
Abstract
Background:
Donation after brain death (DBD) serves as the primary source for liver transplantation. However, livers obtained through DBD often incur damage due to unstable hemodynamics, potentially impacting transplantation outcomes. Extracorporeal Membrane Oxygenation (ECMO) emerges as an optimal technique for donor liver retrieval and has found application in clinical settings. Despite its clinical implementation, the precise mechanisms through which ECMO enhances liver functions remain elusive. This study aims to investigate the mechanisms underlying how ECMO ameliorates liver function in brain-dead donors.
Methods:
We randomly assigned 18 male Sprague-Dawley (SD) rats (350 ± 50 g) into three groups: Con (n = 6), DBD-assisted drug (n = 6), and DBD-assisted ECMO (n = 6). After 3 h of ECMO, the rats were sacrificed. We assessed and compared changes in heart rate, blood pressure, cumulative liver damage (evaluated through HE and TUNEL staining), serum levels of AST and ALT, alterations in serum oxidative stress factors (MDA, H2O2, SOD, and 8-OHdG), and serum concentrations of related inflammatory factors (interleukin [IL]-1β, IL-6, IL-8, and TNF-α) among rats in the Con, DBD-assisted drug, and DBD-assisted ECMO groups. Subsequently, we established a rat orthotopic liver transplantation (OLT) model and transplanted livers obtained through the aforementioned methods. The post-transplantation status of the livers was observed.
Results:
After 3 h of brain death, liver injury worsened, accompanied by a significant increase in serum transaminases, inflammatory responses, oxidative stress, and TUNEL staining. Strikingly, ECMO not only stabilized hemodynamics after DBD but also mitigated liver damage, leading to an alleviated status post liver transplantation.
Conclusions:
ECMO stabilizes hemodynamics, attenuates inflammatory responses and oxidative stress, thereby enhancing the quality of liver grafts for transplantation.
Introduction
Liver transplantation stands as an effective treatment for various end-stage liver diseases, encompassing conditions like liver failure, alcoholic liver disease, and liver cancer. The feasibility of liver transplantation relies on both living and deceased organ donations. Despite the success of living organ donation, ethical concerns, significant surgical risks, and potential economic implications pose challenges to its widespread implementation. Consequently, attention has shifted toward deceased donation, which includes donors after brain death (DBD) or circulatory death (DCD). Deceased donor organs predominantly originate from individuals declared dead by neurological criteria.
Clinical and experimental studies unveil a multitude of pathophysiological changes during brain death, encompassing hemodynamic instability, hormonal imbalances, leukocyte infiltration, cytokine and chemokine induction, loss of blood pressure autoregulation and sympathetic tone, and reduction in systemic vascular resistance. Additionally, macro- and microcirculation to the liver diminishes, escalating hepatic oxidative stress and inducing ischemic-hypoxic conditions, 1 particularly in potential donors experiencing explosive brain death. The use of vasoactive drugs, such as norepinephrine and dopamine, becomes imperative for maintaining hemodynamic stability. However, high doses of these drugs may exacerbate liver injury, compromising the quality and tolerance of liver grafts to preservation or reperfusion injury, and aggravating liver ischemia-reperfusion (I/R) injury post-transplantation, ultimately reducing graft survival rates.2,3
Extracorporeal Membrane Oxygenation (ECMO) or partial cardiopulmonary bypass serves to temporarily support the respiratory and cardiac functions of patients unresponsive to maximal medical therapy for cardiac failure. Increasingly, ECMO is employed to maintain DBD organs.4,5 The excessive administration of vasoactive catecholamine drugs to achieve hemodynamic stability after brain death leads to oxidative stress. ECMO, however, eliminates the need for vasopressor agents, preventing damage to liver grafts. 6 Furthermore, it improves organ perfusion by increasing the partial pressure of arterial oxygen and reducing lactic acid levels. In cases of DBD with respiratory failure, ECMO prevents circulatory instability by providing additional blood oxygenation.7–10
Despite the potential benefits, the debate persists due to a lack of evidence demonstrating whether ECMO can enhance liver functions in DBD patients. Hence, this study aims to establish a DBD-assisted ECMO rat model and comprehensively assess hemodynamics, pathology, liver functions, oxidative stress, and related inflammatory factors. Additionally, the study seeks to validate whether ECMO can indeed improve liver functions post-DBD and elucidate the molecular mechanisms underlying its actions.
Methods
Animals
All animals were treated according to the “Principles of laboratory animal care” formulated by the National Society for Medical Research and the “Guide for the care and use of laboratory animal resources” published by the US National Institute of Health (NIH publication No. 85-23, revised 1996). All experimental protocols were approved by the local Ethical Committee of Lanzhou Second Hospital, Lanzhou University, Gansu.
Anesthesia
The rats of all groups were anesthetized in a plexiglass chamber using 5% sevoflurane in oxygen for 3–5 min. The rats were mechanically ventilated in a volume-controlled manner at a respiratory rate of 70–75 breaths/min, tidal volume of 6 mL/kg, and positive end-expiratory pressure of 2 cmH2O. Surgery was performed under aseptic conditions and all surgical fields were then infiltrated with 1% lidocaine.
Brain death model
A Fogarty 3F balloon catheter (Medtronic Inc, USA) was introduced through the front lateral trepanation into the intracranial cavity with the tip pointing caudally. Using a syringe pump, the balloon was inflated by saline solution with rapidly to increase the intracranial pressure in a short time, compression was stopped when the electroencephalogram (EEG) showed a straight line. This eventually induced progressive brain injury and thereafter explosive brain death. Occurrence of an autonomic storm, absence of corneal reflexes, and dilated and fixed pupils, followed by an apnea test were used for the clinical diagnosis of brain death. In this study, only animals with unstable mean arterial blood pressure (MAP ⩽ 60 mm Hg) were considered eligible as subjects.
