
Abstract
Introduction:
Renal replacement therapy efficiently eliminates cefepime. A published in vitro study concluded to minimal adsorption of cefepime in a polysulfone derived filter. We aimed at assessing cefepime adsorption in filters used in critically ill patients.
Methods:
Two filters were used, ST™150 and AV™1000. Adsorption was assessed in two modes, including diafiltration and filtration set to flow rates of from 2.5 to 1 L/h, respectively. Routes of elimination were assessed using NeckEpur® method for 6-h session duration.
Results:
The mean initial concentration in the 5-L central compartment (CC) in the 10 sessions was 47.7 ± 2.9 mg/L. Using the diafiltration mode, the mean adsorption rates in the ST™150 and AV™1000 were 1.3 ± 2.3% and 19.7 ± 1.2% (n = 3), respectively. Using the filtration mode at 1 L/h, the mean adsorption rates in the ST™150 and AV™1000 were 1.7% (n = 2) and 18.5% (n = 2), respectively.
Conclusion:
ST™150 filter sequestrated very limited quantities of cefepime. In the diafiltration and filtration modes, AV™1000 sequestered cefepime at about 19%. The adsorption rate seems independent of the flow rate. Further studies would be needed to assess, in particular, the clinical relevance of these results in adults as well as drug adsorption in the pediatric population.
Keywords
Introduction
Cefepime, a fourth-generation cephalosporin antibiotic, has a broad spectrum of activity against Gram-positive and Gram-negative bacteria, including Pseudomonas aeruginosa. 1 Its enhanced stability against beta-lactamases and improved penetration into bacteria make it an attractive choice for treating severe infections in critically ill patients.1,2
Pharmacokinetic studies have shown that cefepime has a linear pharmacokinetic profile, is primarily eliminated unchanged by the kidneys, and has an elimination half-life of approximately 2 h in healthy adults. In patients with renal impairment, the half-life is prolonged and dose adjustments are necessary, based on creatinine clearance.3–6
In the intensive care setting, patients often develop acute kidney injury necessitating continuous kidney replacement therapy (CKRT). CKRT can significantly alter the pharmacokinetics of drugs, especially those that are primarily eliminated by the kidneys like cefepime. 7 Subtherapeutic antibiotic concentrations may lead to treatment failure and development of resistance, while excessive levels may cause neurotoxicity, a recognized adverse effect of cefepime. 8
Although dosing recommendations for cefepime during CKRT have been proposed, based on pharmacokinetic data, 9 there is a paucity of data on the actual clearance of cefepime by different CKRT modalities and settings. One in vitro study evaluated the sieving and saturation coefficients of cefepime in the dialysis mode with no mention of adsorption, 10 while some others assessed its elimination by dialysis and filtration in clinical studies.11–13 In addition, Green et al. 14 reported minimal adsorption of cefepime in a polyarylethersulfone filter in an ex vivo CKRT circuit dedicated to assess drug adsorption.
Given the widespread use of cefepime in critically ill patients and the high prevalence of CKRT in this population, a more thorough characterization of cefepime elimination using different filters is crucial to optimize dosing. The present in vitro study aims to quantify cefepime elimination by filtration, dialysis, and adsorption using the NeckEpur® method that closely mimics the clinical scenario bedside.15–19
Materials and methods
Cefepime
Cefepime dihydrochloride monohydrate was supplied by Mylan and 2 g were diluted with 20 mL of saline solution. A 5-L Hemosol® bag, used as a central compartment (CC), was loaded with cefepime solution at a targeted concentrations of 50 mg/L. The filter was initially exposed to the maximum concentration of cefepime.
NeckEpur® method
We designed two in vitro CKRT circuit configurations (NeckEpur®, Paris, France), 19 the continuous diafiltration mode (CDF) and continuous filtration mode (CF). CKRT procedures were performed with two different filters, ST™150 and AV™1000, using the NeckEpur® method designed to simultaneously determine the respective roles of dialysis, filtration, and adsorption. The methodology is further explained in previous publications15–20 without modification in the present study. The NeckEpur® method is designed to simultaneously determine the respective roles of dialysis, filtration, and adsorption. The methodology is further explained in previous publications15–20 without modification in the present study.
