
Abstract
Objective:
Hemodialysis can significantly prolong the survival of uremia patients, but uremia and long-term hemodialysis can also cause complications. This study aimed to compare the clinical efficacy between the menostat mesylate and sodium citrate as anticoagulants in patients receiving CRRT.
Methods:
The clinical data of 80 patients with uremic cerebral hemorrhage in our hospital from January 2020 to October 2022 were collected and randomly divided into observation (nelostat anticoagulation, n = 40) and control (citrate and sodium anticoagulation, n = 40) groups. Physiological parameters, CRRT filter life, coagulation function index, activated whole blood coagulation time (ACT), anticoagulation efficiency rate, and incidence of adverse reactions were compared between the two groups.
Results:
The physiological index, coagulation function index, ACT value, and anticoagulation efficiency were higher in the observation group than in the control group (p < 0.05). The observation group also demonstrated a longer CRRT filter life and lower incidence of adverse reactions than those in the control group (both p < 0.5).
Conclusion:
Naphlimostat mesylate demonstrated a good anticoagulant effect and was safe for use in CRRT.
Introduction
Hemodialysis can significantly prolong the survival of patients with uremia; however, uremia itself and long-term hemodialysis can also cause complications, including cerebral hemorrhage, a serious complication that occurs in 1.6%–2.3% of cases. 1 Continuous renal replacement therapy (CRRT) is the first choice of treatment for intermittent hemodialysis (IHD) because it removes more solutes and does not aggravate hemodynamic instability. However, a main drawback of CRRT is the need for anticoagulants to prevent blood clotting. 2 Ideal anticoagulants should exhibit optimal antithrombotic activity, minimal bleeding complications, and negligible systemic effects. CRRT usually uses unfractionated heparin as an anticoagulant, which has the advantages of low price, simple management, and easy monitoring; however, it is unsuitable for patients with bleeding diseases. 3 Owing to the risks of side effects, sodium citrate is gaining popularity as a CRRT anticoagulant in patients at high risk for bleeding.
The effectiveness of sodium lime citrate as an anticoagulant in CRRT is similar to that of heparin, and it reduces the risk of bleeding. The disadvantage of using citrate is the need for frequent monitoring of electrolyte and ionized calcium levels and acid-base status, as citrate can cause hypernatremia, metabolic alkalosis, and systemic ionizing hypocalcemia. 4 As a possible alternative, naphlimostat mesylate is a synthetic serine protease inhibitor with a biological half-life of approximately 8 min. Given that both antithrombotic activity and short half-life are essential for anticoagulation in renal replacement therapy, naphlimostat mesylate has been used as an anticoagulant during hemodialysis in patients with bleeding conditions or another coagulopathy.5,6 Although the use of naphrostat mesylate is increasing, few studies have reported its safety and efficacy, and domestic studies comparing it with sodium citrate are rare. Therefore, this study analyzed the clinical effects of nalilimostat compared with sodium citrate as anticoagulants in CRRT in patients with uremic cerebral hemorrhage.
Materials and methods
General information
The clinical data of 80 patients with uremic cerebral hemorrhage treated at our hospital between January 2020 and October 2022 were collected and randomly divided into observation (menmonostat mesylate, n = 40) and control (sodium citrate, n = 40) anticoagulation groups. Inclusion criteria: (1) All patients meet the clinical diagnostic criteria of uremia and cerebral hemorrhage7,8; (2) the patient had no other co-affected tumors and other immune system and blood system diseases; (3) no drugs prone to thrombolytic bleeding; (4) no allergy to the drugs involved in the institute; (5) the patient without hypoxemia, hyperlactatemia, and hypernatremia; and (6) regular hemodialysis treatment three times a week. Exclusion criteria: (1) patients with other tumors, immune, or blood diseases; (2) incomplete clinical data; (3) allergic reaction to the drug under study; and (4) patients with severe liver insufficiency.
Physiological parameters, CRRT filter lifetime, coagulation function index, anticoagulation response rate, and the incidence of adverse effects were compared between the two groups. General clinical data were collected for all included patients. These clinical data did not differ significantly between the groups (p > 0.5; Table 1). All patients provided signed informed consent.
Comparison of the general clinical data between the two groups.