ECMO model
The ECMO circuit 11 used in this study comprised a peristaltic pump, membrane oxygenator (oxygenation area 0.02 m²), and tubing, along with 22- and 24-G catheters, and a specially designed catheter. The circuit was pre-primed with a bloodless solution (3 mL of pure colloid, hydroxyethyl starch 130/0.4 in saline). We inserted a 24-G catheter into the left femoral artery of rats to continuously monitor the arterial pressure, while a 22-G catheter was inserted into the right femoral artery for continuous arterial perfusion. The right jugular vein was cannulated with a specially designed catheter for venous return. Venous return blood was transported using a roller pump to the membrane oxygenator for oxygenation and subsequently perfused systemically through the right femoral artery. Heparin was administered to the rats at a dose of 300 U/kg at the beginning of the procedure. Sodium bicarbonate (5%, 1 mL) was added to the circuit during ECMO to maintain acid-base balance. Additionally, all substituting or buffering solutions were administered via the left femoral artery. The central temperature was monitored using a rectal probe and maintained at 36 ± 0.5°C with a heating blanket. Initially, the ECMO flow rate was set at 80–90 mL/kg/min and adjusted as needed to maintain the desired arterial pressure. After 3 h of ECMO, the animals were weaned off the support.
Rat orthotopic liver transplantation
The donor liver was carefully isolated, and the recipient rat underwent meticulous hepatectomy to create a suitable space for graft placement. Vascular anastomoses were performed, connecting the hepatic artery and portal vein of the donor liver to those of the recipient. Bile duct reconstruction was carried out to establish biliary continuity. The entire procedure was conducted under strict aseptic conditions to minimize the risk of infection. Post-transplant, the rats were closely monitored for signs of rejection or complications, and appropriate measures were taken.
Hematoxylin-eosin (HE) staining pathology injury score
The HE slides were scanned and four images were randomly selected from each slide and corresponding areas. Blinded observers scored each image accordingly. Nuclear damage, tissue vacuolization, hepatocyte vacuolization, and congestion were the criteria for liver damage.
Enzyme-linked immunosorbent assay (ELISA)
We measured the levels of interleukin-1β
Immunohistochemistry (IHC)
The liver tissues were obtained and fixed in 4% paraformaldehyde for 24 h. Then, the sections were subjected to high-pressure antigen retrieval. Further, we incubated the sections with endogenous peroxidase blocker (Zhongshan Golden Bridge Biotechnology, Beijing, China) for 20 min to inactivate the endogenous peroxidases. While for blocking non-specific binding, the sections were incubated with a blocking reagent (Zhongshan Golden Bridge Biotechnology) for 20 min. Next, the sections were incubated with rabbit
anti-myeloperoxidase (MPO) (Proteintech,22225-1-AP, 1:100) and rabbit anti-CD68 (Proteintech,28058-1-AP, 1:500) primary antibodies at 4°C overnight. Thereafter, the sections were incubated with goat anti-rabbit IgG (Zhongshan Golden Bridge Biotechnology) secondary antibody at 37°C for 15 min. Further, the sections were visualized with 3,3′-Diaminobenzidine (DAB) for a few seconds before they were counterstained with hematoxylin. Finally, we calculated the average number of activated cells in the liver.
TUNEL analysis
We conducted the TUNEL assay using the TUNEL detection kit (TUNEL, Beyotime) according to the manufacturer’s instructions. Briefly, liver sections were fixed in 4% paraformaldehyde at room temperature for 30 min. Then, the sections were washed with Phosphate Buffered Saline(PBS)followed by treatment with 0.3% Triton X-100 for 15 min. Subsequently, 50 µl of the TUNEL reaction mixture (5 µl TdT enzyme solution and 45 µl labeling solution) was added to the samples. The resulting mixture was incubated at 37°C for 1 h in a dark and humidified environment. Finally, the cells were co-stained with 4,6-diamino-2-phenyl indole (DAPI) and visualized using an Olympus FV3000 confocal microscope.
Statistics
All statistical analyses were conducted using GraphPad Prism 7.0. Data were presented as mean ± standard error (SE) of the mean. The Shapiro-Wilk test was used to determine the normality of data. We used an unpaired Student’s t-test to compare two groups of data having normal distribution and similar variances. The Mann-Whitney U test was used for data showing abnormal distribution. A two-tailed p-value of <0.05 was considered statistically significant.
Results
Establishing a DBD-assisted ECMO rat model
Figure 1(a) shows the schematic illustration of the ECMO assisted-DBD model. Briefly, after anesthetizing the rats, the intracranial balloon and ECMO vascular cannula were prepared, and progressive mechanical intracranial hypertension induced brain death. ECMO intervention was initiated when the hemodynamics were unstable, such as mean artery pressure (MAP) ⩽60 mmHg, or ineffective action of a large amount of vasoactive drug. After 3 h, ECMO was stopped and liver tissues were collected. The heart rate and blood pressure of the rats were measured throughout the procedure. Figure 1(b) depicts a flowchart of the experimental process.
