
Abstract
Reliable stratification of the risk of early mortality after postcardiotomy veno-arterial extracorporeal membrane oxygenation (V-A-ECMO) remains elusive. In this study, we externally validated the PC-ECMO score, a specific risk scoring method for prediction of in-hospital mortality after postcardiotomy V-A-ECMO. Overall, 614 patients who required V-A-ECMO after adult cardiac surgery were gathered from an individual patient data meta-analysis of nine studies on this topic. The AUC of the logistic PC-ECMO score in predicting in-hospital mortality was 0.678 (95%CI 0.630–0.726; p < 0.0001). The AUC of the logistic PC-ECMO score in predicting on V-A-ECMO mortality was 0.652 (95%CI 0.609–0.695; p < 0.0001). The Brier score of the logistic PC-ECMO score for in-hospital mortality was 0.193, the slope 0.909, the calibration-in-the-large 0.074 and the expected/observed mortality ratio 0.979. 95%CIs of the calibration belt of fit relationship between observed and predicted in-hospital mortality were never above or below the bisector (p = 0.072). The present findings suggest that the PC-ECMO score may be a valuable tool in clinical research for stratification of the risk of patients requiring postcardiotomy V-A-ECMO.
Introduction
Patients requiring veno-arterial extracorporeal membrane oxygenation (V-A-ECMO) after adult cardiac surgery have a high risk of mortality 1 and their risk stratification remains elusive. We have previously developed a specific risk scoring method for prediction of in-hospital mortality after postcardiotomy V-A-ECMO, 2 which was externally validated in the present study.
Methods
The present series was gathered through an individual patient data (IPD) meta-analysis 3 and its protocol is registered in the PROSPERO international register for systematic reviews (CRD42022359392). Details on this IPD meta-analysis have been previously reported. 3 In this study we followed the STROBE guidelines for cohort studies (Supplemental Table 1). 4 Approval by the Institutional Review Board of the Authors’ Institutions and informed consent were not asked because of the anonymized data and the retrospective and meta-analytic nature of the study. Patients aged >18 years who required V-A-ECMO for acute heart failure after surgical procedures on heart valves, coronary arteries, the ascending aorta and/or aortic arch and ventricular walls were eligible for this IPD meta-analysis (Supplemental Table 2). The additive PC-ECMO score can be calculated by adding the following points given to each independent predictor of in-hospital mortality: female gender (1 point), advanced age (60–69 years, 2 points; ⩾70 years, 4 points), prior cardiac surgery (1 point), arterial lactate 6.0 mmol/L or greater before venoarterial extracorporeal membrane oxygenation (2 points), aortic arch surgery (4 points) and preoperative acute stroke/unconsciousness (5 points). The coefficients of the PC-ECMO score are summarized in Table 1. As an example, a 69-year-old female with preoperative arterial lactate of 9.0 mmol/L would have an additive PC-ECMO score of 5. Her logistic PC-ECMO score can be calculated using the equation and coefficients reported in Table 1: predictive in-hospital mortality = 2.71828(-0.467 + 0.521 + 0.390 + 0.552)/1 + (2.71828(-0.467 + 1.127 + 0.398 + 0.552)), which is 0.730, that is, 73.0%.
Coefficients and additive points for calculation of the logistic and additive PC-ECMO score.