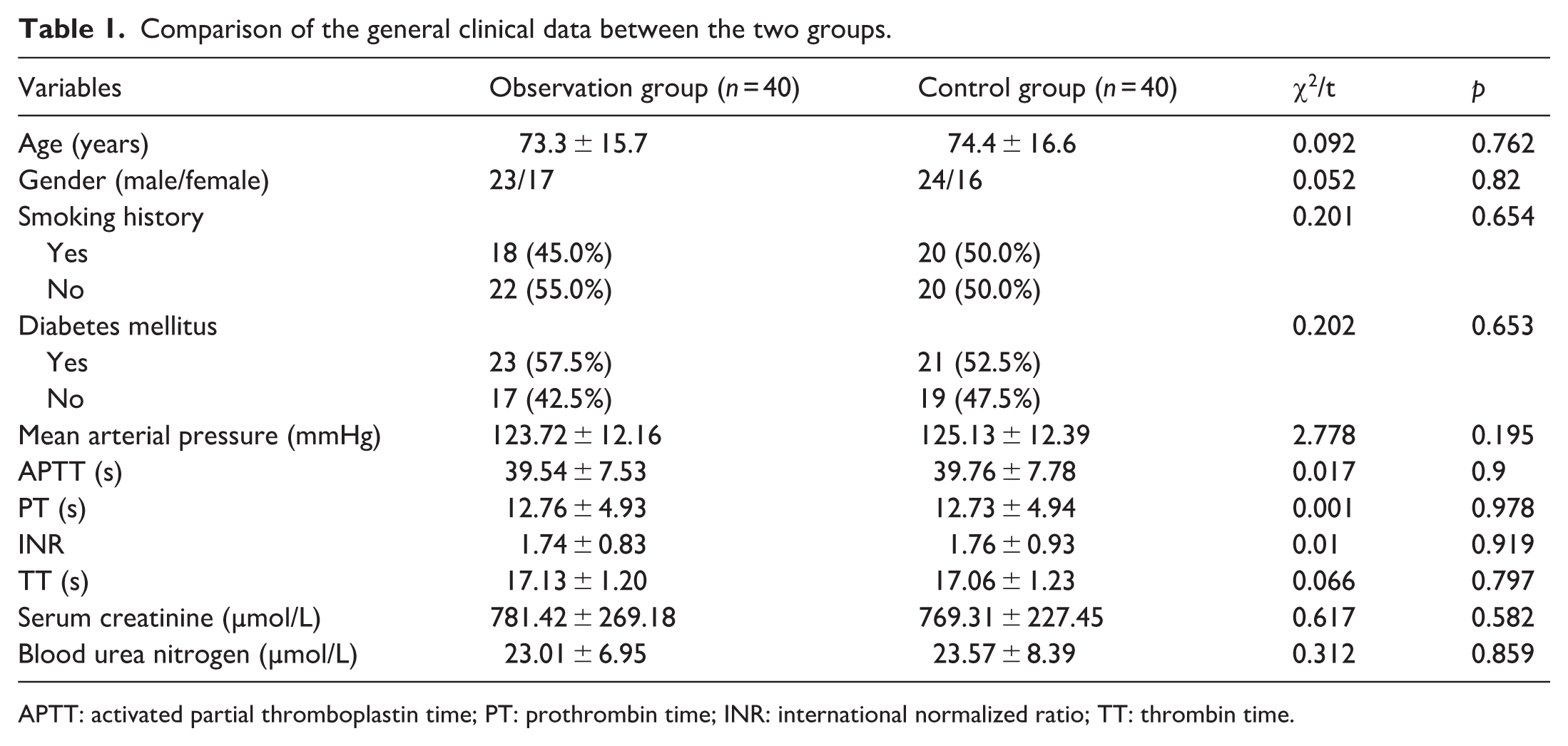
APTT: activated partial thromboplastin time; PT: prothrombin time; INR: international normalized ratio; TT: thrombin time.