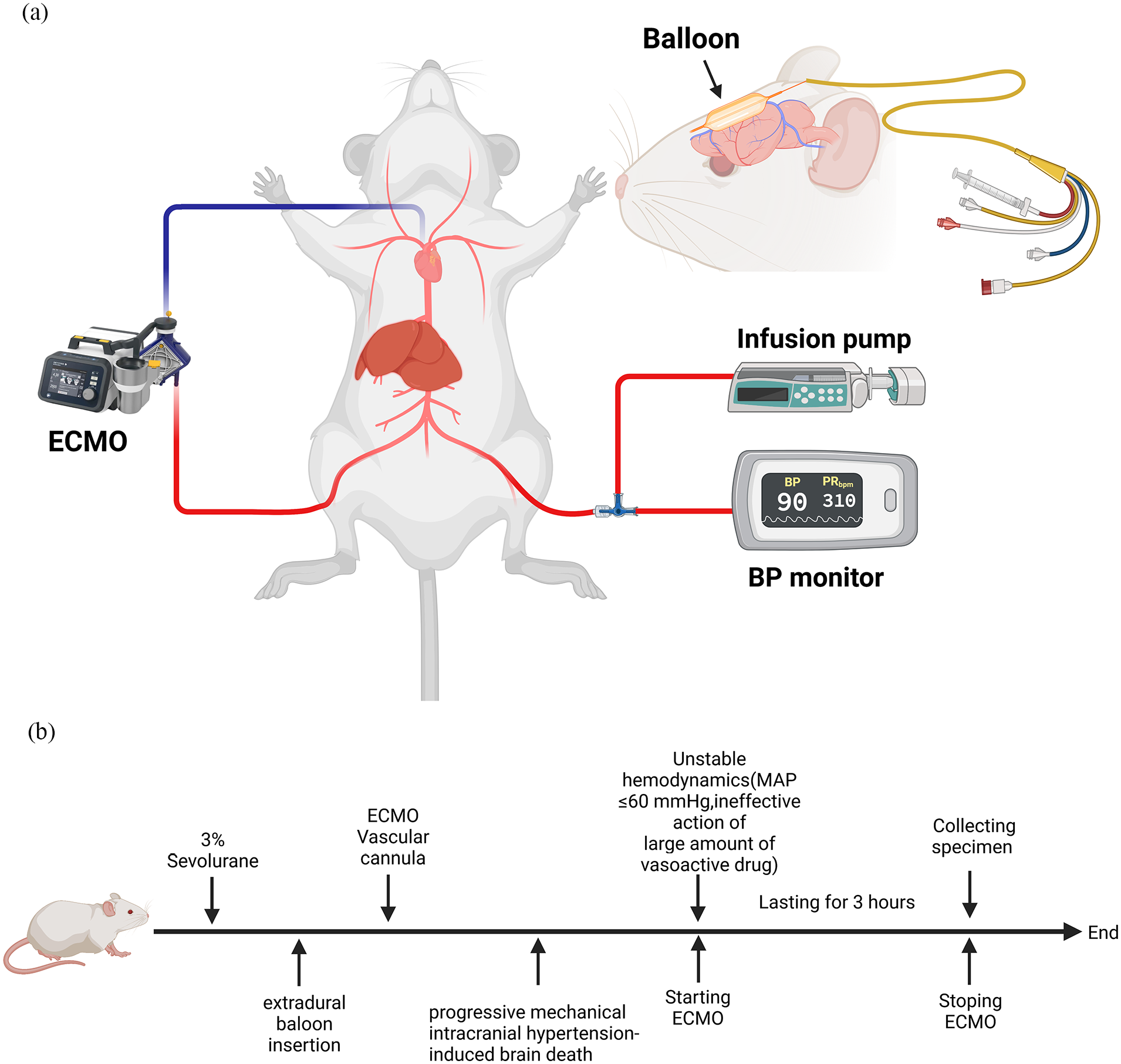
Flow chart and schematic diagram of experimental operation: (a) schematic diagram of the rat model of brain death supported by ECMO and (b) flow chart of the establishment of experimental models.
ECMO stabilized hemodynamics after brain death
After balloon compression, the blood pressure increased, peaked at the fifth minute, and then slowly declined in both, DBD-assisted drug and DBD-assisted ECMO groups. The peak blood pressure was 182 ± 9.64 mmHg in the DBD-assisted drug while 179 ± 7.55 mmHg in the DBD-assisted ECMO group. At the 10th minute, the blood pressure was 54.67 ± 3.06 mmHg in the DBD-assisted drug and 54.67 ± 3.79 mmHg in the DBD-assisted ECMO group. Additionally, the rats showed an absence of corneal reflexes, dilated and fixed pupils, and a positive apnea test in all groups. At this time, we started ECMO in the DBD-assisted ECMO group. ECMO stabilized the blood pressure and avoided the need of vasoactive drugs to maintain hemodynamics. While the DBD-assisted drug required an average of three injections of vasoactive drugs (norepinephrine) throughout the trial when MAP ⩽60 mmHg (Figure 2(a)). Similarly, the heart rate rapidly increased after balloon compression and the peak value was 411.67 ± 9.5 bpm in the DBD-assisted drug while 418 ± 3.61 bpm in the DBD-assisted ECMO group at the fifth minute (Figure 2(b)). The heart rate remained stable after ECMO support and was 323.33 ± 7.51 bpm by the end. However, the heart rate of the DBD-assisted drug showed significant fluctuations throughout, especially, a significant increase after the injection of vasoactive drugs. Table 1 summarizes the physiological data obtained during the process. In conclusion, we established a mature and stable model of ECMO support after brain death in rats. Moreover, ECMO maintains hemodynamic stability and reduces the use of vasoactive drugs.