CKRT modes and devices
The total flow rate for continuous diafiltration (CDF) was set to 2.5 L/h, combining 1 L/h of dialysis and 1.5 L/h of filtration, which included a pre-dilution rate of 0.5 L/h and a post-dilution rate of 1 L/h. Conversely, the total flow rate for continuous filtration (CF) was set to 1 L/h with post-dilution. The devices used for the filter and dialyzer were the Prismaflex® monitor with the ST™150 filter (Baxter-Gambro), and the Multifiltrate Pro monitor with the AV™1000 filter (Fresenius). ST™150 (polyacrylonitrile) and AV™1000 (polysulfone) were selected as they represent the two most commonly used filters in intensive care units worldwide. Their different physicochemical properties (electrical charge, surface area) make them ideal candidates to study the impact of these characteristics on drug sequestration.
Sampling
Samples were taken in the central compartment (CC), at the inlet (Cin), at the outlet (Cout) of the filter, and at the effluent tube (Ceffl instant) at 0, +15, +30, +45, and +60 min, then at + 2, 3, 4, and 6 h. Cumulative effluents were also sampled.
Method of cefepime concentration measurement
Cefepime concentrations were measured by an analytical method with online extraction procedure (TurboFlow™). Cefepime and the stable isotopically labeled internal standard ([2H5]-Cefepime) were extracted from either sample by a turbo flow liquid chromatographic method (MCX-2 (0.5 mm × 50 mm) column, Thermo Scientific®) and eluted by Hypersil Gold aQ (3 mm × 50 mm; 5 µm) column; Thermo Scientific®. Mass spectrometry was conducted using an exact mass determination method by electrospray positive ionization high-resolution mass spectrometry (Orbitrap, Thermo Scientific®). The run time was 10 min. The LLOQ and ULOQ were determined to be 0.4 and 100 μg/mL, respectively.
Statistical, pharmacokinetic, and graphical analysis
The GraphPad Prism® V9 software was used for column statistics. The NeckEpur® spreadsheet was used for pharmacokinetic calculation (e.g. area under the curve (AUC) calculation, extraction coefficient (EC), and Sieving coefficient (Sc)).
Results
Stability in the CC and the effluent bag of AV™1000
The mean initial measured concentration was 52.4 ± 4.2 mg/L. The difference of mean concentrations between T0 and T + 6 h was −9.1%.
Pharmacokinetics and route of elimination of cefepime during CDF mode at 2.5 L/h flow rate
Pharmacokinetic parameters and routes of elimination of cefepime in the continuous diafiltration mode at 2.5 L/h using the ST™150 and AV™1000 filters.
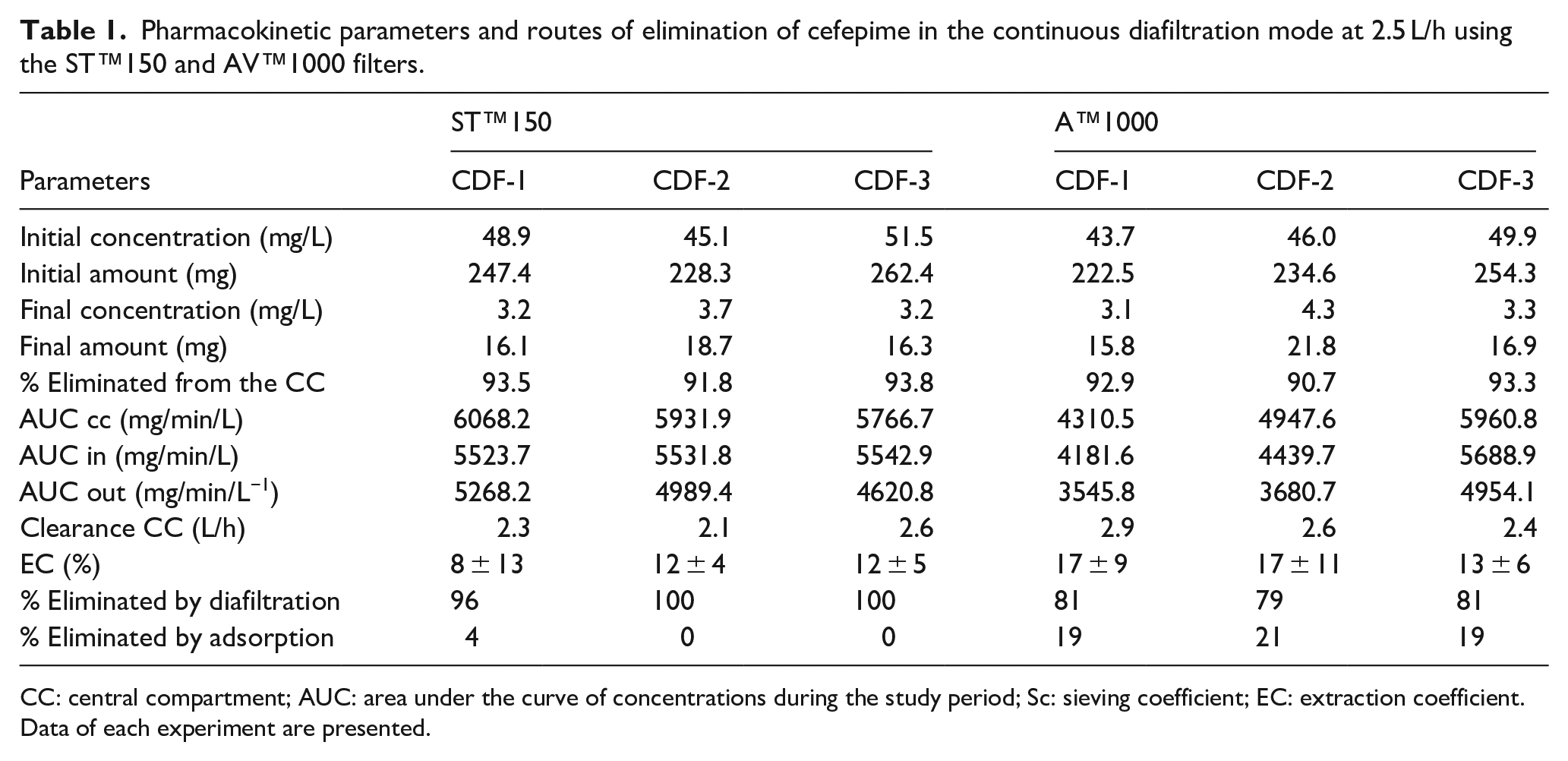
CC: central compartment; AUC: area under the curve of concentrations during the study period; Sc: sieving coefficient; EC: extraction coefficient.
Data of each experiment are presented.
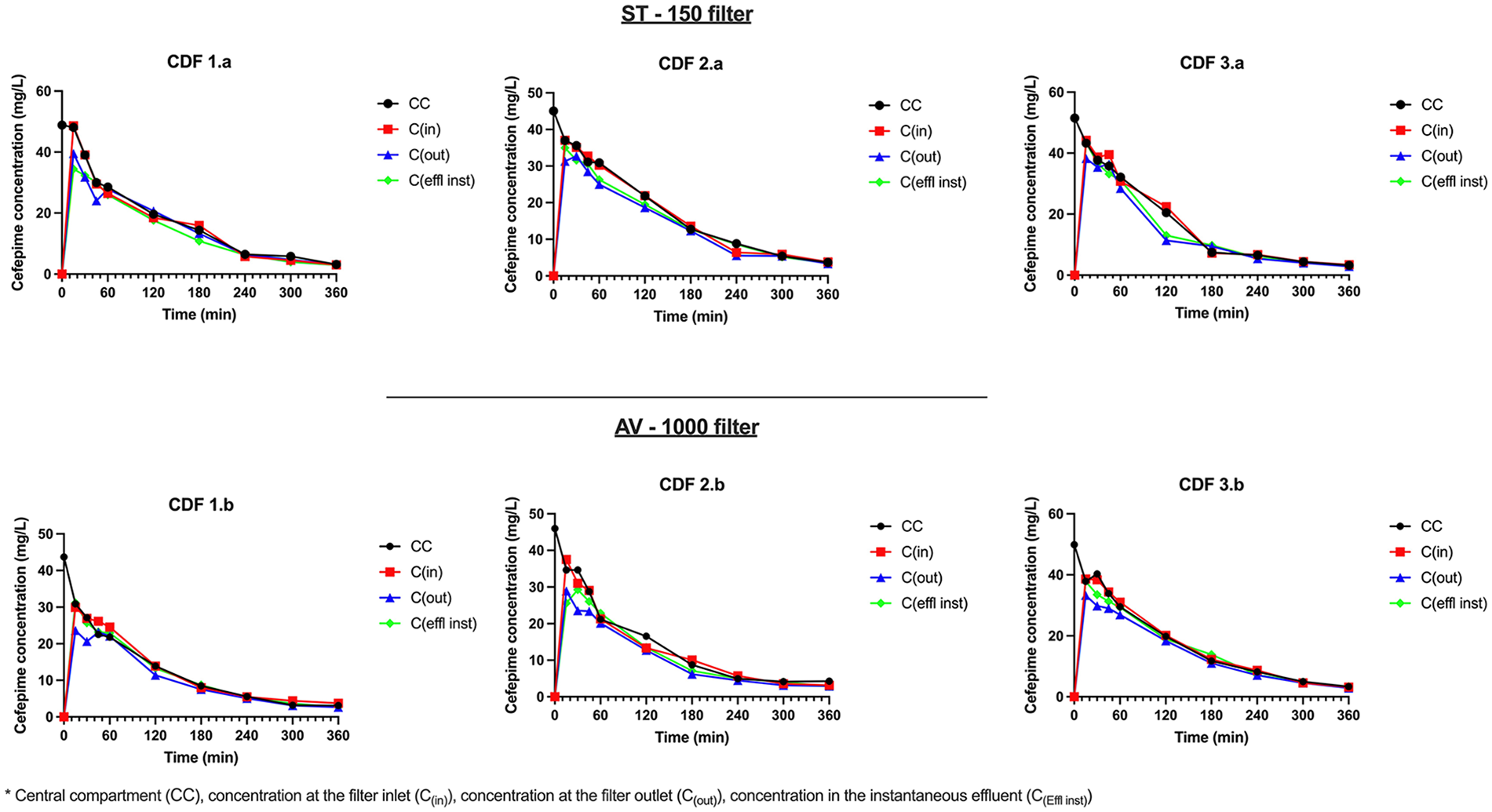