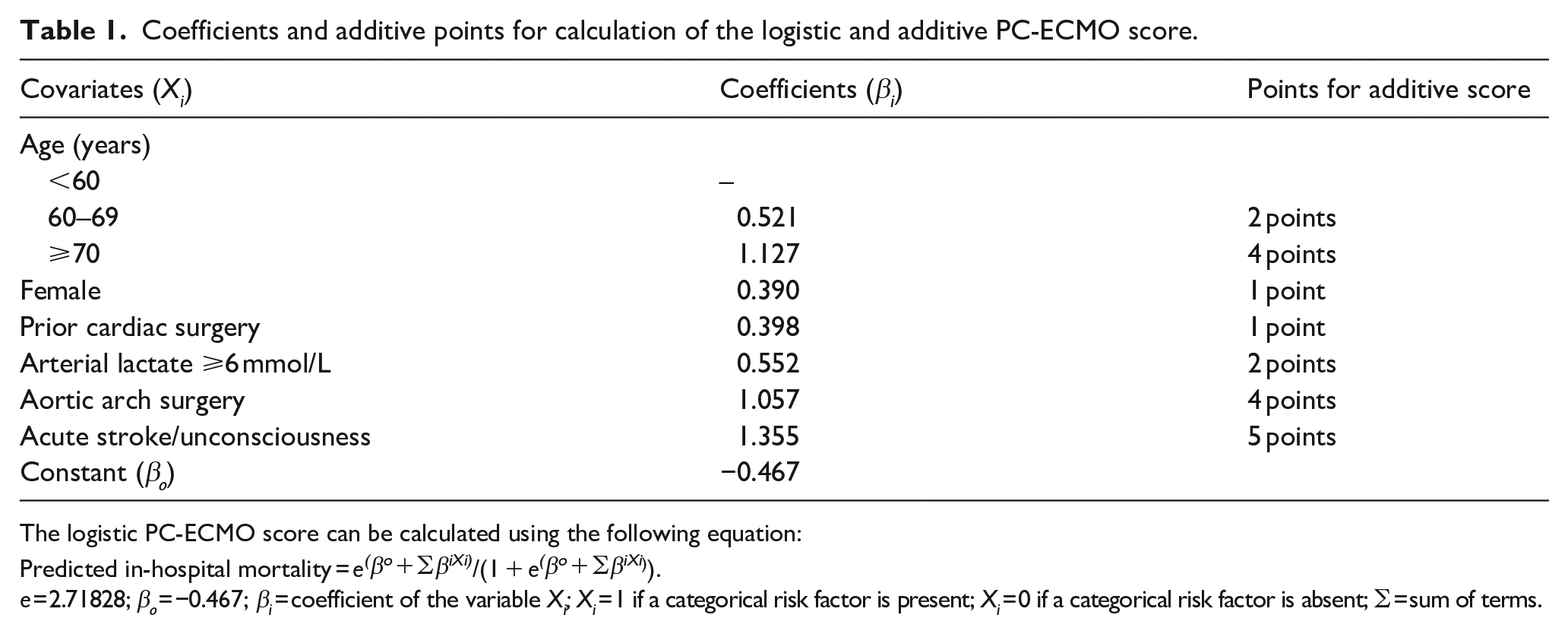
The logistic PC-ECMO score can be calculated using the following equation:
Predicted in-hospital mortality = e(βo + ∑βiXi)/(1 + e(βo + ∑βiXi)).
e = 2.71828; βo = −0.467; βi = coefficient of the variable Xi; Xi = 1 if a categorical risk factor is present; Xi = 0 if a categorical risk factor is absent; ∑ = sum of terms.
The outcome measures of this study were all-cause mortality during the index hospitalization, mortality due to failure to wean from V-A-ECMO and mortality after weaning from V-A-ECMO.
Statistical analysis
Categorical variables are reported as counts and percentages, while continuous variables are reported as means and standard deviations. Logistic regression was used to identify predictors of in-hospital mortality. Discrimination of risk scores was assessed by estimating the area under the receiver operating characteristics curve (AUC) with 95% confidence interval (CI). Difference in AUCs was evaluated with the DeLong’s test. The Brier score, slope, calibration-in-the-large, the expected/observed mortality ratio and calibration belt of the logistic PC-ECMO score in predicting in-hospital mortality were estimated. Analyses were performed using Stata statistical software (version 15.1, StataCorp LLC, College Station, Texas, USA).
Results
A systematic review yielded 273 articles and 31 studies were considered suitable for the present analysis. The investigators of 10 retrospective studies provided IPD for this analysis. These studies included 1503 patients treated at 25 hospitals from Northern America, Europe and Asia. For the present analysis, we excluded 624 patients from the PC-ECMO score derivation dataset 2 and 265 patients with reason (Supplemental Figure 1). Overall, 614 patients from nine studies5–13 with complete data were included in the present analysis (Supplemental Table 3). Patients’ characteristics and operative data are reported in Table 2. Mortality on V-A-ECMO was 44.0%, while in-hospital mortality was 69.4% and mortality after V-A-ECMO weaning was 25.4%. Age, preoperative arterial lactate, prior cardiac surgery and aortic arch surgery were independent predictors of in-hospital mortality in this series (AUC 0.696, 95%CI 0.649–0.743; Hosmer-Lemeshow’s test, p = 0.494; 95%CIs of the calibration belt were never above or below the bisector, p = 0.052; Table 2). The AUC of the probabilities of this regression model did not significantly differ from that of the logistic PC-ECMO score (p = 0.254).
Patients’ characteristics and procedural data.