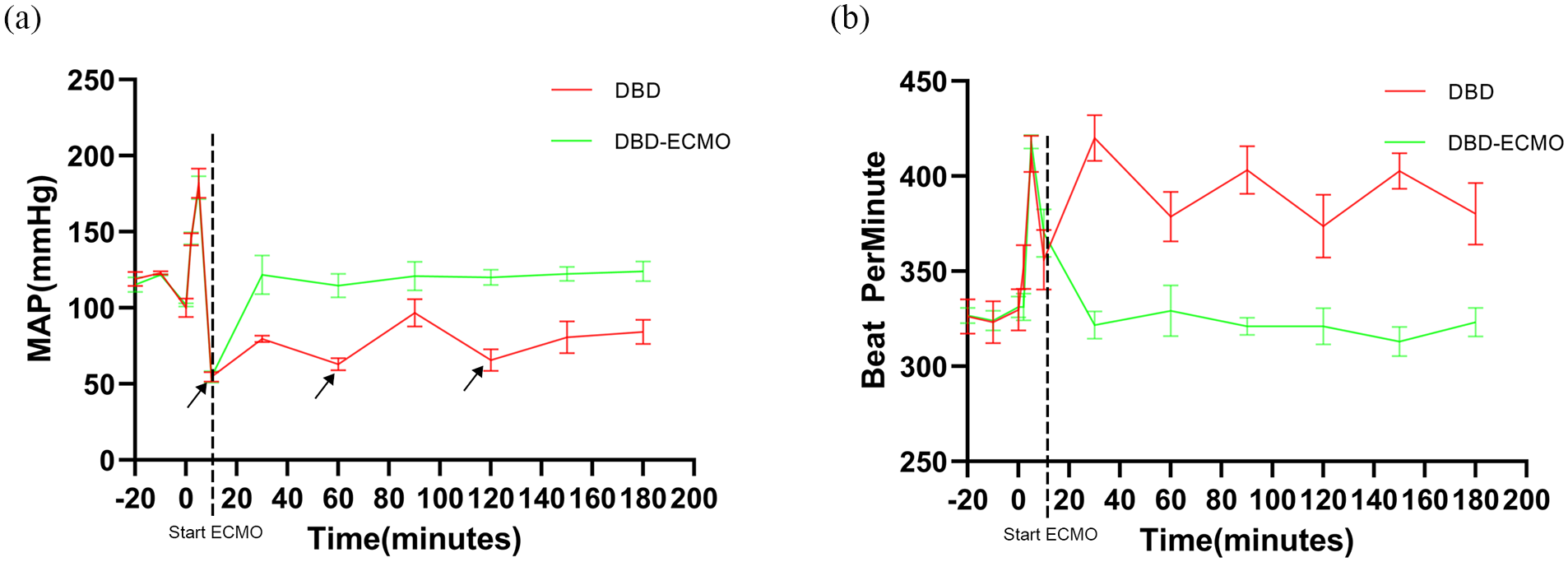
Mean arterial blood pressure and beat per minute in DBD-drug, DBD-ECMO groups during procedures. Time course of changes in mean arterial pressure (a) and beat per minute (b).
The physiological data.

Data are presented as mean ± standard deviation.
ECMO improves liver functions in DBD rats
Serum AST and ALT are liver function-related biochemical indices that increase during liver injury. We observed that the DBD-assisted ECMO group had lower serum ALT/AST levels compared with the DBD-assisted drug (Figure 3(a)). Furthermore, we evaluated the patterns of hemorrhage, tissue oedema, nuclear pyknosis, cell vacuolization, and cellular morphology using hematoxylin-eosin staining (HE staining) and combined them into a cumulative damage score according to standard pathologic criteria. Meanwhile, apoptotic death was assessed using TUNEL staining. Interestingly, the DBD-assisted ECMO group exhibited a lower HE damage score (Figure 3(b)) and TUNEL+ cells compared with the DBD-assisted drug (Figure 3(c)). These results indicate an absence of injury promotion and cytoarchitectural damage in the ECMO-assisted DBD group compared with the DBD-assisted drug. This suggests that ECMO support helps approach the normal state.
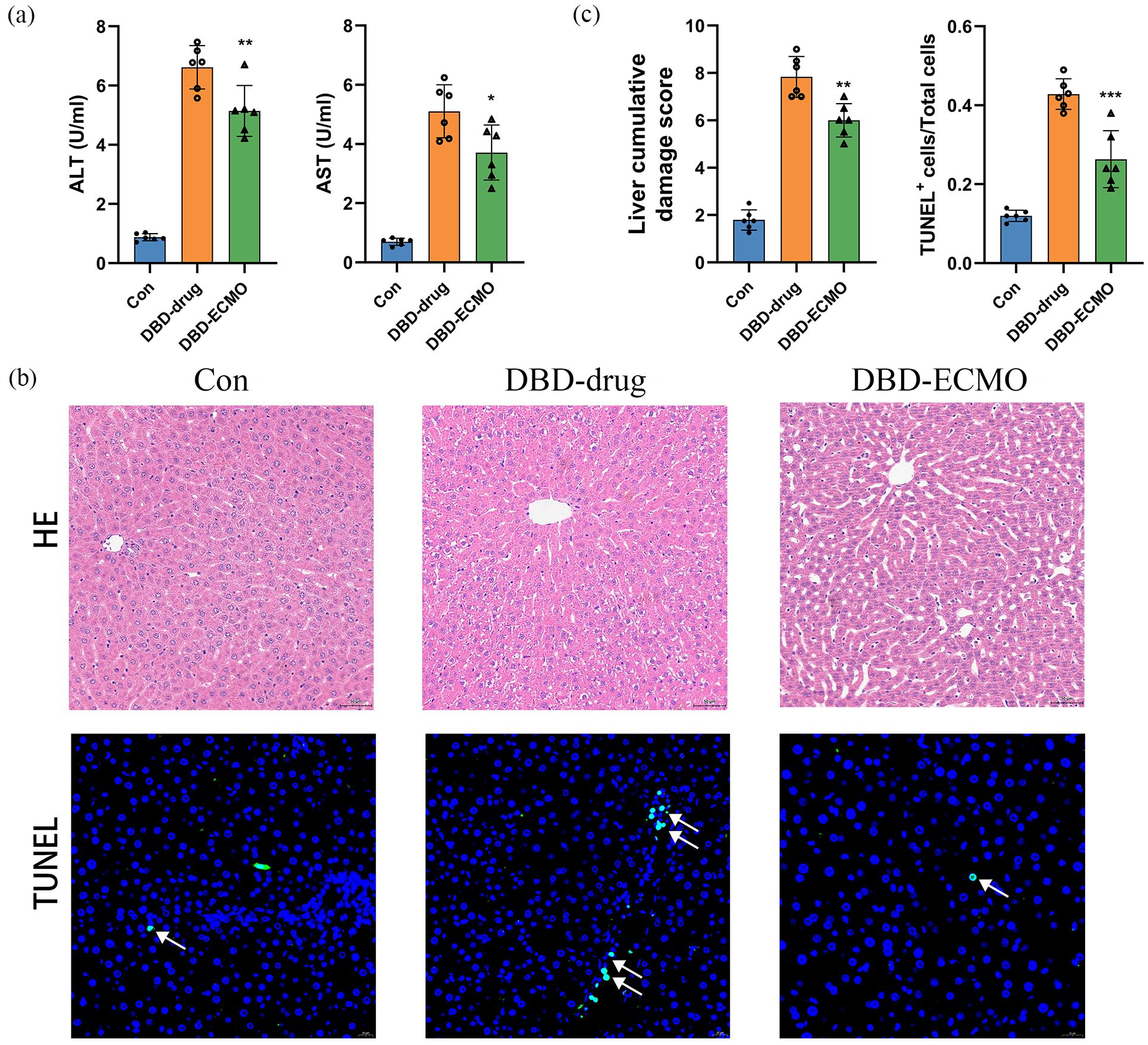