Upper panel shows the time-course of concentrations of cefepime in the different compartments in the CDF (2.5 L/h) sessions performed using the ST™150 filter. Lower panel shows the time-course of concentrations of cefepime in the different compartments in the CDF sessions performed using the AV™1000 filter.
The mean initial concentration was 48.5 ± 3.2 mg/L corresponding to an initial amount of 245.9 ± 17.1 mg. The mean percentage of cefepime eliminated for the CC was 93.0 ± 1.1%. The mean AUCs in the CC, inlet, and outlet ports were respectively 5922.3 ± 151.0, 5532.8 ± 9.6, and 4959.5 ± 324.7 mg/min/L, respectively. The mean clearance from the CC was 2.3 ± 0.3 L/h. The mean EC was 10.7 ± 2.3%. The mean percentages of elimination by diafiltration and adsorption were 98.7 ± 2.3% and 1.3 ± 2.3%, respectively.
The mean initial concentration was 46.5 ± 3.13 mg/L corresponding to an initial amount of 237.13 ± 16.1 mg. The mean percentage of cefepime eliminated for the CC was 92.3 ± 1.4%. The mean AUCs in the CC, inlet, and outlet ports were respectively 5073 ± 832.3, 4770.1 ± 806.1, and 4060.2 ± 777.1 mg/min/L, respectively. The mean clearance from the CC was 2.63 ± 0.3 L/h. The mean EC was 15.7 ± 2.3%. The mean percentages of elimination by diafiltration and adsorption were 80.3 ± 1.2% and 19.7 ± 1.2%, respectively.
Pharmacokinetic parameters and routes of elimination of cefepime in the continuous filtration mode at 1.0 L/h using the ST™150 and AV™1000 filters.
