
Abstract
Background:
This study investigates the hypothesis that presence of atrial fibrillation (AF) in LVAD patients increases thrombogenicity in the left ventricle (LV) and exacerbates stroke risk.
Methods:
Using an anatomical LV model implanted with an LVAD inflow cannula, we analyze thrombogenic risk and blood flow patterns in either AF or sinus rhythm (SR) using unsteady computational fluid dynamics (CFD). To analyze platelet activation and thrombogenesis in the LV, hundreds of thousands of platelets are individually tracked to quantify platelet residence time (RT) and shear stress accumulation history (SH).
Results:
The irregular and chaotic mitral inflow associated with AF results in markedly different intraventricular flow patterns, with profoundly negative impact on blood flow-induced stimuli experienced by platelets as they traverse the LV. Twice as many platelets accumulated very high SH in the LVAD + AF case, resulting in a 36% increase in thrombogenic potential score, relative to the LVAD + SR case.
Conclusions:
This supports the hypothesis that AF results in unfavorable blood flow patterns in the LV adding to an increased stroke risk for LVAD + AF patients. Quantification of thrombogenic risk associated with AF for LVAD patients may help guide clinical decision-making on interventions to mitigate the increased risk of thromboembolic events.
Keywords
Introduction
Left ventricular assist device (LVAD) utilization continues to increase due to a high prevalence of medical-therapy refractory stage-D heart failure (HF) and a stagnant donor heart supply.1,2 While advances in technology and improvements in LVAD design have resulted in 1-year survival of LVAD patients approaching 90%, devastating complications such as cerebrovascular and other thromboembolic events remain undesirably high.2 –5 Atrial fibrillation (AF) is a common co-existing condition with HF, and approximately 57% of HF patients develop AF.6,7 Since AF alone is a well-established risk factor for stroke,8 –11 it can potentially exacerbate risk in the setting of LVAD therapy. Quantifying the thrombogenicity of intraventricular flow patterns in the setting of AF in LVAD therapy is the intended goal of this study.
Several studies have associated the presence of AF with increased mortality, morbidity, and significant clinical burden, however there is limited information available to assess the combined effect of LVAD and AF on thrombogenic risk.12 –15 More recently, researchers have sought to analyze the combined influence of AF and LVAD therapy on stroke risk with varying results. 16 The MOMENTUM3 trial did not find correlation between stroke risk and preexisting or new AF for HF patients implanted with the HeartMate 3. 17 A smaller, single-center study found that post-operative AF (POAF) did not negatively impact early postoperative morbidity, but was found to be a predictor for future AF, ischemic stroke, and device thrombosis. 12 A recent article highlighted the conundrum of determining treatment for LVAD patients with AF due to the lack of data and mechanistic understanding of this phenomenon in this population. 18 Thus, there is an unmet clinical need to evaluate the thrombogenic risk of LVAD patients with AF.
Mechanistic prediction of thrombogenic risk requires detailed knowledge of the hemodynamics environment in the left ventricle (LV). Unfavorable hemodynamic patterns in the LV due to various factors such as inflow cannula angulation, LV size, and residual LV contractility can predispose platelets to aggregate prior to entering the LVAD.19,20 The presence of AF adds to this milieu of risk factors due to the irregular and potentially unfavorable flow patterns in the LV. Given the variety of factors influencing blood flow within the LV, it is essential to evaluate each of them independently, followed by a combined risk analysis. Though some studies exist that evaluate atrial and LV hemodynamics in the presence of AF, they use incomplete estimates of slow-moving flow for stasis and thrombus initiation, often based on endothelial (Eulerian) wall shear-derived metrics to characterize hemodynamics.21 –25 Moreover, they do not focus on the combined effects of LVAD and AF on thrombogenicity. Thrombogenicity prediction based on platelet-focused (Lagrangian) simulations that track individual platelets and accurately compute platelet residence times (RT) and shear stress accumulation can yield both a mechanistic understanding of AF contribution to intraventricular platelet activation and aggregation.26 –28 Our group has previously published a series of detailed thrombogenic risk analysis for various anatomical and surgical factors toward developing a clinically-translatable risk stratification tool.19,20,29,30
In this study, we hypothesize that AF increases thrombogenic risk in the setting of LVAD implantation. This is done by comparing the intraventricular flow patterns of a patient-derived LVAD + AF case over 20 chaotic cardiac cycles to the intraventricular blood flow for an anatomically identical case in sinus rhythm (LVAD + SR). To characterize the differences in intraventricular flow patterns and quantify thrombogenicity, we estimate thrombogenic indices from platelet RT and shear stress history (SH). This approach is device-neutral and clinically translatable to AF patients treated with LVAD. This can provide valuable insights into the combined effect of LVAD and AF on intraventricular blood flow.
