
Abstract
Platelet derived prothrombotic microparticles (MP) have been associated with hemocompatibility related adverse events in patients with continuous flow left ventricular assist devices; little is known with the contemporary Impella platform micro-axial flow pumps. Indeed, the extended duration of support provided by the Impella 5.5 calls for a specific evaluation. We report for the first time two patients in whom MP have been assessed during Impella 5.5 and concomitant dual antiplatelet and direct thrombin inhibitor therapy. Interestingly, the patients showed significantly different profile in overall MP release (peak: 78.1% vs 2.7%), which was not correlated to lactate dehydrogenase nor platelet count. The patient with the higher values suffered from minor stroke 4 days after pump removal, when systemic anticoagulation with Bivalirudin had been stopped. These preliminary data might envision a new predictor of hemocompatibility related adverse events in patients with Impella, and a rethinking on the post support antithrombotic strategy.
Introduction
Microparticles (MP) are small vesicles (0.1–1.0 μm), originating from circulatory and vascular wall cells, consisting of anuclear fragments of cellular membrane and cytoplasmic material. They are generated during cell activation or damage and represent end-products of cellular injury and apoptosis of different cells, leukocytes, erythrocytes, endothelial cells and, above all, platelets. 1 MP formation implies structural alteration and different protein expression, as a result of cellular activation or disruption; anionic phospholipids are externalized, especially phosphatidylserine: these molecules can activate inflammatory reactions, but they can also trigger and propagate the coagulation cascade so that MP can act as deregulators of endothelial and circulatory homeostasis. 2
These particles, released both after physiological and pathological stimuli, 3 can be used as detectable biomarkers of cellular stress and damage and have the potential to become a clinical diagnostic tool.
One of the most recent fields of application is the evaluation of the MP role in hemocompatibility of mechanical circulatory support. 4 Circulating cells are not only impacted by the non-pulsatile non-physiological flow, but also by the device itself: mechanical stress can cause disruption of cellular integrity, apoptosis, and MP generation. Diehl et al. 5 reported that MP levels were significantly higher in left ventricular assist device (LVAD) patients compared to healthy controls. Similarly, Sansone et al. 6 showed that MP levels of both platelet and endothelial origin were significantly increased in LVAD patients when compared to controls. Nascimbene et al. 7 showed that the concentration of MP was significantly higher in patients who developed an hemocompatibility related adverse event; in patients without adverse events, no significant change in the concentration of MP was observed after LVAD implantation and at 3 months follow up.
These results suggest that measurement of circulating MP in peripheral blood might be a promising predictor of device-associated adverse events. Notwithstanding, the contemporary value of Impella technology in patients with cardiogenic shock calls for a reduction of hemocompatibility adverse events. Given the mechanical forces generated by the pump, MP might be a target or a signal to tackle these complications.
We report two cases of patients admitted to our hospital for myocardial infarction complicated by cardiogenic shock and treated with Impella 5.5 in whom we determined MP in peripheral blood.
Case report
Case 1
A 74-year-old man, smoker, obese, and with hypertension, was admitted to the emergency department for prolonged chest pain at rest. The ECG showed anterior ST elevation myocardial infarction (STEMI). First left ventricle ejection fraction (LVEF) was 40% with anterior and septal apical segments akinesia; right ventricle dimensions and function were normal. Urgent coronary angiography showed multi-vessels disease and primary percutaneous coronary intervention (PCI) on the culprit lesion was performed.
A progressive decline of hemodynamic and echocardiographic parameters was observed, unresponsive to inotropes evolving to cardiogenic shock (Society for Cardiovascular Angiography and Intervention Shock Stage (SCAI D)). After 72 h, the mechanical circulatory support (MCS) team decided for Impella 5.5 support, surgically implanted via right axillary artery; subsequent protected PCI for full revascularization was performed. Bivalirudin was administered to achieve an activated partial thromboplastin time (aPTT) of 60–80 s, on top of dual antiplatelet therapy (DAPT; clopidogrel and aspirin).