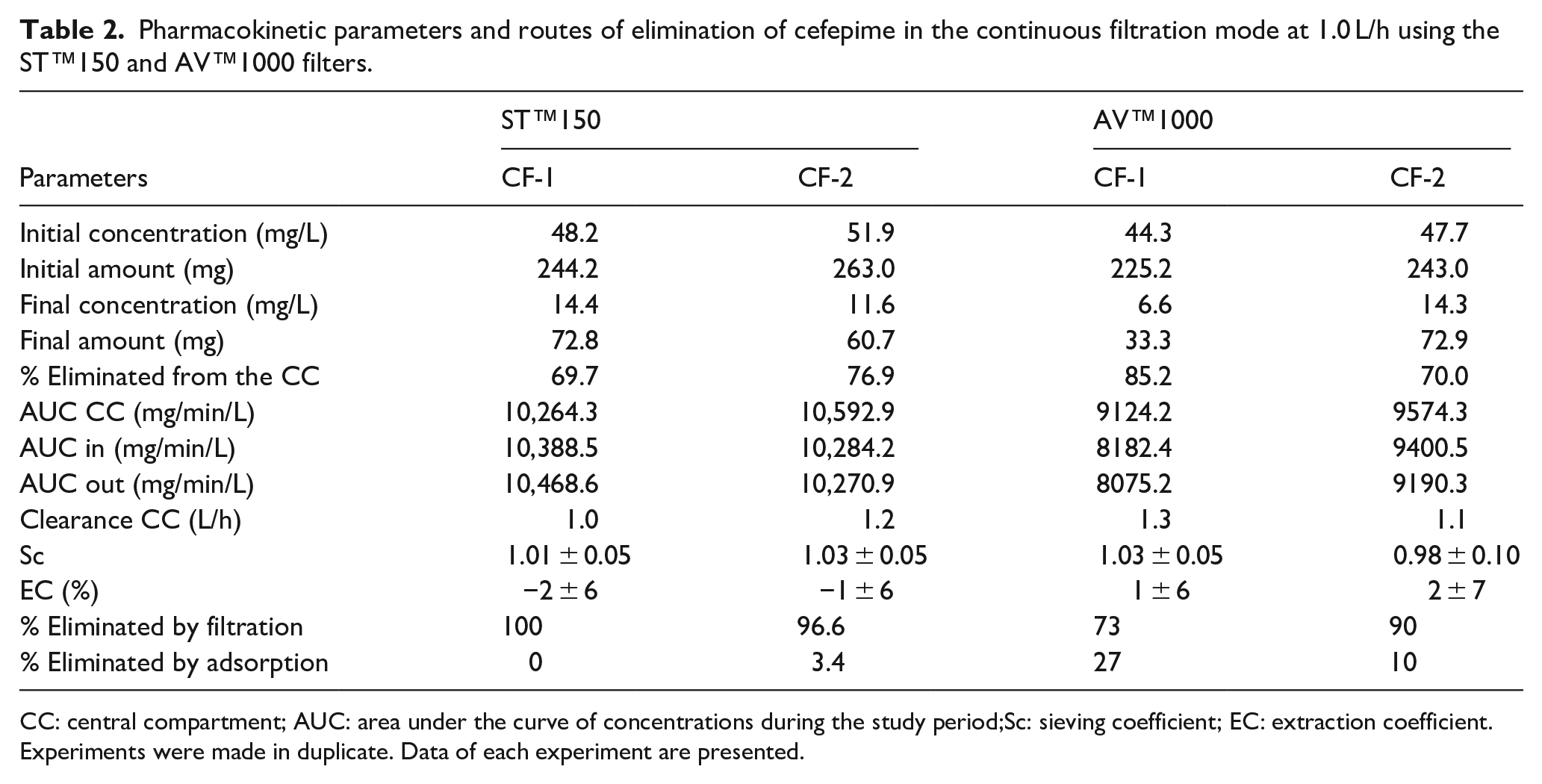
CC: central compartment; AUC: area under the curve of concentrations during the study period;Sc: sieving coefficient; EC: extraction coefficient.
Experiments were made in duplicate. Data of each experiment are presented.