Anticoagulation methods
The observation group was administered 500 mL of 0.9% sodium chloride injection with 20 mg naphthylostat in 5 ml of 5% dextrose (10 mg/bottle, H20203508, Jiangsu Durui Pharmaceutical Co., Ltd.). After starting the treatment, Nlimostat mesylate (200 mg, 50 mg/vial, H20203509, Jiangsu Durui Pharmaceutical Co., Ltd.) was dissolved in 50 ml of 5% glucose and injected via continuous micropump administration at 25 mg/h through a filter. During the dialysis, blood was sampled from the arterial end line every 4 h to measure the activated clotting time (ACT). The drug administration rate was dynamically adjusted according to ACT value: for values >120%, the pump speed was decreased to 12.5 mg/h, while for values >150%, dialysis was suspended for 2 h, and the pump speed was adjusted according to the latest measurements. The instrument used was an Aquarius continuous blood purification device (Baxter, USA).9,10 In the control group, the line was flushed with sodium citrate and connected to the motor, and venous ends with vascular access were used to add 10% calcium gluconate (pump rate (ml/h) = 7.7% × blood flow rate (ml/h)). The arterial end was used to input 4% sodium citrate anticoagulant (pump rate = 1.6 × blood flow rate). The sodium citrate concentration and blood flow rate were adjusted according to the timing of blood gas analysis results to maintain the filter Ca+ concentrations at 0.25–0.40 mmol/L and systemic blood Ca2+ levels until the end of treatment. Coagulation of the dialyzer and circulating line was checked, and the time recorded combined with ACT, with adjustments to the dose of anticoagulant drugs made as required.11,12 The ACT was divided into three points (A, B, and C) for blood collection: from the bloodline (arterial end) before the pump (point A), between the pump and dialyzer (point B), and after the dialyzer (venous end; point C). 13
Evaluation indices
Physiological parameters, CRRT filter life, coagulation function index, whole blood activated clotting time (ACT), anticoagulation efficacy rate, and incidence of adverse reactions were evaluated in both groups. The physiological indicators included (heart rate, respiratory rate, systolic blood pressure, and fingertip oxygen saturation). The normal heart rate, respiratory rate, upper limit of systolic blood pressure, and normal fingertip oxygen saturation values were defined as 60–100 beats/min, 16–20 breaths/min, 120 mmHg, and 90%–100%, respectively. 14 The coagulation function indicators included prothrombin time (PT), international normalized ratio (INR), activated partial thromboplastin time (APTT), and thrombin time (TT). 15 The coagulation in the dialyzer was categorized as grades 0–III, with lower grades indicating better anticoagulant effects to assess anticoagulant efficiency. ACT values were collected at points A, B, and C and 15 min after dialysis.
Statistical analysis
Continuous variables are expressed as means ± standard deviation. The two groups were compared using the independent t-test. Count data are expressed as numbers (percentages) and compared using the χ2 test, with statistical significance set at p < 0.05.
Results
Physiological indices
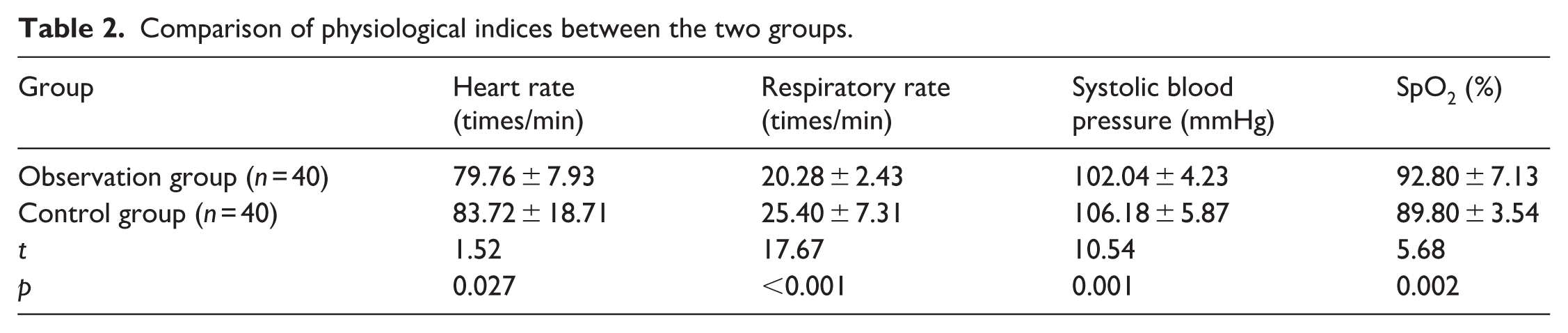
The physiological indices of the two groups differed significantly (p < 0.5), with the menostat mesylate group showing better values compared with the sodium citrate group (Table 2).
Comparison of physiological indices between the two groups.
Anticoagulation response rates
The efficacy rate of anticoagulants with pranostat mesylate was significantly higher than that with sodium citrate (92.5% vs. 75.0%, p = 0.034), suggesting better anticoagulation with nlimostat mesylate (Table 3).
Comparison of anticoagulation response rate between the two groups.

Coagulation indicators
The time of APTT and INR value in the observation groups were increased than those in the control group, but the difference was not significant. The time of PT and TT in the observation group were significantly higher than those in the control group (p < 0.5; Table 4).
Comparison of coagulation indicators between the two groups.