ECMO can reduce the liver injury of DBD: (a) ALT and AST levels (n = 6 per group). (b) Representative HE (original magnification, ×100; scale bar,100 µm) and TUNEL (original magnification, ×400; scale bar, 50 µm) staining. (c) Suzuki’s histological grading of the liver and quantification of TUNEL+ cells/Total cells (n = 6 per group). Data were shown as mean ± SEM. *p < 0.05. **p < 0.01. ***p < 0.001 by Student’s t-test.
ECMO reduces inflammatory response in DBD rats
Inflammation during brain death is an important cause of liver damage. We observed that ECMO reduced the levels of pro-inflammatory TNF-α, IL-1β, IL-6, and IL-8 in the serum of rats after brain death (Figure 4(a)). Danger-associated molecular patterns (DAMPs) regulate inflammation and give rise to numerous sterile inflammatory disorders. HMGB-1 expression in plasma is a DAMP indicator for tissue damage. Interestingly, ECMO reduced HMGB-1 levels in the serum after brain death. Additionally, we detected macrophages and neutrophils in the liver using IHC staining for CD68 and MPO, respectively. The DBD-assisted drug showed macrophage and neutrophil infiltration in the hepatic sinusoid (Figure 4(b)). In addition, MPO+ neutrophil infiltration and CD68+ macrophages were observed in the DBD but not in the DBD-assisted ECMO group (Figure 4(c) and (d)).
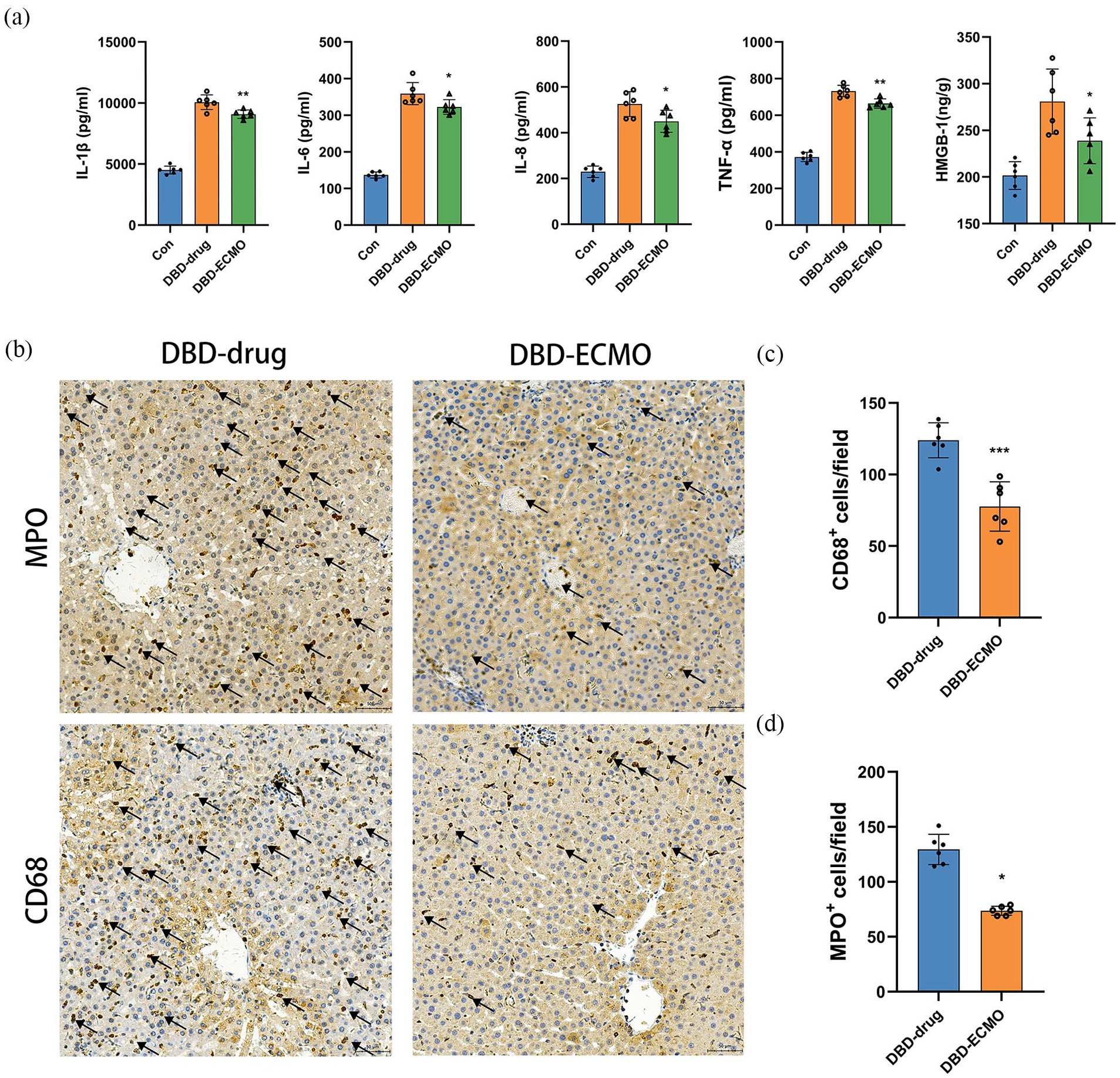
