
Abstract
Introduction:
Management of severe circulatory collapse in the setting of amlodipine toxicity can be challenging. High doses of vasopressors and conventional therapies fail to improve hemodynamics, resulting in the use of veno-arterial extracorporeal membrane oxygenation (VA-ECMO) to treat severe cardiogenic shock and peripheral vasodilatation. Therapeutic plasma exchange (TPE), which helps remove plasma protein-bound toxins and significantly reduces mortality, may be a useful adjunct to invasive hemodynamic support in severe cases of amlodipine poisoning.
Case summary:
A 32-year-old female with a history of intentional consumption of ninety 5-mg amlodipine tablets (totaling 450 mg) was admitted to our intensive care unit (ICU) after 3 h. Her amlodipine serum concentration was 147 ng/mL. She presented with cardiogenic shock and fatal vasoplegia and received VA-ECMO and TPE. The patient was weaned off ECMO after 4 days and discharged home on Day 10 of hospitalization.
Conclusion:
Amlodipine toxicity can result in severe cardiac failure with circulatory collapse. We describe the case of a patient with cardiovascular collapse who successfully bridged to recovery from refractory shock secondary to severe amlodipine toxicity as a result of ECMO and TPE treatment.
Introduction
Calcium channel blockers (CCBs) are widely prescribed cardiovascular drugs that are used for hypertension, angina, and heart failure. According to the National Poison Data System (NPDS), CCB poisoning in adults was one of the most common causes of toxicity-related deaths among cardiovascular drug overdoses in 2016. 1 Amlodipine is a widespread prescribed drug belonging to the group of CCBs, with a duration of action of approximately 30–58 h. This mechanism involves blocking voltage-gated calcium channels, which results in decreased cardiac contractility and peripheral vasodilatation. 2 Refractory poisoning-induced shock and pulmonary edema after the ingestion of amlodipine are very challenging to treat.
According to the Expert Consensus Recommendations for the Management of Calcium Channel Blocker Poisoning in Adults, first-line therapies for CCB poisoning in symptomatic CCB-poisoned patients include intravenous calcium, high-dose insulin therapy, and norepinephrine and/or epinephrine in the presence of shock. In addition to these first-line treatments, the workgroup suggests extracorporeal membrane oxygenation (ECMO) as a rescue treatment for the treatment of CCB-poisoned patients in refractory shock. 3 However, routine methods of dialysis cannot rapidly and effectively remove CCBs because of their protein-bound nature.4,5 Therapeutic plasma exchange (TPE) may provide a valid alternative rescue option following massive ingestion of toxic substances, especially those with high protein binding. 6 We present a rare case of severe amlodipine toxicity with refractory cardiovascular collapse and successful treatment following extracorporeal membrane oxygenation (ECMO) and therapeutic plasma exchange (TPE). The aim of this study was to describe the clinical properties of amlodipine toxicity and provide clinicians with valuable insight for successful treatment strategies.
Case report
A 32-year-old female presented after ingesting approximately 450 mg of amlodipine about 3 h earlier. She was hemodynamically stable on arrival at the local hospital (30–45 min later) and received a gastric lavage with activated charcoal and adequate intravenous fluids. The patient’s family reported vomiting and progressive lethargy before arriving at our hospital for further management. Upon admission to the emergency department (ED) of our hospital, the patient developed sudden shock with an abrupt drop in mean arterial pressure from 100 to 60 mmHg and concomitant drowsiness and tachypnea. Fluid resuscitation with calcium and insulin infusion commenced because of hypotension; subsequently, she was intubated and mechanically ventilated. Dopamine was commenced and titrated to address her hypotension further. On arrival at the intensive care unit (ICU), her blood pressure was 90/40 mmHg, with a heart rate of 105 bpm and 80% oxygen saturation on a 100% inspired oxygen concentration on the ventilator. Initial arterial blood gas analysis (ABG) revealed a pH of 7.23, PCO2 of 64 mmHg, PO2 of 44 mmHg, HCO−3 of 26.8 mmol/L, BE of −1.5 mmol/L, Glu of 22 mmol/L, and Lac of 10.5 mmol/L. Transthoracic echo (TTE) demonstrated acute systolic heart failure with an ejection fraction of 50%, and electrocardiography revealed sinus tachycardia. When the arterial line was placed, the results of pulse in continuous cardiac output (PiCCO) revealed a CI of 4.19 L/min/m2, a GEDI of 525 mL/m2, an SVRI of 1275 dyn s cm−5 m2, an ELWI of 16 mL/kg, and a GEF of 25%. Invasive hemodynamic monitoring indicates high cardiac output with low vascular resistance, increased pulmonary vascular permeability and pulmonary edema. Mean arterial blood pressures between 45 and 60 mmHg persisted despite high doses of epinephrine, norepinephrine, and dopamine. The patient subsequently developed acute kidney injury (AKI) requiring early renal replacement therapy without any hemodynamic improvement.