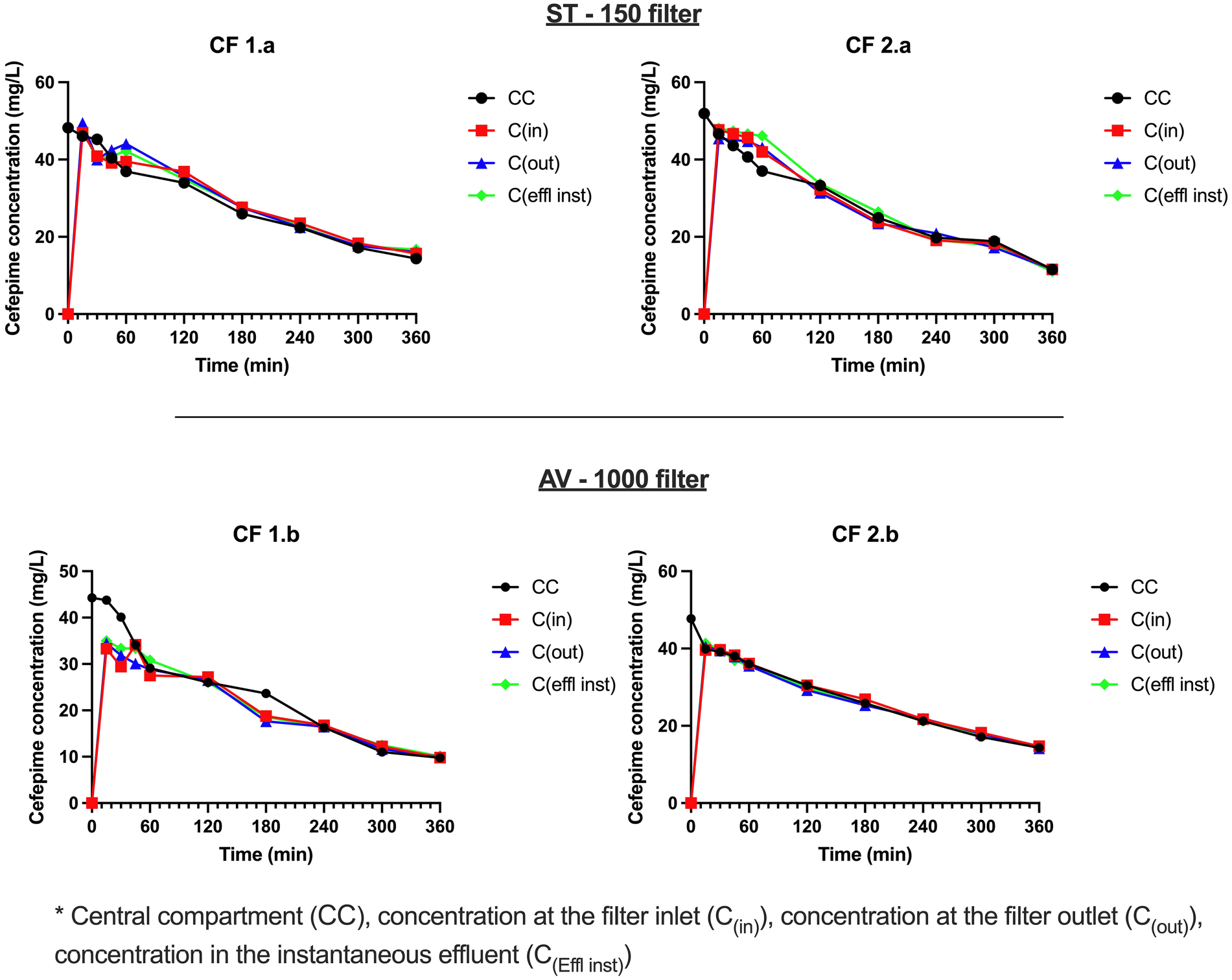
Upper panel shows the time-course of concentrations of cefepime in the different compartments in the CF (1.0 L/h) sessions performed using the ST™150 filter. Lower panel shows the time-course of concentrations of cefepime in the different compartments in the CF sessions performed using the AV™1000 filter.
The mean initial concentration was 50.1 mg/L corresponding to an initial amount of 253.6 mg. The mean percentage of cefepime eliminated for the CC was 73.3%. The mean AUCs in the CC, inlet, and outlet ports were respectively 10,428.6, 10,336.4, and 10,369.8 mg/min/L, respectively. The mean clearance from the CC was 1.1 L/h. The mean Sc was 1.02 ± 0.05. The mean EC was −1.5 ± 5.5%. The mean percentages of elimination by filtration and adsorption were 98.3% and 1.7%, respectively.