The role of ECMO might be correlated with downregulating inflammation in DBD-drug rats. (a) Elisa analysis of IL-1β, IL-6,IL-8,TNF-α serum concentrations in Con (n = 6), DBD-drug (n = 6), DBD-ECMO (n = 6) groups. (b) Activated microglia identified by MPO and CD68 IHC in the representative liver (scale bars represent 50 μm) in each group (n = 6 per group). Arrowheads: positive cell. (c) the MPO+ and CD68+ cell numbers/field in the liver tissues in each group (n = 6 per group). Data were shown as mean ± SEM. *p < 0.05. **p < 0.01. ***p < 0.001 by Student’s t-test.
ECMO reduces oxidative stress in DBD rats
Brain death decreases liver macro- and microcirculation, thereby increasing hepatic oxidative stress and causing liver cells to become ischemic-hypoxic. By measuring the levels of oxidative stress markers, we observed that brain death significantly increased MDA and H2O2 levels, while decreased SOD levels in the liver, which suggests increased
oxidative stress. In contrast, ECMO effectively alleviated oxidative stress (MDA, H2O2, SOD) (Figure 5(a)
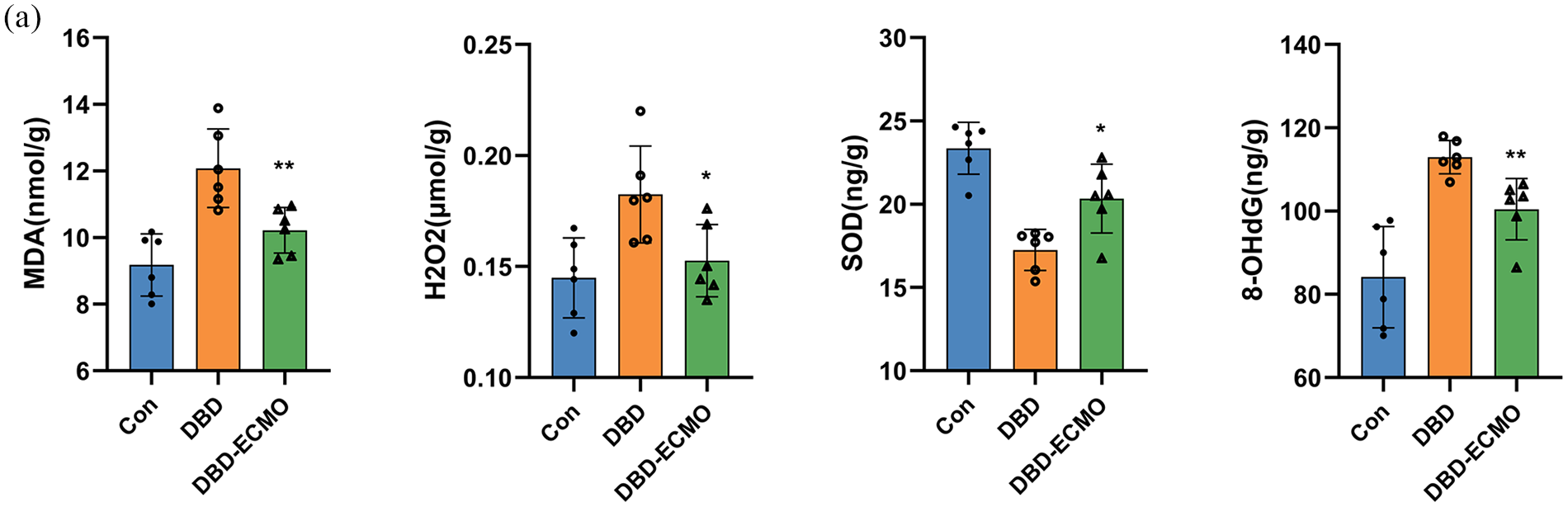
ECMO can reduce liver oxidative stress: (a) Elisa analysis of MDA, H2O2, SOD, 8-OHdG, liver concentrations in Con (n = 6), DBD-drug (n = 6), DBD-ECMO (n = 6) groups. Data were shown as mean ± SEM. *p < 0.05. **p < 0.01. ***p < 0.001 by Student’s t-test.