The patient’s hemodynamics continued to deteriorate. TTE assessment revealed severe left ventricular systolic dysfunction with a 30% ejection fraction. Therefore, veno-arterial extracorporeal membrane oxygenation (VA-ECMO) was finally started after 10 h of aggressive medical treatment (Figure 1). A 23-Fr drainage cannula was inserted into the left femoral vein, and a 19-Fr return cannula was inserted into the right femoral artery with an antegrade perfusion catheter (flow of 3.5 L/min; gas flow of 6). Over the subsequent 24 h, the epinephrine and norepinephrine infusions were gradually tapered, and the dopamine infusion was discontinued. Therapeutic plasma exchange (TPE) was added in series with VA-ECMO using continuous renal replacement therapy (CRRT) to facilitate amlodipine clearance. The blood flow rate was 200 mL/min, and the dialysate flow rate was 2000 mL/h. The blood levels of amlodipine, creatinine, and serum lactate decreased. The total plasma volume (in liters) was calculated using the following formula: 0.065 × weight (kg) × (1-hematocrit). The replacement fluid was fresh frozen plasma. No changes were made to systemic heparin anticoagulation. The patient subsequently developed ventilator-associated pneumonia (VAP), and the sputum culture revealed carbapenem-resistant Acinetobacter baumannii (CRBA). According to the results of the drug sensitivity test, cefoperazone sodium/sulbactam sodium combined with tigecycline was administered to treat the infection. VA-ECMO was gradually weaned starting on Day 4, after discontinuation of the vasoactive agent, lipid emulsion, and insulin and calcium infusions 24 h earlier. The patient received a total of seven TPE cycles followed by an additional 24 h of CRRT for fluid removal. Finally, the patient was transferred to the ward and subsequently discharged home on Day 10. Table 1 shows the relevant laboratory test results. Figure 2 shows the patient’s vasoactive agent dose and blood pressure related to therapeutic interventions.
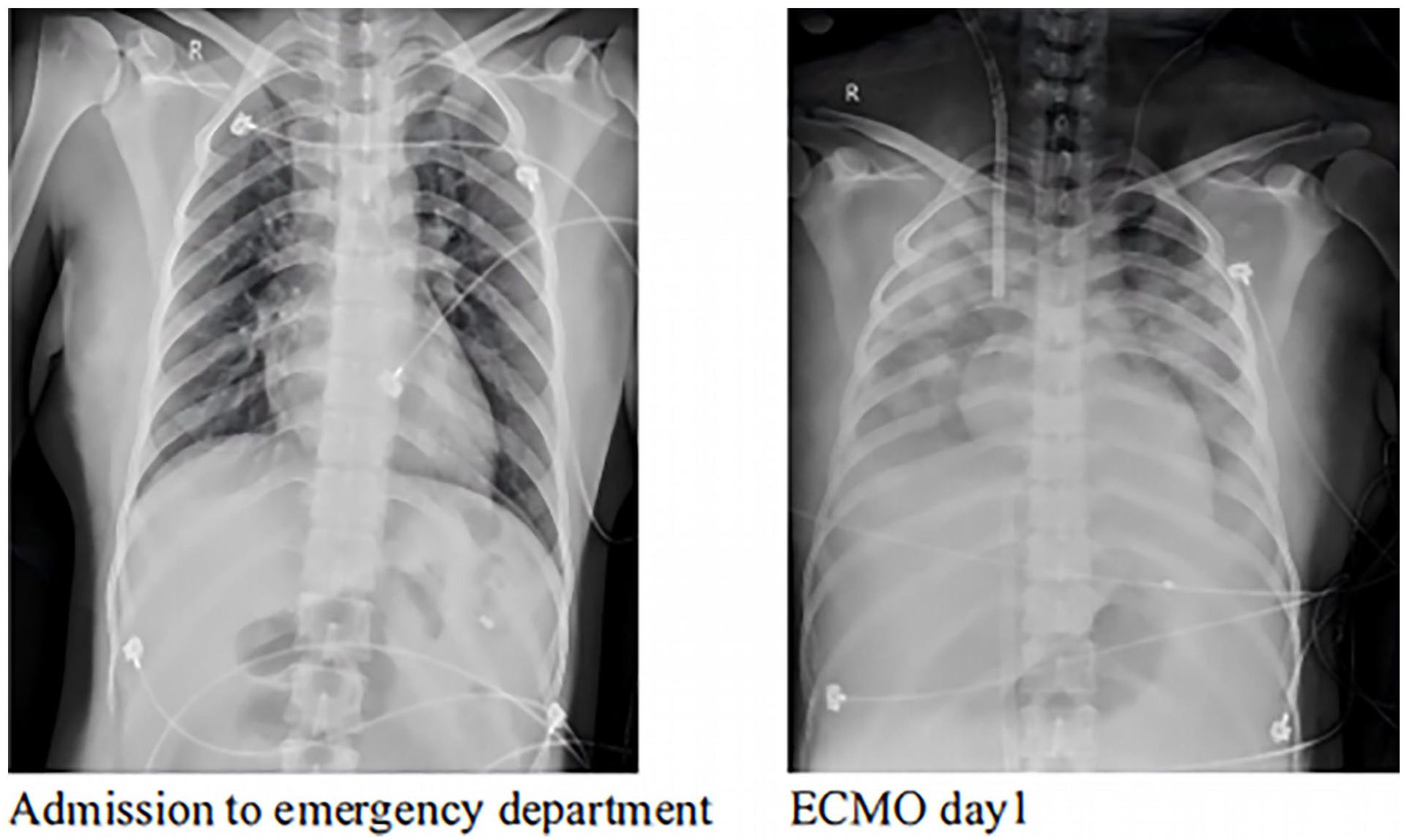
Chest X-ray evolution of the patient.