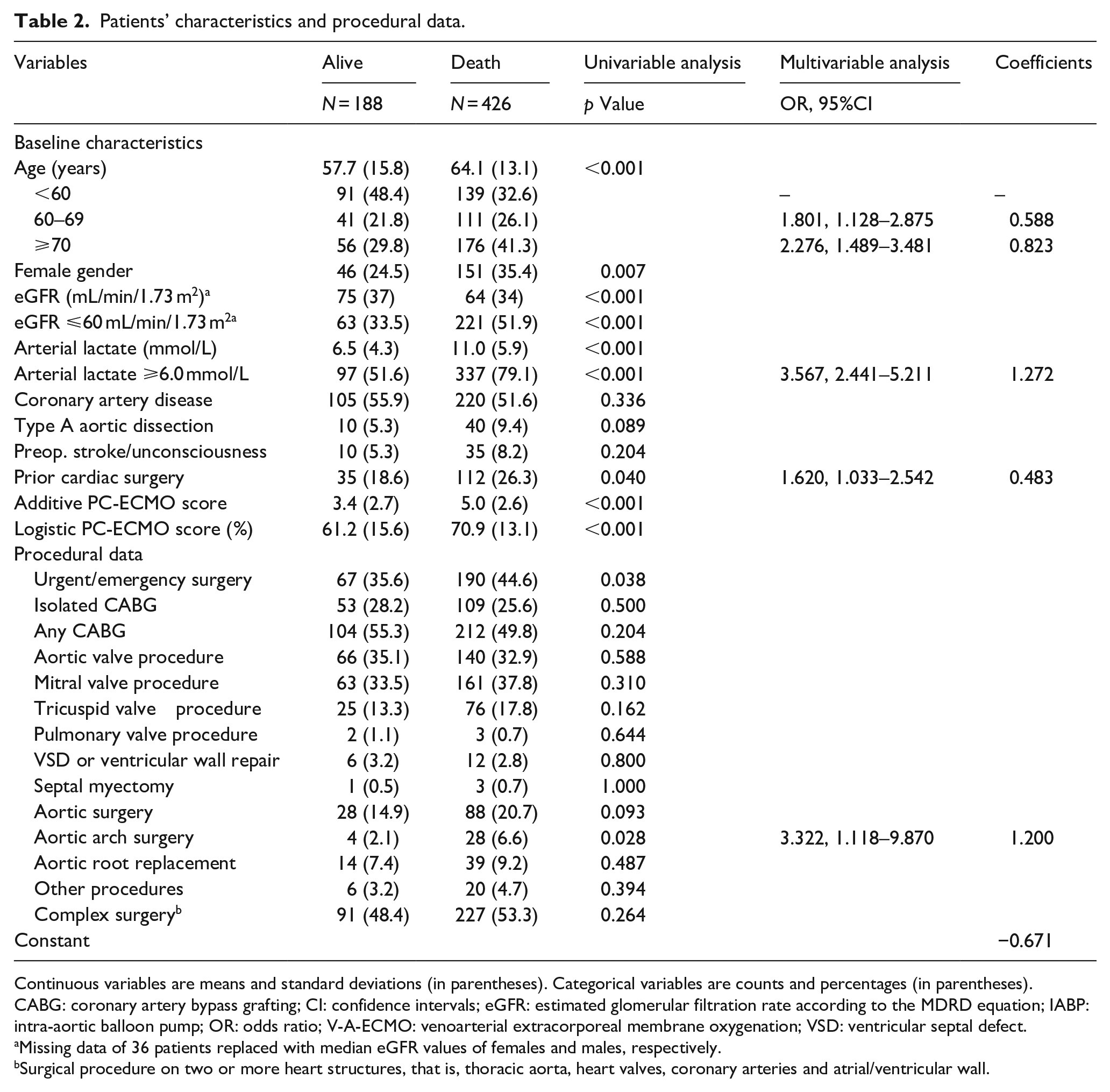
Continuous variables are means and standard deviations (in parentheses). Categorical variables are counts and percentages (in parentheses).
CABG: coronary artery bypass grafting; CI: confidence intervals; eGFR: estimated glomerular filtration rate according to the MDRD equation; IABP: intra-aortic balloon pump; OR: odds ratio; V-A-ECMO: venoarterial extracorporeal membrane oxygenation; VSD: ventricular septal defect.aMissing data of 36 patients replaced with median eGFR values of females and males, respectively.