Methods
Virtual surgery
Image segmentation was performed on computed tomographic images of a patient (70 kg male with non-ischemic cardiomyopathy and LV end-diastolic diameter of 7 cm) as approved by the IRB and after obtaining informed consent, to obtain the anatomic LV model. A representative LVAD inflow cannula was virtually implanted apically in the LV, as described previously. 19
Modeling intraventricular hemodynamics
Blood is simulated in this high Reynolds number/high mean shear flow as a homogeneous Newtonian fluid. The 3D time-resolved Navier-Stokes equations are solved to simulate fluid flow inside the LV. Very high spatial O(200 μm) and temporal O(10−4 s) resolutions are used to capture the unsteady, and sometimes chaotic, nature of flow in the LV and the hemodynamics stimuli exerted on platelets. For the LVAD + SR case, echo Doppler-derived mitral valve (MV) inflow was prescribed. 19 For the LVAD + AF case, a virtual chaotic waveform representative of AF was applied after consultation with electrophysiology experts (Figure 1). Time-averaged flow rate for both cases (LVAD + SR and LVAD + AF) was 5 L/min, and the CFD simulation was performed for 20 cardiac cycles. The aortic valve (AV) was assumed to be closed for the duration of the simulation, representing complete LVAD support.
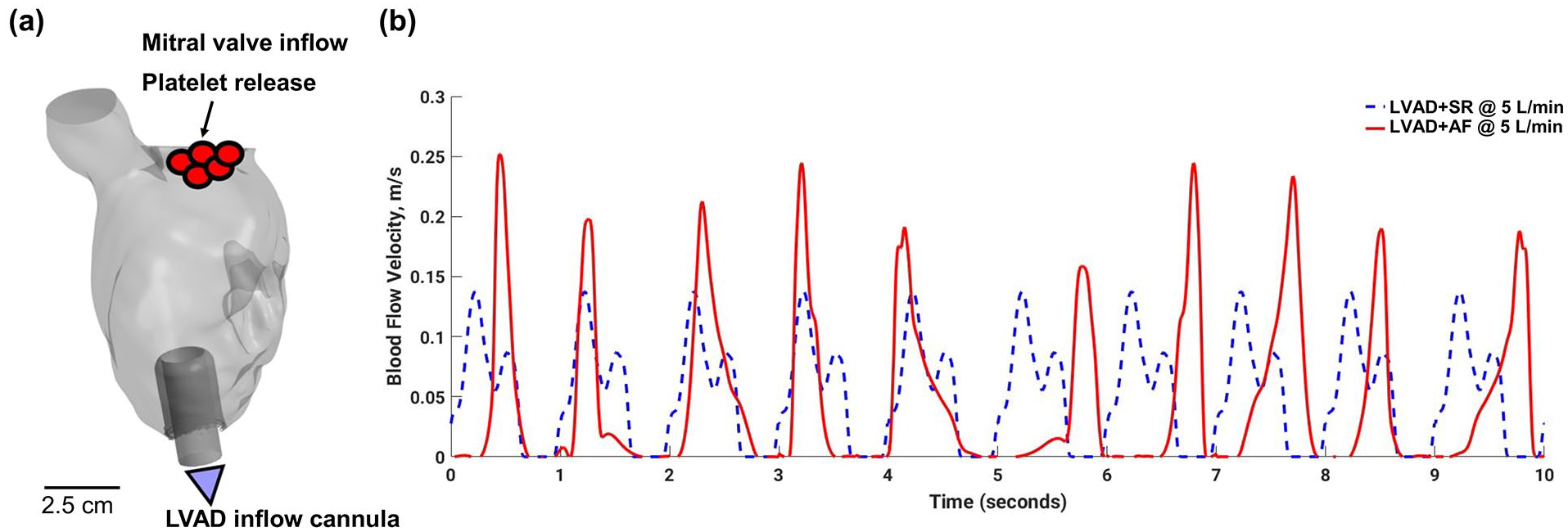
(a) Intraventricular 3D flow model of an LVAD-implanted left ventricle (b) mitral valve inlet waveform comparing sinus rhythm inlet condition (dotted line) and AF (solid line) used in the computational simulations.