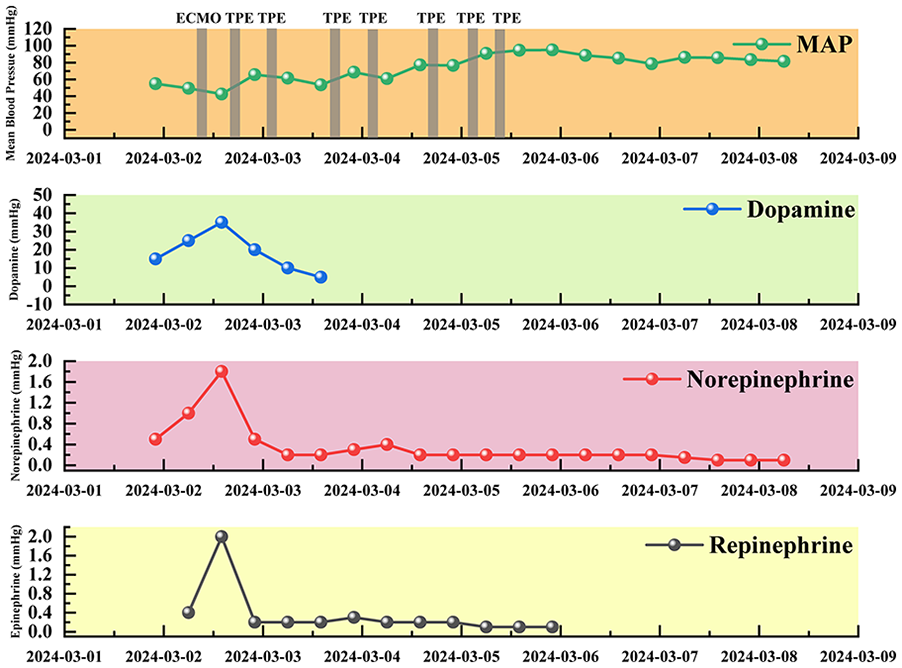
Timeline from admission through ECMO decannulation and inotropic support with dopamine (blue), norepinephrine (red) and epinephrine (black) with interventions (gray).
List of laboratory values.

ECMO: extracorporeal membrane oxygenation; CRP: C-reactive protein; HGB: hemoglobin; PLT: platelets; PCT: procalcitonin; Tbil: total bilirubin; ALT: alanine transaminase; AST: aspartate aminotransferase; BUN: blood urea nitrogen; PT: prothrombin time; APTT: activated partial thromboplastin time; INR: international normalized ratio.