After 34 days of support, heart recovery was observed. Weaning from mechanical support was complicated by rhythm instability with occurrence of atrio-ventricular third grade block, alternated to atrial fibrillation; a definitive pacemaker was implanted. Heart failure medical therapy was slowly introduced. Triple anti-thrombotic therapy was ended after 1 month and shifted to Warfarin + acetylsalicylic acid (ASA).
The patient was finally discharged from hospital and started a cardiac rehabilitation program.
Case 2
A 75-year-old man was admitted to our emergency department for chest pain at rest: anterior STEMI was diagnosed. He had known coronary artery disease, with previous inferior myocardial infarction in 2006 and NSTEMI in 2019. At presentation LVEF was 15%, with preserved right ventricular function and no evidence of valvular disease. Coronary angiography showed three-vessels disease, with culprit lesion on left main-anterior descending artery, and chronic total occlusion of circumflex and right coronary arteries. Primary PCI on left main-left anterior descending (LAD) was performed.
After 24 h cardiogenic shock worsened (SCAI C >D) and Impella 5.5 was surgically implanted via the right axillary artery. Bivalirudin was administered to achieve an aPTT of 60–80 s, on top of DAPT (ticagrelor and aspirin). During the first hours, the patient presented numerous episodes of ventricular fibrillation, successfully treated with DC shock and intravenous lidocaine. He was extubated after 48 h. A total of 13 days of mechanical support was necessary to obtain heart recovery. At MCS explant LVEF was 30%, with residual anterior and septal apical segments hypokinesia. Bivalirudin was stopped and prophylactic low molecular weight heparin was administered; DAPT was maintained.
Four days after Impella removal, the patient complained of left arm paresthesia and hypoesthesia; slight lateral deviation of the labial fold was observed. Cranial CT scan was urgently performed and revealed a tiny region of hypodensity in the right semioval center. Neurological evaluation concluded for a minor stroke (National Institutes of Health Stroke Scale 2). There was no evidence of atrial fibrillation at ECG monitoring over the last 48 h.
During Impella support peripheral venous blood was collected from the two patients, using 21-G needles into sodium citrate 0.019 M–3.2% tubes, avoiding prolonged use of a tourniquet and discarding the first 2/3 mL to avoid the contact phase activation. Platelet poor plasma (PPP) was prepared within 30 min after blood collection by double refrigerated centrifuge (2 min × 15 min at 2500g), using the lowest or no deceleration, and collecting plasma. Then aliquots of 500 µL were immediately frozen and stored at 80°C until use. Immediately before assay, we proceeded with the thaw of samples by incubation for 5 min in a water bath at 37°C. Thus, the samples were stained with the following procedure: 10 µL of each sample were incubated with 10 µL of CD61 PC7 conjugated monoclonal antibody, 10 µL Annexin V FITC conjugated monoclonal antibody, 5 µL CD45 KO conjugated monoclonal antibody (Beckman Coulter), for 30 min at dark and 4°C temperature. Subsequently, the samples before the analysis were resuspended in 400 µL of Annexin V kit binding buffer (Beckman Coulter) then were analyzed using the DXFlex flow cytometer (Beckman Coulter) for 500 s on slow using 405 nm violet side scatter (ASSC) trigger. To prevent cross-concentration between samples, a PBS wash done between each sample. We identified Platelet Extracellular Vesicles (PEVs) as double positive Annexin-V and CD61 events (Figure 1).