ECMO can improve liver function after transplantation
To assess whether the use of ECMO-preserved livers can lead to improved post-transplant outcomes, we established a rat orthotopic liver transplantation(OLT) model. Livers obtained using the two aforementioned methods were used for transplantation. Blood collected 72 h post-transplantation was analyzed. In comparison to the group where pharmacological blood pressure maintenance was employed after donation DBD, the group utilizing ECMO after DBD showed lower liver enzyme levels (Figure 6(a)). Additionally, we compared the 72-h postoperative survival rates, revealing that, except for one case, livers in the DBD-ECMO group could survive for 72 h with enhanced liver function, However, the overall survival rates the two groups were not significantly different (Figure 6(b)). Histopathological examination with HE staining of livers 72 h post-transplantation showed that ECMO-maintained donor livers after DBD exhibited reduced damage compared to those without ECMO support (Figure 6(c) and (d)).
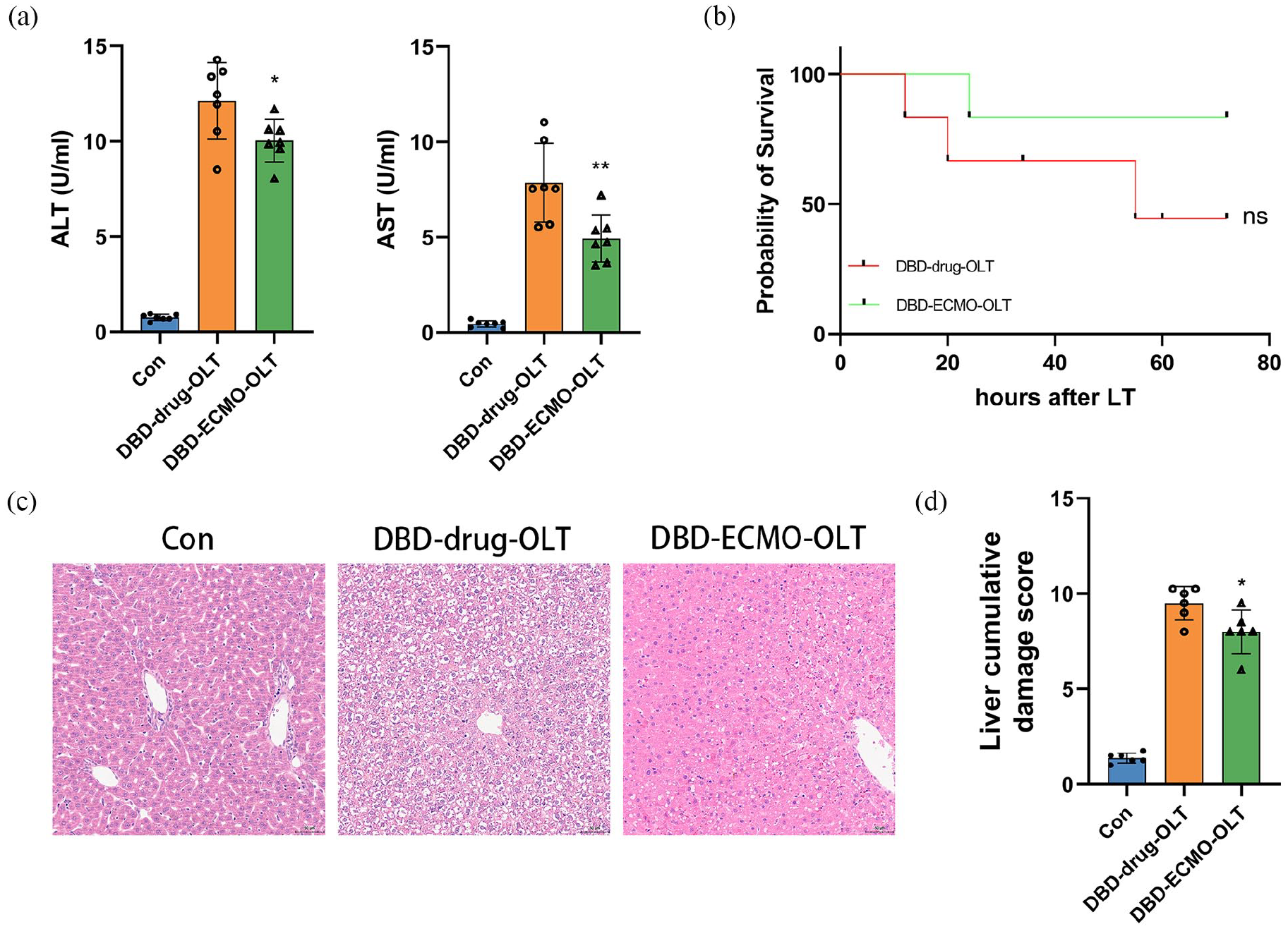
ECMO can improve liver function after transplantation. (a) ALT and AST levels (n = 6 per group). (B) Kaplan-Meier chart of rats after liver transplantation with and without ECMO.(C) Representative HE (original magnification, ×100; scale bar,100 µm). (d) Suzuki’s histological grading of the liver (n = 6 per group). Data were shown as mean ± SEM. *p < 0.05. **p < 0.01. ***p < 0.001 by Student’s t-test.
Discussion
Liver transplants obtained from DBD exhibit a higher incidence of grafting complications compared to those obtained from living donors. Additionally, within the 6–24 months post-transplantation period, organs sourced from DBD donors experience a significantly elevated rate of acute rejections in comparison to those from living donors. This discrepancy can be attributed to the impact of brain death, which induces the following physiological changes 12 : (1) Loss of autoregulation of blood pressure and sympathetic nerve tone. (2) Decrease in systemic vascular resistance. (3) Hemodynamic instability that disturbs blood supply, causes neutrophil and macrophage infiltration, releases pro-inflammatory factors, and increases oxidative stress in the liver. Furthermore, the hemodynamic instability associated with brain death necessitates the administration of vasoactive drugs to stabilize blood pressure and heart rate. Unfortunately, these drugs, while crucial for immediate stabilization, contribute to hepatocyte damage. Collectively, these multifaceted mechanisms adversely affect the graft quality from DBD donors, resulting in diminished graft survival rates.