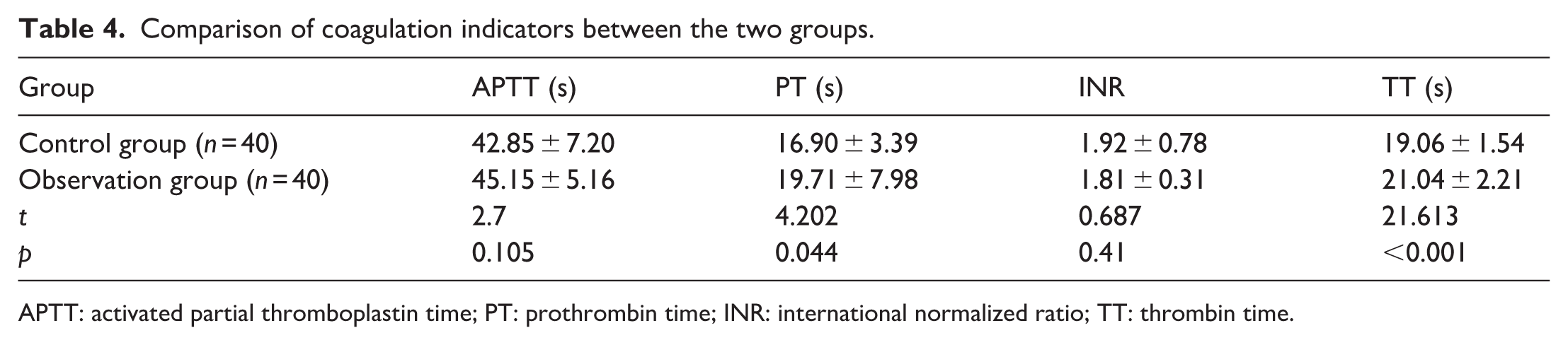
APTT: activated partial thromboplastin time; PT: prothrombin time; INR: international normalized ratio; TT: thrombin time.
ACT indexes and CRRT filter life
After blood collection at A, B, and C, the ACT values in the observation group were higher than those in the control group (p < 0.5), indicating that the effect of nlostat mesylate on ACT was small. The service life of CRRT filters in the observation group was also longer than that in the control group (p < 0.5; Table 5).
ACT index and CRRT filter life.

Adverse reactions
The incidence rate of adverse reactions in the observation group was 7.5%, including three cases (one with device problems, one with abnormal acidophil count, and one with decreased platelet count). In contrast, the rate of adverse reactions in the control group was 20%, including eight cases (two cases of decreased platelet count, three cases of ventricular contraction, and one case of abnormal acidophil count). The incidence rates differed significantly between the groups (p < 0.5), with namodiostat mesylate showing a better safety profile than sodium citrate.
Discussion
Clinically, >80% of patients with uremia are prone to cerebral hemorrhage when blood pressure increases, with a high mortality rate. 16 Therefore, reducing the increase in uremic mortality due to ICH is crucial. Currently, hemodialysis is the primary clinical treatment for uremia. Commonly used anticoagulants include heparin, low-molecular-weight heparin, agatroban, citrate, and nlostat mesylate. 17 CRRT is the first choice of treatment for IHD because it removes more solutes and does not aggravate hemodynamic instability. One of the main drawbacks of CRRT is the need for anticoagulants to prevent blood clotting. Therefore, antithrombotic activity and a short half-life are essential for anticoagulants in renal replacement therapy. 18 Patients undergoing kidney dialysis with active bleeding disease, obvious bleeding tendencies, or abnormal coagulation may receive adatroban, sodium citrate, and naphrostat mesylate according to patient status. Moreover, some patients may temporarily receive no anticoagulant treatment.19,20 Currently, sodium citrate is the first-choice anticoagulant for CRRT in China. However, the application of sodium citrate requires monitoring of blood calcium levels and activated partial thromboplastin time (APTT), and sodium citrate should not be administered to renal patients with severe liver dysfunction, hypoxemia, metabolic acidosis, and hypernatremia. 21 Clinical studies confirmed that namotl mesylate can be used as an anticoagulant during hemodialysis in patients with bleeding or coagulopathy. In earlier studies, to avoid heparin use, researchers administered namotat mesylate to 33 patients at high risk for bleeding undergoing hemodialysis. Drug concentration and anticoagulant activity were stable during hemodialysis, and the anticoagulant activity decreased immediately after hemodialysis. 22 The present study compared napholostat and sodium citrate. The physiological indices, anticoagulation efficacy rate (92.5%), coagulation function indices, and ACT values were all higher in the group administered napholostat than those in the control group administered sodium citrate (p < 0.5). Thus, napholostat mesylate had a good anticoagulant effect. Moreover, the service life of the CT filter for napholostat mesylate was longer than that of sodium citrate, consistent with the reports by Beicun et al. 23 that pranostat mesylate had higher hemofilter longevity and fewer hemorrhagic complications in patients at high risk for bleeding. The incidence of adverse reactions to mentolostat mesylate anticoagulant (7.5%) was lower than that of adverse reactions to sodium citrate (20%), indicating that mentolostat mesylate anticoagulant is safe.
Conclusions
Usage of naphlimostat mesylate in CRRT treatment demonstrated significant anticoagulant efficacy and can improve the physiological status of patients, anticoagulation efficiency, and coagulation function index with high safety.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.