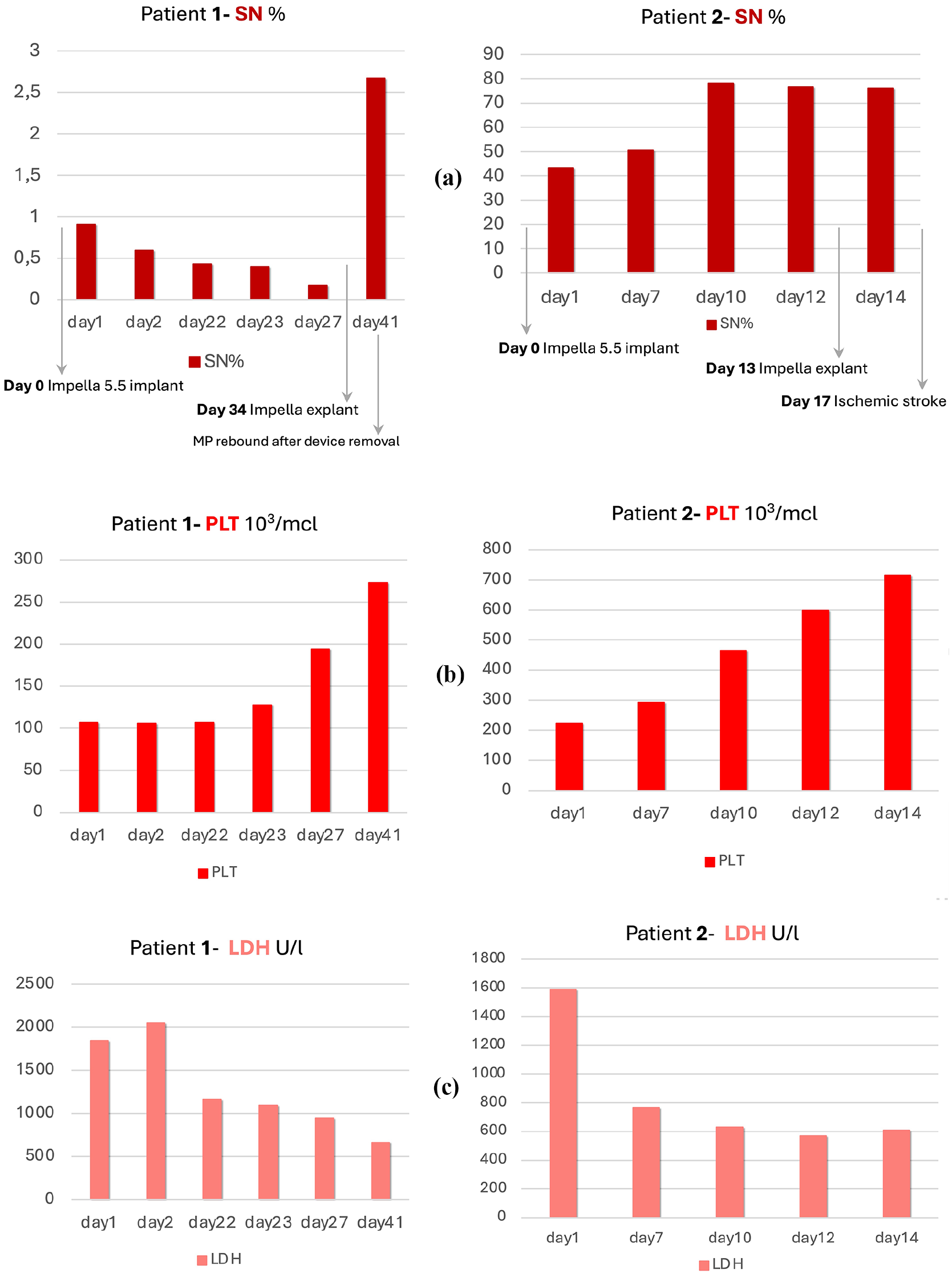
Percentage of platelet-derived microparticles, identified as double positive Annexin-V and CD61 (a); platelets count (b) and lactate dehydrogenase (LDH) levels (c) in patients 1 (on the left) and 2 (on the right). a. The patients showed marked differences in terms of microparticles release overall, with patient 2 having significantly higher levels (peak: 78.1% vs 2.7%); in patient 2 levels of platelet-derived microparticles increased during Impella support and remained high, while patient 1 showed lower levels at the beginning that slightly decreased, with a final rebound after device removal. b. Platelets trends during support were similar in patient 1 and patient 2. Interestingly, patients showed an increase of platelet and MP count after Impella removal and bivalirudin discontinuation (day 34 for patient 1; day 13 for patient 2). c. Neither patient 1 nor patient 2 showed significant alteration in plasma levels of LDH during support (peak 2045 U/L vs 1589 U/L).