Platelets, modeled as inertialess tracer particles were injected at the MV every 1/10th s for 10 cardiac cycles—in total, over 100,000 platelets were individually tracked. Platelet trajectories were reconstructed from their positions as they traversed the LV. While platelet activation is a multi-factorial phenomenon, it is widely accepted that shear-induced platelet activation (SIPA)—incorporating platelet RT and shear exposure—is of significant importance in evaluating thrombogenicity for mechanical circulatory support devices such as LVADs.27,31 –33 Thus, for each platelet, RT was calculated based on the length of time that it remained within the LV:

Where
Since each platelet trajectory is individually computed using Lagrangian tracking, it is possible to quantify the shear exposure integrated during its transit:

Where
Thrombogenic potential estimation
Thrombogenic potential (TP) for both cases (LVAD + SR and LVAD + AF) was quantified combining platelet RT and SH median and outlier metrics that adversely influence thrombogenicity.19,20,35
Results
Blood flow patterns
Flow in the LV is highly dynamic owing to the pulsatile inflow from the MV, forming an unsteady jet that propagates from the valve toward the apex, and an LVAD-induced drainage at the apex. Blood entering the LV splits into multiple streams as the unsteady jet breaks down, with a central core traveling directly toward the inflow cannula. Blood peripheral to the central core swirls around the LV before converging toward the inflow cannula, while the blood between the cannula and the apical ventricular space flows slowly around the cannula base and takes extended time to leave the LV, making this apical cannula pocket a quasi-stagnation zone. These intraventricular flow patterns including the presence of quasi-stagnation zones at the apex and the space beneath the closed AV, are generally present for both cases. However, in the LVAD + AF case, flow is more chaotic owing to the irregularity in the mitral inflow (Figure 2). This causes pockets of blood to break up into multiple streams that travel either toward the inflow cannula (if they are in the central core of the LV) or are slow-moving flow regions near the LV walls. This is markedly different than a central core traveling toward the inflow cannula during mitral systole seen in the SR case. As a consequence, the hemodynamics stimuli acting on platelets is significantly different due to the chaotic and irregular intraventricular flow, in which platelets experience abnormal RT and SH over multiple cardiac cycles in AF.