Surgical procedure on two or more heart structures, that is, thoracic aorta, heart valves, coronary arteries and atrial/ventricular wall.
The AUC of the logistic PC-ECMO score in predicting in-hospital mortality was 0.678 (95%CI 0.630–0.726; p < 0.0001) and of the additive PC-ECMO score was 0.676 (95%CI 0.629–0.724; p < 0.0001). The AUC of the logistic PC-ECMO score in predicting on V-A-ECMO mortality was 0.652 (95%CI 0.609–0.695; p < 0.0001) and for the additive PC-ECMO score was 0.653 (95%CI 0.610–0.696; p < 0.0001). These risk scores were not predictive of mortality after weaning from V-A-ECMO (p = 0.921 and 0.946, respectively).
In-hospital mortality significantly increased along increasing PC-ECMO additive score (Figure 1). The Brier score of the logistic PC-ECMO score for in-hospital mortality was 0.193, the slope 0.909, the calibration-in-the-large 0.074 and the expected/observed mortality ratio 0.979 (Figure 2). 95%CIs of the calibration belt of fit relationship between observed and predicted in-hospital mortality were never above or below the bisector (p = 0.072).
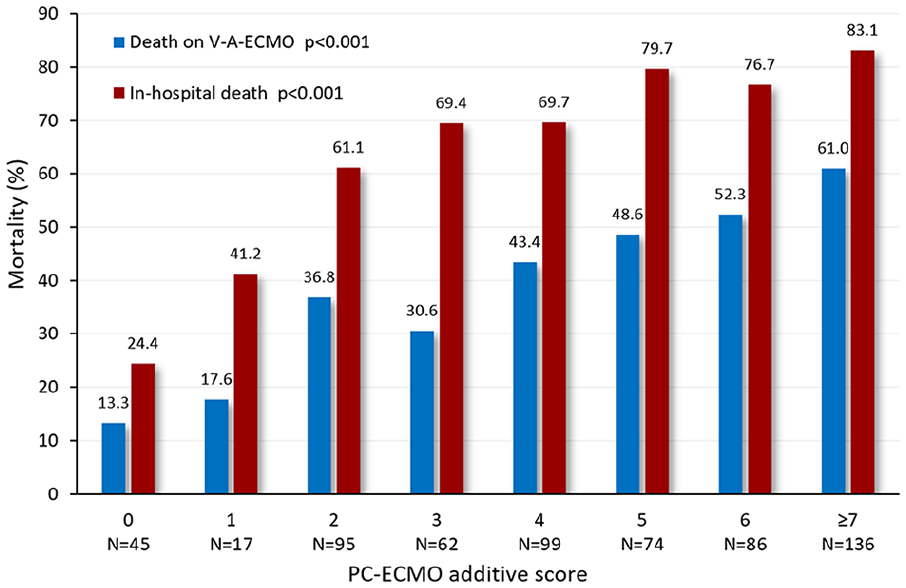
In-hospital and on V-A-ECMO mortality rates according to PC-ECMO additive scores.
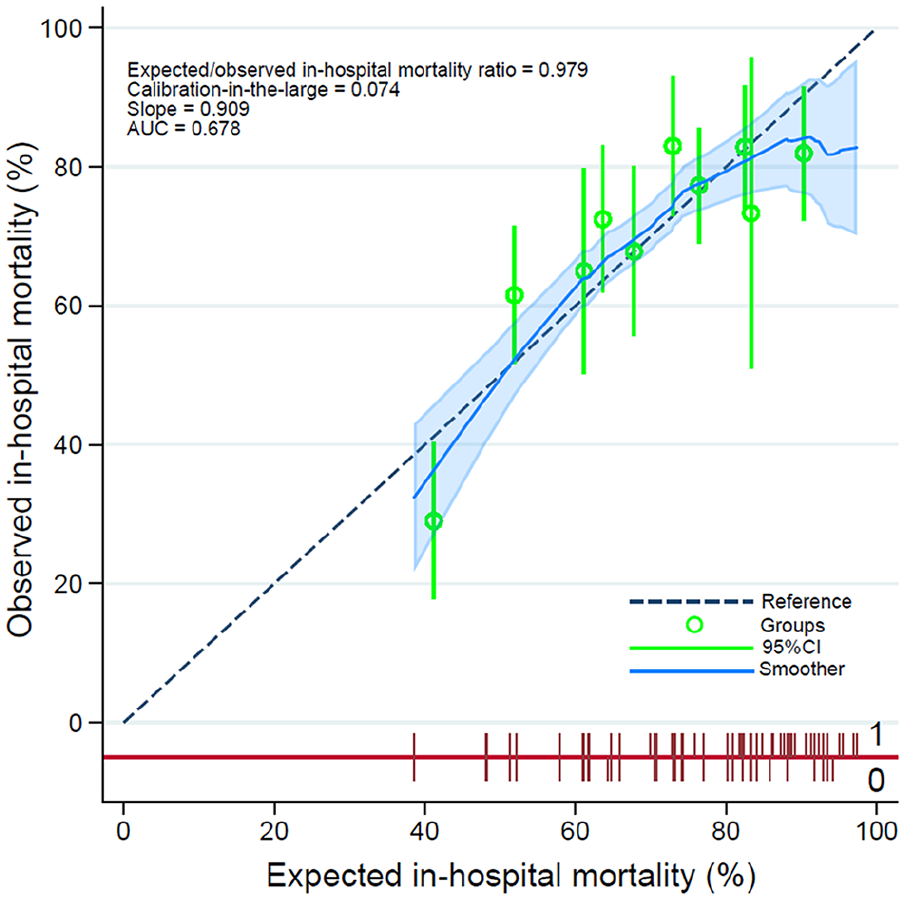
Calibration plot of the logistic PC-ECMO score in predicting in-hospital mortality after postcardiotomy V-A-ECMO.
Discussion
The external validation of the PC-ECMO score showed satisfactory discrimination and calibration performance in a series of patients gathered from an IPD meta-analysis. Calibration demonstrated that the PC-ECMO score tended to overpredict the risk of in-hospital mortality, but the calibration belt CIs of fit relationship observed/predicted in-hospital mortality were never above or below the bisector.
Logistic regression of this IPD series identified four independent predictors of in-hospital mortality in common with the PC-ECMO score, that is, advanced age, pre-V-A-ECMO arterial lactate ⩾6.0 mmol/L, prior cardiac surgery and aortic arch surgery as the index procedure. Still, in-hospital mortality was numerically higher among females and in patients with acute preoperative neurological event. These findings suggest that the predictive importance of the components of the PC-ECMO score can be confirmed in other study populations.