Discussion
Acute MCS systems use has risen dramatically in the management of cardiogenic shock and Impella CP has been shown superior to standard therapy in the DANGER Shock trial. 8 Device selection on clinical grounds is driven by many clinical features, but also by differences in device performance and hemocompatibility. Finding the balance between bleeding and thrombosis and, moreover, the prediction and prevention of clinically relevant events represent a major issue in MCS management.
Early thrombus detection is challenging: increasing hemolysis, pump power consumption, or, in extreme cases, clinical overt pump thrombosis are late signals. Similarly, minor bleeding can be observed, as well as clinically relevant hemorrhage, reflecting the final step of coagulation imbalance. A major clinical impact might be obtained by estimating the status of ongoing hemostatic dysregulation and tackle with specific therapies, in order to prevent the occurrence of complications.
The antithrombotic strategy is crucial but might be insufficient and administration of anticoagulants and/or antiplatelets might just increase the risk of hemorrhage.
The increase of MP, especially the procoagulant populations, with ability to bind coagulation factors and usher thrombin generation, was suggested to be a predecessor of MCS related thrombotic complications. The underlying pathogenesis is not completely understood but MPs may participate in the equilibrium between anti and pro-thrombotic states, as they contain anticoagulant factors present in platelets, but also promote the generation of procoagulant factors 9 ; MPs deficiency (Castman’s defect) or the impaired ability to generate MPs (Scott’s syndrome) are associated to bleeding tendency 10 ; by contrast, platelet derived MPs levels are increased in patients with recent myocardial infarction 11 and are suggested to be strictly involved in the atherosclerosis progression from initiation of fatty streak to the atherothrombotic acute event. 12
Most of the current knowledge about hemocompatibility related device complications is derived from LVAD experience. The loss of high-molecular-weight von Willebrand Factor was firstly studied 13 ; it is known that arterio-venous malformation can occur in LVAD patients 14 and the incidence of ischemic and hemorrhagic stroke is increased. Blood exposure to shear stress forces generated by LVAD pump on circulatory and endothelial cells is associated to hemolysis but also to alteration of platelet morphology and a continuous generation of MP and can lead to a sustained proinflammatory and procoagulant state. Recent clinical reports demonstrated a correlation between number of circulating MPs and occurrence of adverse events in patients with LVADs.5,6,15
The pathogenesis of hemocompatibility issues is similar for LVAD and Impella (Figure 2): the artificial surface of the device is thrombogenic; shear stress induces platelet activation and hemolysis. Among the different Impella pumps, 5.5 is the most recent device. One of the key differences are the motor bearings, made of ceramic: toward blood flow, ceramic components generate less friction and heat, resulting in less protein deposition and significant lower risk of thrombosis and hemolysis; however, high-speed continuous micro-axial blood propulsion is associated to platelet activation and MPs generation. Yana Roka-Moiia et al. 16 demonstrated that the number of MP is increased in both Impella 5.5 and Centrimag-sheared samples as compared with nonsheared controls; Impella 5.5 was shown to be less damaging, demonstrating a lower degree of platelet count decrease and MP generation as compared to Centrimag.