ECMO, a life support system used to assist patients experiencing cardiopulmonary failure. 13 ECMO stabilizes hemodynamics without the use of vasoactive drugs. However, whether ECMO can improve liver functions in patients with DBD is not yet clear, which limits its use as a bridge to donation. Thus, we established stable and reliable DBD and DBD-assisted ECMO rat models for determining the effects of brain death and ECMO on liver functions, respectively. We observed that brain death causes hemodynamic instability and requires vasoactive drugs for maintaining blood pressure. However, ECMO stabilizes hemodynamics as well as protects liver functions by reducing systemic inflammation and oxidative stress in liver tissues. These results suggest that ECMO can be used for protecting the donor liver in DBD liver transplantation. We concurrently established a rat orthotopic liver transplantation model and conducted a comparative analysis between grafts from Donation after Brain Death (DBD) donors maintained solely with pharmacological agents and those supported by Extracorporeal Membrane Oxygenation (ECMO). Notably, the ECMO-supported DBD grafts demonstrated enhanced liver functionality; however, intriguingly, there was no statistically significant difference observed in the 72-h survival rates between the two groups. Several factors may contribute to this lack of observed disparity. Firstly, the sample size in each group was limited to only six liver transplants, which could potentially be considered suboptimal for robust statistical analysis. Secondly, our observation period was confined to the initial 72 h post-transplant, which may have influenced the ability to detect more nuanced differences in survival rates between the two groups. Thirdly, it is conceivable that ECMO maintenance primarily elevates the overall quality of the transplanted liver, thereby reducing post-transplant complications, without exerting a substantial influence on short-term survival rates. Addressing these considerations may require further corroboration through additional clinical data, emphasizing the need for a more comprehensive understanding of the complex interplay between ECMO support and post-transplant outcomes.
The use of Extracorporeal Membrane Oxygenation (ECMO) in cases of brain death, particularly when patients exhibit unstable hemodynamics, are non-responsive to vasopressors, or suffer from respiratory failure, has been clinically explored. However, the optimal duration for ECMO support prior to organ retrieval remains unclear. Moreover, the literature offers limited guidance on graft selection criteria, relying predominantly on transaminase levels and liver biopsy findings, underscoring the need for established validation protocols. The decision to initiate ECMO, either in anticipation of or following death, introduces ethical dilemmas due to potential moral implications.14–16 Furthermore, conducting the apnea test in ECMO-supported patients demands specific alterations to the standard protocol. 17 Although the availability of organs for transplantation is a byproduct rather than the primary aim, some experts suggest ECMO should be reserved as an emergency measure during the diagnosis of brain death and not as a method for organ preservation. 18 The technique for organ retrieval from donors maintained on ECMO closely mirrors that used for traditional donors, but certain considerations, such as lowering perfusion temperatures for cold flushing or adopting machine perfusion post-retrieval, have been examined in the context of Donation after Cardiac Death (DCD) donors, potentially enhancing graft preservation and evaluation.19–21
Certain studies indicated no difference between clinical DBD and standard DBD after ECMO. Despite a complicated clinical course, organs procured from DBD donors on ECMO seem to be similar to those from standard donors in terms of primary non-function (PNF), postoperative complications, and short-term graft survival. However, since only a few studies have reported on biliary complications, definitive conclusions cannot be drawn, and the use of Normothermic regional perfusion (NRP) has proven effective in reducing such complications in DCD. 22
This study has several limitations. The use of exclusively male animals means that the results and implications for females remain unknown. Additionally, ECMO support was limited to a 3-h duration to mitigate pump-related blood damage. Another limitation is the use of intermittent vasopressor dosing in the Drug arm to mimic the hemodynamic instability often observed in brain death, resulting in significant blood pressure fluctuations. While continuous infusion of vasopressors is standard in clinical practice, this approach was intended to replicate the instability within the constraints of our model. Future studies should investigate the safety and underlying mechanisms of ECMO more comprehensively and explore continuous vasopressor infusion to compare the effects and further validate the model.
It is crucial to emphasize that the use of DBD + ECMO should be considered judiciously and reserved for cases of refractory hemodynamic instability. ECMO is an extremely resource-intensive and costly intervention. If vasoactive infusions can stabilize the DBD patient, this approach would be preferable due to its lower cost and resource requirements. Moreover, peripheral ECMO may increase afterload on the heart, potentially causing cardiac damage and pulmonary edema. These adverse effects could render thoracic organs unsuitable for transplantation. Therefore, clinicians must carefully evaluate the necessity of ECMO in each case, balancing the potential benefits against the risks and resource implications. This consideration is essential to optimize patient outcomes and ensure the effective use of medical resources.
Conclusion
This study successfully established a DBD-assisted ECMO rat model for liver transplantation. It identified that ECMO reduces liver injury in brain death rats by stabilizing hemodynamics and downregulating inflammation and oxidative stress. Thus, this study provides a potential therapeutic approach to use ECMO for improving liver functions in DBD rats.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Postdoctral Fund (No.2020M683610); the Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (No. CY2021-MS-B05); the Cuiying Students Research Cultivation Program of Lanzhou University Second Hospital (No. CYXZ2021-09); Lanzhou Science and Technology Program Project (NO.2023-4-38).