Discussion
Calcium channel blocker (CCB) poisoning is a leading cause of prescribed cardiovascular medication intoxication, resulting in almost 50% mortality. 7 Amlodipine is a long-acting dihydropyridine derivative that acts on L-type calcium channels in the heart and vessels, resulting in vasodilation and a reduction in inotropism and chronotropism. 8 On initial evaluation, our patient had many of the hallmark signs and symptoms of amlodipine intoxication, including vomiting, lethargy, hypotension, myocardial depression, hypocalcemia, and lactic acidosis. These subtle toxic signs are suggestive of amlodipine intoxication. 9 Vogt et al. reported that the lethal dose of amlodipine was 70 mg, which is equivalent to a serum concentration of 185 µg/L. 10 In our patient, the serum drug concentration (147 ng/mL) was extremely high compared with that in previous reports. Early invasive hemodynamic monitoring revealed normal cardiac output and a significant reduction in peripheral vascular resistance, whereas X-ray suggested pulmonary edema. Although the intake level of amlodipine in this case was far greater than the lethal dose, the early cause of shock was severe peripheral vasodilation rather than a decrease in cardiac output. The patient’s left ventricular systolic function and cardiac output remained relatively stable. The PiCCO findings revealed a marked elevation in the extravascular lung water index, heightened pulmonary vascular permeability, a reduced systemic vascular resistance index and normal cardiac output, indicating that the patient was experiencing noncardiogenic pulmonary edema. However, the patient quickly developed cardiogenic shock, which was the main cause of ECMO initiation. Therefore, the patient may have experienced both cardiogenic and distributive shock. In cases similar to the one reported here, where refractory cardiogenic shock and peripheral vasodilatation occur, VA-ECMO can be used to support the cardiopulmonary system during the critical phase of acute refractory shock due to severe amlodipine poisoning.
However, the optimal timing for ECMO initiation remains inadequately defined in poisoned patients. The time of cardiogenic shock onset after ingestion largely ranges among patients, depending to a large extent on its serum concentration. In this case, the time from admission to ECMO implantation was 10 h, and the amlodipine serum concentration was 147 ng/mL. Although multiple in-hospital interventions were used in combination, the patient still developed refractory shock. The understanding of ECMO initiation in such circumstances remains limited. Nevertheless, in our patient, the rapid development of profound hemodynamic instability or cardiogenic shock and elevated lactate levels should be considered strong indications for emergent ECMO. VA-ECMO can also restore tissue and organ perfusion in the case of heart failure and can be used for hemodynamic stabilization in this patient population. 11 Similar to septic shock, drug-induced shock can result in simultaneous cardiogenic shock and distributive shock. Two scientific statements from the American Heart Association recommend the consideration of ECMO in patients with clinical hypoperfusion or hemodynamic deterioration while on inotropes according to the specific hemodynamic conditions.12,13 In addition, Upchurch et al. suggested that ECMO may provide hemodynamic and respiratory support to poisoned patients with refractory shock, cardiac arrest, or respiratory failure. 14 For the patient described in our case report, it could be argued that ECMO was at the center of successful treatment.
According to the American Society of Apheresis guidelines, TPE is the second-line therapy for acute drug overdose and is considered an appropriate treatment strategy. 15 Only a few case reports on TPE for massive amlodipine poisoning have been reported. Our patient’s amlodipine concentration was 147 ng/mL within 12 h after ingestion, which is far greater than the therapeutic peak concentration of 8.1–10.3 ng/mL. 16 Owing to the favorable binding of amlodipine to albumin and the absence of specific therapeutic alternatives, TPE is considered a therapeutic rescue option, as noted in our case. TPE is viewed as a feasible alternative method to remove large molecules located intravascularly and small molecules with high protein-binding ability. 17 In addition, drugs that exhibit high lipophilicity and are distributed into tissues may display a postdistribution rebound effect after TPE initiation, which rapidly reequilibrates between compartments and returns to preexchange plasma concentrations of the toxic substance. 18 Our patient’s amlodipine concentration decreased to 6 ng/mL from 147 ng/mL after multiple cycles of plasmapheresis. According to our experience and actual knowledge, the utilization of TPE provides a useful adjunct for the management of severe amlodipine toxicity.
Consequently, this combination results in hemodynamic improvement in patients with severe amlodipine poisoning and reductions in the serum concentration.
Conclusions
Amlodipine toxicity can result in cardiogenic shock and peripheral vasodilatation without response to conventional medical management. There are no specific antidotes for reversing the effects of this poisoning, and the treatment strategy is supportive. The described case demonstrates that patients with severe amlodipine intoxication benefit from advanced cardiac life support. We also used TPE for this patient, with encouraging results, suggesting that it may be a useful adjunct to ECMO. This combination should be further verified.
Supplemental Material
sj-pdf-1-jao-10.1177_03913988251321620 – Supplemental material for Veno-arterial ECMO support for severe amlodipine toxicity combined with cardiogenic shock: A case report
Supplemental material, sj-pdf-1-jao-10.1177_03913988251321620 for Veno-arterial ECMO support for severe amlodipine toxicity combined with cardiogenic shock: A case report by Yi Sun, Tingting Wang, Jiading Xia, Liwei Hua, Shuchen Cao and Kun Zhang in The International Journal of Artificial Organs
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The study was approved by the Ethics Committee of the Affiliated Hospital of Chengde Medical University and was performed in accordance with the tenets of the Declaration of Helsinki.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.