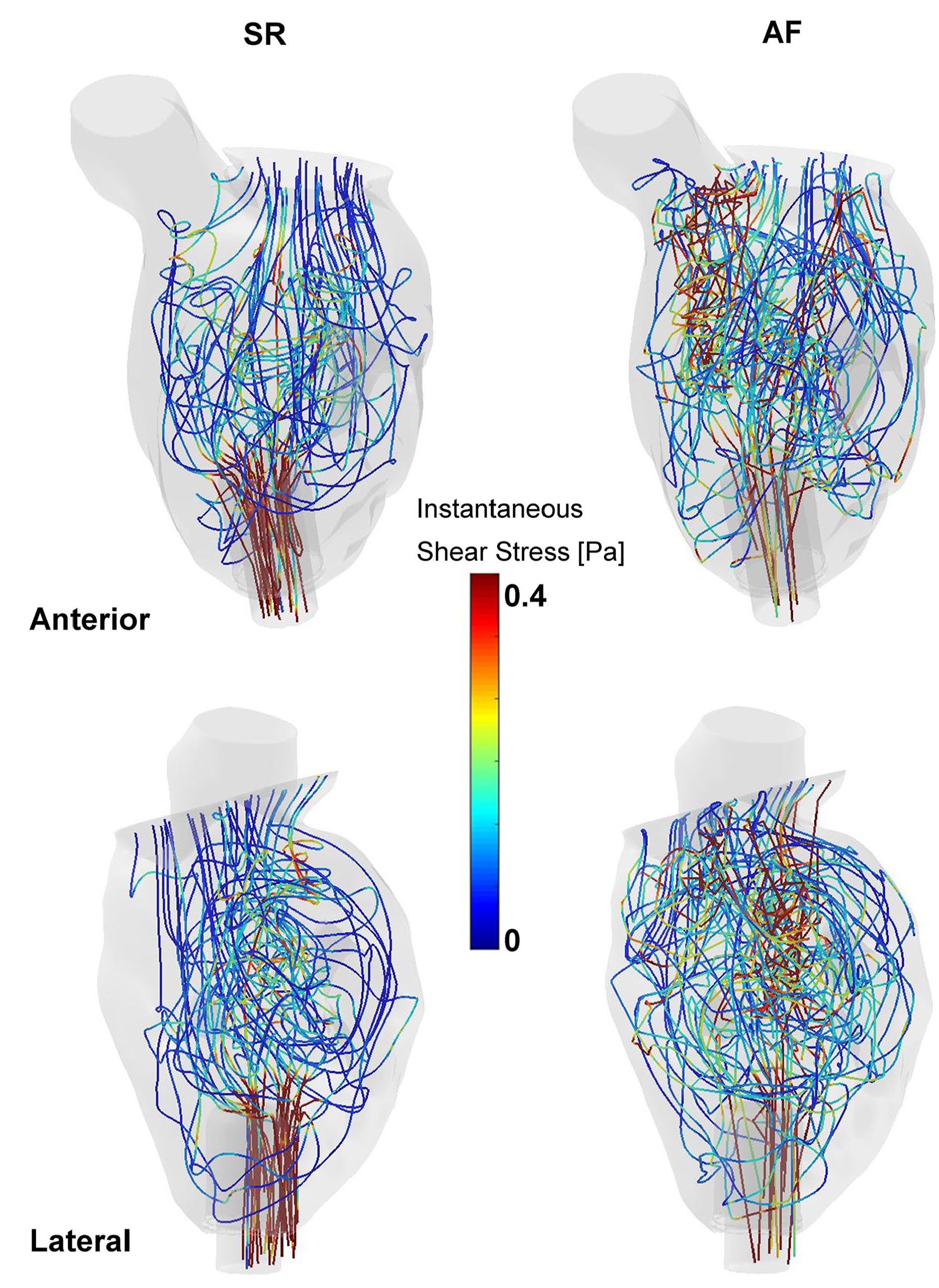
Representative platelet trajectories for the LVAD + SR (left column) and LVAD + AF (right column) cases depicting the instantaneous shear exposure that they experience as they traverse the LV. Due to the irregular and chaotic intraventricular flow, platelets in the LVAD + AF case experience a greater variation of instantaneous shear stress, potentially increasing thrombogenic risk.
Platelet metrics
For each case (LVAD + SR and LVAD + AF), over 100,000 platelets were individually tracked for 20 s to obtain detailed platelet metrics. Platelets traverse the LV in complex paths that often involve circulating around the apical zone surrounding the LVAD inflow cannula multiple times. During their transit, platelets pass through regions of high shear such as the central core during mitral peak flow and low shear such as recirculation and stagnation zones along their individual trajectories. Thus, each platelet experiences a heterogeneous spatio-temporal exposure of hemodynamics stimuli (RT and SH) that contribute to its overall activation state. Trajectories for platelets in the LVAD + AF case are more tortuous due to the chaotic nature of flow in AF; this translates to a greater exposure of alternating acceleration and deceleration that not only results in particles getting trapped in recirculation zones for longer times, but also accumulate higher shear during their transit.
After 15 s, median RT for the LVAD + AF case (median 2.42 s) was more than 15% longer (statistically significant) compared to the LVAD + SR case (median 2.09 s) indicating that, on average, particles in the LVAD + AF case lingered for longer as they traversed the intraventricular space, as seen in Figure 3. To compare the long tails of the platelets RT distribution throughout the duration of the simulation, an arbitrary threshold of 5 s was chosen to define a long residence time (LRT) zone, with less than 1% of platelets in this zone. Using this threshold, twice as many platelets from the LVAD + AF case were found to be in the LRT zone compared to the LVAD + SR case, indicating higher risk of activation and aggregation, as shown in Figure 4. Different RT thresholds provide qualitatively the same result, with small quantitative variations in the AF-induced increases.