The mean initial concentration was 46 mg/L corresponding to an initial amount of 234.1 mg. The mean final concentration was 10.45 mg/L corresponding to a final amount of 53.1 mg. The mean percentage of cefepime eliminated for the CC was 77.6%. The mean AUCs in the CC, inlet, and outlet ports were respectively 9349.3, 8791.5, and 8632.8 mg/min/L. The mean clearance from the CC was 1.2 L/h. The mean Sc was 1 ± 0.03. The mean EC was 1.5 ± 0.7%. The mean percentages of elimination by filtration and adsorption were 81.5% and 23.5%, respectively.
Discussion
Adsorption of antibiotic may lead to too low plasma concentrations in patients resulting in delaying efficient dosage regimen, increased treatment costs, and ultimately in treatment failure.21–24 Demonstrating the absence of drug adsorption or of a clinically non-relevant drug adsorption should be considered as a major advance forward in definitively concluding that there is no interaction between a specific drug and a specific medical device.
The NeckEpur® methodology uses the same crystalloid solution in the different compartments of the model and focuses on the free fraction of drugs in plasma, which is the active fraction responsible for pharmacological activity, metabolism, and elimination through physiological and non-physiological routes.25–27 In contrast, most authors use reconstituted/diluted blood, which induces several biases. Indeed, protein binding may lead to reversible physiological drug sequestration in plasma, while blood cell distribution adds another factor of drug sequestration which is assessed by measuring the blood-to-plasma ratio of drugs. 28 Moreover, spontaneous hemolysis occurring 1 h after blood collection may contribute to false positive (BTPR < 1) and false negative adsorption rates (BTPR > 1). Studying the unbound fraction of antimicrobial agents is in line with the European Committee on Antimicrobial Susceptibility Testing recommendations to determine bacterial minimum inhibitory concentrations (MICs) using the unbound antimicrobial fractions. 29 There is a growing interest in studying the elimination of unbound fractions of antimicrobial agents like ceftolozane-tazobactam by CKRT. 30 This was previously reported by Pfaller et al. 31 who emphasized the reference method for evaluating antifungal MICs which should be based solely on the unbound fraction.
Population pharmacokinetics (PopPK) of cefepime in patients requiring CKRT using either polyacrylonitrile filters10,11,32,33 or polysulfone-derived filters were reported.3,10,12,34,35 However, PopPK analysis are designed to study interindividual variability with no particular design to unveil drug adsorption.
Our study focuses on 10 sessions of CKRT with the ST™150 and AV™1000 filters, set to two different flow rates, 1 and 2.5 L/h. The choice of the 1 L/h flow rate was based on a previous study performed by NeckEpur which showed for amikacin that lower flow rates lead to increased adsorption rates. 16 In contrast with amikacin, in this present study the adsorption rate of cefepime in AV™1000 filter at flow rates set to 2.5 and 1 L/h were 19.7 ± 1.2% and 23.5%, respectively. This finding suggests a flow-independence of cefepime adsorption.
The mean adsorption rates using the ST™150 in the CDF/2.5 L/h and CF 1 L/h were 1.3 ± 2.3%, respectively. In contrast, the adsorption rates in the AV™1000 at the same modes and flow rates were 19.7 ± 1.2 and 23.5%%, respectively. Phillips et al. 36 set a threshold value of 17% to conclude that the interaction was relevant while In our in vitro studies, we set a threshold value of 20%.17,18,37–39 Therefore, we conclude that the AV™1000 induces a significantly greater adsorption rate of cefepime as compared to the ST™150 one. The AV™1000 filter shows significant cefepime adsorption under experimental conditions, something which could have serious clinical impact. One major limitation results from the use of conditions corresponding to an adult population while it would be interesting and of value to assess cefepime adsorption in pediatrics.
Conclusion
There is a significant cefepime adsorption in the AV™1000 and a clinically non-significant adsorption in the ST™150 filter. Further studies are required to clarify cefepime adsorption in the AV™1000 filter in both adult and pediatrics.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.