The PC-ECMO score was not able to identify patients whose mortality rate approached 100%. Indeed, clinical risk scores rarely, if ever, can identify with a high degree of certainty those patients who are going to experience an adverse event, and they cannot be used alone to turn down salvage treatments in high-risk patients. Still, clinical judgement can be supported by the presence of one or more components of such risk scores. We do believe that the value of risk stratification methods mainly resides in clinical research as tools to adjust treatment strategies for individual patients’ risk. In this series, the PC-ECMO score was useful also to evaluate the number of patients with an extremely high risk of in-hospital mortality. In fact, 48% of patients of this series had a score ⩾5 which was associated with a prohibitive in-hospital mortality rate of about 80% (Figure 1). These findings suggest that patients’ selection should be refined to allocate resources to patients who may most benefit of this salvage therapy.
This study has two main limitations which deserve to be acknowledged. The retrospective nature of studies included in this analysis is the main limitation of the study. The participating hospitals might have had different referral pathways, specific experience with postcardiotomy V-A-ECMO and perioperative strategies which might introduce bias in this analysis. However, the external validation of the PC-ECMO score in such a heterogenous series confirmed the predictive ability of this risk score, which is likely generalizable to other study populations.
In conclusion, the present results suggest that the PC-ECMO score may be a valuable tool in clinical research for stratification of the risk of patients requiring postcardiotomy V-A-ECMO.
Supplemental Material
sj-pdf-1-jao-10.1177_03913988241237701 – Supplemental material for External validation of the PC-ECMO score in postcardiotomy veno-arterial extracorporeal membrane oxygenation
Supplemental material, sj-pdf-1-jao-10.1177_03913988241237701 for External validation of the PC-ECMO score in postcardiotomy veno-arterial extracorporeal membrane oxygenation by Fausto Biancari, Tatu Juvonen, Sung-Min Cho, Francisco J Hernández Pérez, Camilla L’Acqua, Amr A Arafat, Mohammed M AlBarak, Mohamed Laimoud, Ilija Djordjevic, Robertas Samalavicius, Marta Alonso-Fernandez-Gatta, Sebastian D Sahli, Alexander Kaserer, Carmelo Dominici and Timo Mäkikallio in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.