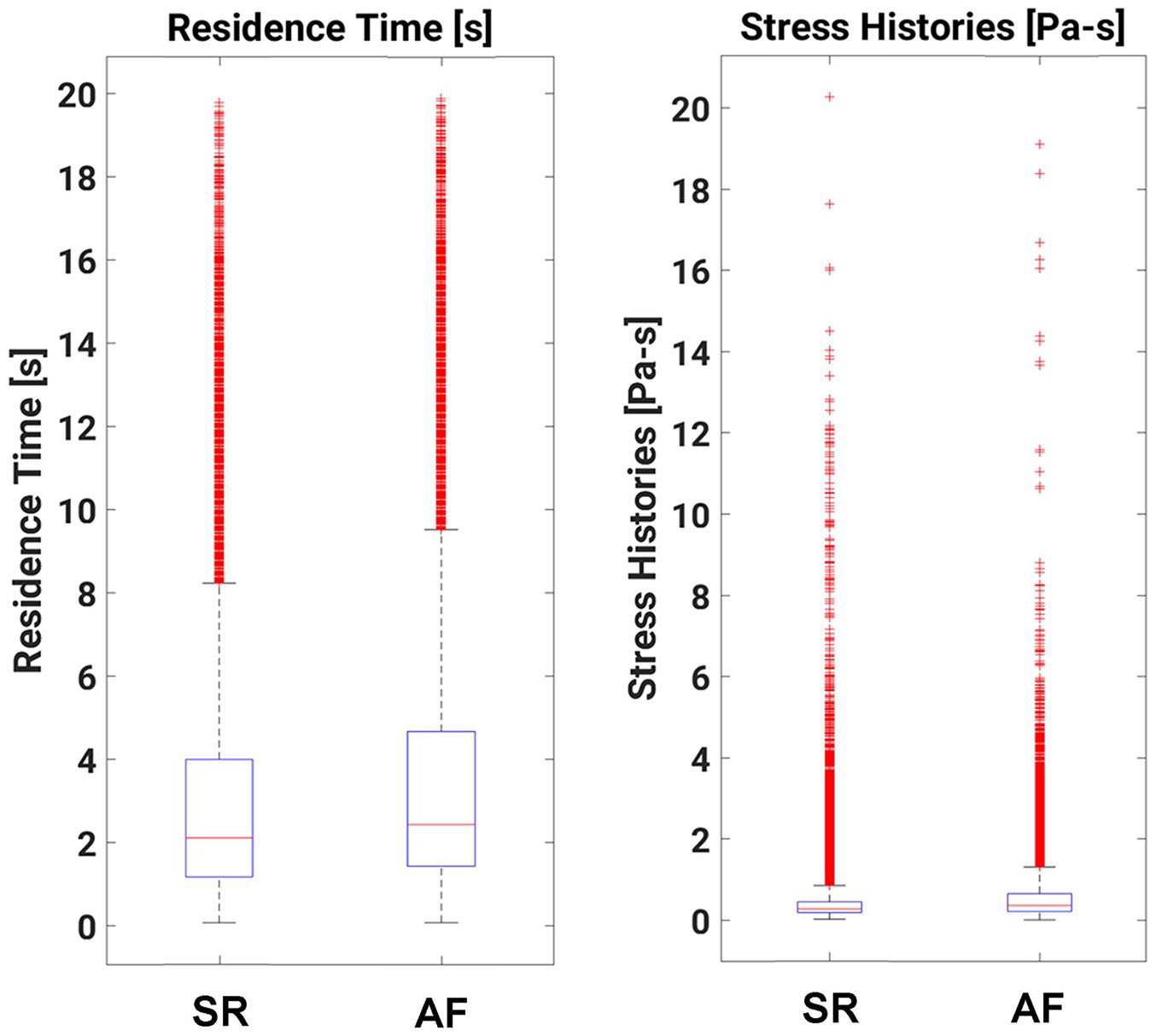
Boxplots of platelet RT (left) and SH (right) for the two cases analyzed in this study indicating a statistically significantly higher RT and SH (both median and in the percentage of high-valued outliers) for platelets in the LVAD + AF case.
