo; Ismar Monteiro Junior; Jeronimo Centeno; Luiz Antonio Pais; Consuelo Carvalho; Aparecida Visoná; Maria Goretti Polito; Januário Roberto; Glória Reis; João Damásio Simões; Tânia Brandão; Fernando Thomé; Ana Lydia Cabeça; Marcos Scheidemantel; Márcia Beatriz Abichequer; Eli da Silva; Silvana Oliveira; Renata Starling; José Miguel Bregón; Marcelo Ruas; Antonio Brito; Ana Bela Palazzo; Mario Rodrigues; Rafael Siqueira; Aluizio C e Silva; Nilso Moreira; Maria de Fátima Alvarenga; João C Filho; André L Marassi; Rodrigo Braz; Cristiano da Silva; Fernanda Polacchini; Henrique Carrascossi; Leandro Lucca; Gelzie Ennes.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RS receives a research grant from the Brazilian Research Council–CNPq (N.301767/2022-0).