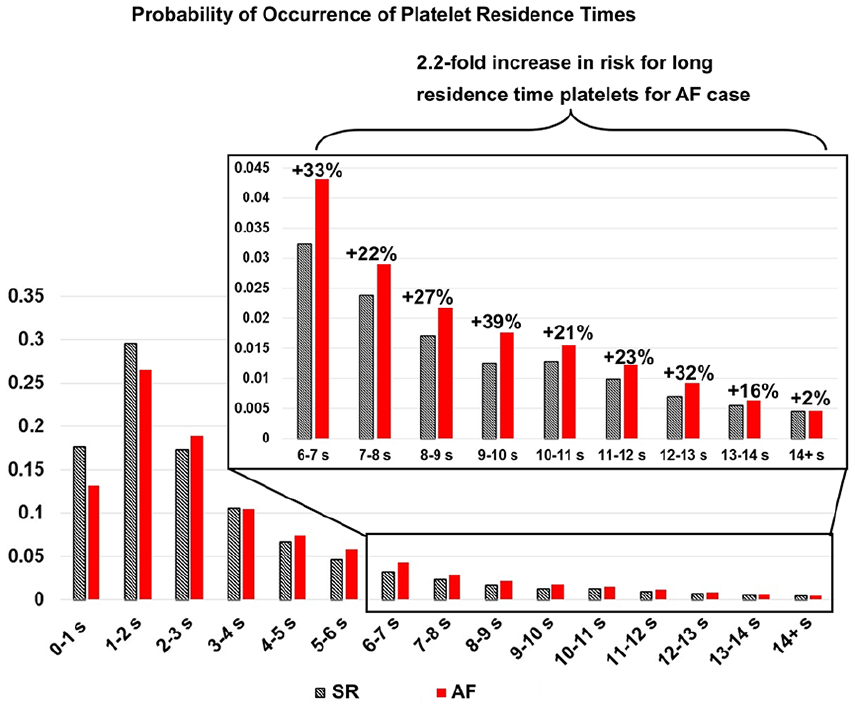
Probability of occurrence plot showing an increased risk (2.2 fold) of platelets circulating for increased length of time for the case with LVAD + AF.
Median SH accumulated by the particles followed a similar trend. Platelets in the AF case (median 0.36 Pa s) experienced more than 38% higher shear stress accumulation compared to the LVAD + SR case (median 0.26 Pa s) on average. To study the outliers statistically, a threshold of 3 Pa s was chosen to delineate the zone of high shear history (HSH), with less than 1% of platelets in this zone for either of the LVAD + AF and LVAD + SR cases. Figure 5 shows both RT and SH metrics for each platelet tracked in both cases. The LRT (RT >5 s) and HSH (SH >3 Pa s) zones intersect in the upper right quadrant, giving rise to a high thrombogenicity (HT) zone. There was a 2× increase in platelets for the LVAD + AF case residing in the HT zone, compared to the LVAD + SR case, revealing a higher thrombogenic potential due to the presence of AF.
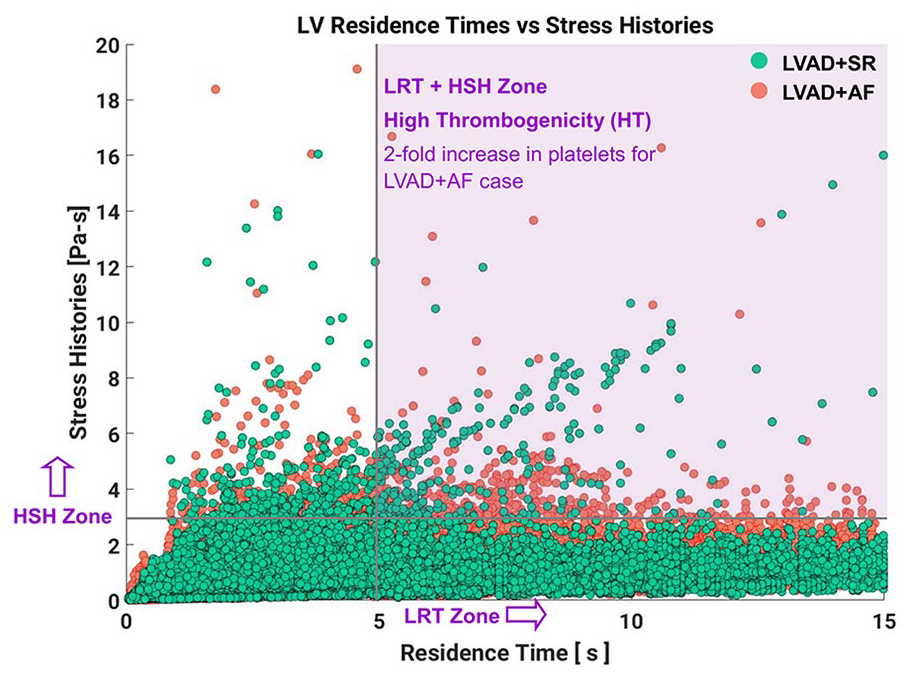
Cross correlation analysis of particle RT and SH, demonstrating that a much higher percentage of platelets occurring in the high thrombogenicity (long RT + high SH) zone for the LVAD + AF case, indicating increased thrombogenic risk.
Thrombogenic potential estimation
We estimated the thrombogenicity for the AF and SR cases using a previously published methodology19,34 that incorporates both RT and SH platelet metrics, shown in Table 1. Since the long tails of the RT and SH distributions are of interest and present the most likely conditions for platelet aggregation and activation, we have incorporated the outliers as follows: using the LVAD + SR case as the reference, cutoffs were determined for the top 5% of platelet outliers for both RT and SH. The same cutoffs were used to determine the percentage of platelets from the LVAD + AF case that cross this threshold. This is presented as a ratio of top 5% outlier cutoffs: for example, the ratio of 2.17 for SH indicates that for the same cutoff level, there are more than twice as many platelets occurring in high SH exposure for the LVAD + AF case. The TP score is normalized to compare the relative risk, for risk stratification purposes, between a minimum of 0 and a maximum of 1. The LVAD + SR case receives a TP score of 0.64, while the LVAD + AF case is assigned a TP score of 1, indicating that the LVAD + AF case is significantly more thrombogenic.
Thrombogenic Potential Score for LVAD + SR and LVAD + AF cases.

Discussion
Undesirably high thromboembolic complications continue to hinder the success of LVAD therapy despite significant improvements in LVAD technology and design.3,4,36 Blood flow in the LV implanted with an LVAD is highly non-physiological and is influenced by several factors as and our group and others have shown.19,20,33,34,37 There is however a lack of understanding of the mechanisms by which AF (itself a major stroke risk factor) and LVAD physiology interact and, therefore, no consensus on the best path to treat LVAD + AF patients.6,7,12,38 Thus, it is critical to evaluate the contribution of AF as a risk factor to estimate the overall thrombogenicity of LVAD therapy.
Two cases are compared, sinus rhythm (LVAD + SR) and atrial fibrillation (LVAD + AF). Our platelet-tracking analysis enables quantifying the detailed stimuli on platelets traversing the LV, such as RT and SH which have been strongly implicated in SIPA. Keeping all other parameters such as LV size, inflow cannula angle, extent of LVAD support, and average flow rate fixed, we evaluate the sole influence of a chaotic, irregular mitral flow, simulating AF, for an LVAD patient and demonstrate that the intraventricular flow patterns associated with AF strongly increase thrombogenic risk.
The presence of concomitant AF results in markedly different intraventricular hemodynamics. Due to the irregular and chaotic flow through the MV, blood in the LV experiences multiple cycles of unsteady jets forming at the MV and detaching and breaking down in the LV, which result in platelets experiencing increasingly disruptive biomechanics stimuli. Platelets in the LVAD + AF case circulate in the LV for up to 15% longer on average than in the LVAD + SR case. This trend was mirrored for shear exposure—platelets in the LVAD + AF case accumulated more than 38% higher median shear on average than in the LVAD + SR case. Since platelet aggregation is dependent on the interplay between RT and SH, we delineate LRT and HSH zones, using arbitrary thresholds of RT >5 s and SH >3 Pa s, respectively, and find the joint probability of finding platelets in both zones, as these platelets will be the outliers that start the clotting cascade and trigger thrombosis. The intersection of these zones gives rise to the HT zone where platelets have increased risk of activating, as they accumulate very high SH, and then aggregating, as they spend longer time in the LV. Our analysis revealed that there is a two-fold increase in the risk of platelets occupying the HT zone for the LVAD + AF case compared to the LVAD + SR case, resulting in an overall higher TP for the LVAD + AF case.
Our analysis reveals the complex interdependence between intraventricular flow patterns and platelet mechanical stimuli. Due to the chaotic nature of flow through the MV for the LVAD + AF case, platelets are subjected to repeated cycles of intense acceleration and deceleration as they traverse the LV, consequently leading to increased RT and shear exposure along their trajectories. Moreover, the combination of high velocity jet-like from the MV toward the ventricular apex (which is more pronounced in the AF case) leads to not only high shear exposure initially, but also regions of stagnation near the apical pocket surrounding the LVAD inflow cannula. This phenomenon is due to a sequence of fast-moving flow emanating from the MV repeatedly getting trapped in recirculating regions near the LV apex. The isolation can become exacerbated because the next irregular bolus of blood enters the LV and meanders into a different region of the LV, reaching the cannula before the isolated blood from the previous diastolic filling has sufficient time to drain into the LVAD inflow cannula. Thus, there exists regions of quasi-stagnation and recirculation, most notably near the ventricular apex, and also below the AV. These could form an aggregation zone for activated platelets. Such unfavorable intraventricular flow would continue to exist as long as AF is not treated.
Treating AF in the LVAD population remains a clinical unknown.16,18 AF is strongly linked with increased thromboembolic complication risk, and care of AF patients remains an active clinical and basic science research topic.9,39 –42 The superposition of AF with LVAD therapy further complicates assessment of thromboembolic risk and, thus, the design of effective treatment strategies. Anecdotal evidence indicates a strong link between coexisting and POAF and thromboembolic complications for HF and LVAD patients. In a 2013 study, authors demonstrated that, among HF patients undergoing LVAD implantation, the presence of pre-operative AF was a significant risk factor for thromboembolic events—25% of patients had some form of thromboembolic complication including pump thrombosis and cerebrovascular events. 38 Yet another recent study concluded that preoperative AF resulted in a lower freedom from thromboembolic events after LVAD implantation, indicating a link between preexisting AF and LVAD therapy on stroke risk. 38 Our study clearly demonstrates increased thrombogenic risk of platelet aggregation and activation for LVAD + AF patients compared to LVAD + SR patients (up to a 36% increase in risk) by rigorously analyzing the platelet hemodynamics microenvironment in the LV. Thus, the results from this study provided quantitative support for the hypothesis that AF presents an increased risk of thromboembolic events in patients implanted with an LVAD.
Limitations
The lack of modeling the left atrium flow, with the potential to seed thrombi of different sizes (microthrombi or fully mature thrombi detached from the atrial wall, is a major limitation. It does not negate, however, these results, but rather would exacerbate the increased thromboembolic risk as the thrombi formed in the left atrium suffering atrial fibrillation would grow and trigger more thrombogenecity in the LV, multiplying the effect of AF beyond the effect found here.
The MV inflow waveform for the LVAD + AF case was synthetically generated in consultation with our clinical collaborators. Due to the wide variation in AF waveforms, future studies will incorporate additional variations to quantify AF-waveform-specific thrombogenic risks.
Intermittent AV flow is also known to influence thrombogenicity for LVAD patients; we envision future models to incorporate these effects. Future models will also incorporate platelet-platelet signaling and aggregation models.
Conclusions
The presence of AF increases thrombogenic risk for LVAD patients. Using high-fidelity CFD simulations incorporating platelet Lagrangian tracking, this study characterizes in detail the hemodynamics stimuli and blood flow patterns within the LV for a representative LVAD + SR and LVAD + AF case. Platelets in the LVAD + AF case had a two-fold increased risk of being subjected to long RT and high SH compared to the LVAD + SR case. This indicates a higher risk of platelet aggregation, activation, and subsequent thromboembolic events for the LVAD + AF case, resulting in a 36% higher TP for LVAD + AF patients. Such analyses can help the clinical and overall research community determine efficient methods to combat the increased thrombogenic risk due to AF for LVAD patients. Maintaining SR may help reduce adverse events and improve outcomes.
Footnotes
Author contributions
VKC performed the computational simulations, analyzed the blood flow and platelet data, and wrote the manuscript, JB, SL, NA, AA, and CM provided guidance on the clinical and engineering perspectives and helped write the manuscript.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: CM is an investigator/consultant for Abbott, Abiomed, and Endotronix. VKC, JB, SL, NA, and AA have no disclosures.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported in part by an American Heart Association postdoctoral fellowship (16POST30520004) to VKC.
List of non-standard abbreviations
LVAD: Left Ventricular Assist Device
HF: Heart Failure
AF: Atrial Fibrillation
LV: Left Ventricle
CFD: Computational Fluid Dynamics
RT: Residence Time
SH: Shear History
SR: Sinus Rhythm
LVAD + AF: Left Ventricular Assist Device with Atrial Fibrillation Case
LVAD + SR: Left Ventricular Assist Device with Sinus Rhythm Case
AV: Aortic Valve
TP: Thrombogenic Potential
SIPA: Shear Induced Platelet Activation
LRT: Long Residence Time
HSH: High Shear History
HT: High Thrombogenicity