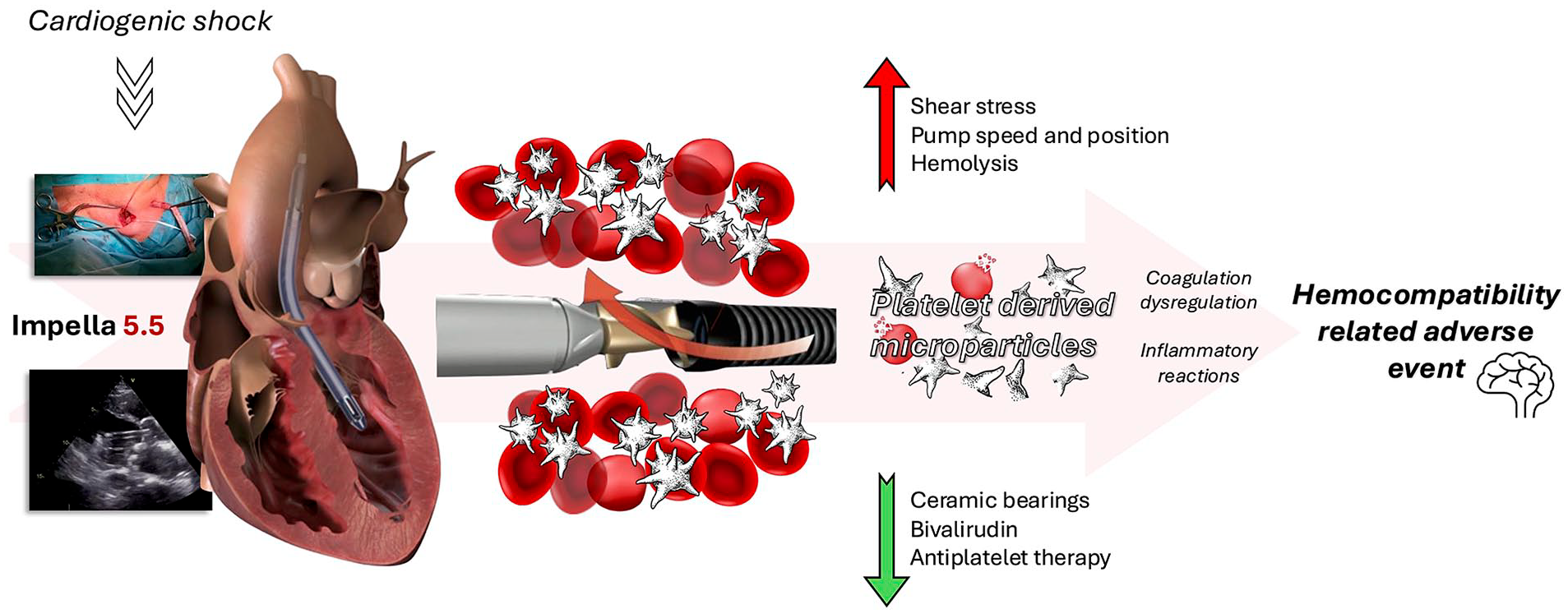
Centrale Figure. From left to right: surgical right axillary artery access and transthoracic echocardiography check of Impella 5.5 correct positioning in parasternal long-axis view; during Impella activity, hemolysis phenomena and platelet derived microparticles formation are exacerbated by shear stress, incorrect pump position and high rotation speed, while they are mitigated due to Impella 5.5’s own structural features (above all, the ceramic bearings) and a proper management of antithrombotic therapy. Platelet derived microparticles are associated to coagulation dysregulation and inflammatory reactions, which can result in hemocompatibility related adverse events.
Hemocompatibility phenomena, however, are not reproducible across all patients despite similar antithrombotic therapy; indeed, multiple factors might play a role in the patient specific profile: pump speed and position amongst all, but also residual heart function and suction events.
We described two cases of MP assays during Impella 5.5 support and we assume a possible relation between higher circulating MPs levels and an adverse thrombotic event after pump removal (patient 2), but sample size is obviously insufficient for statistical measurements and it is not possible to draw definitive conclusions.
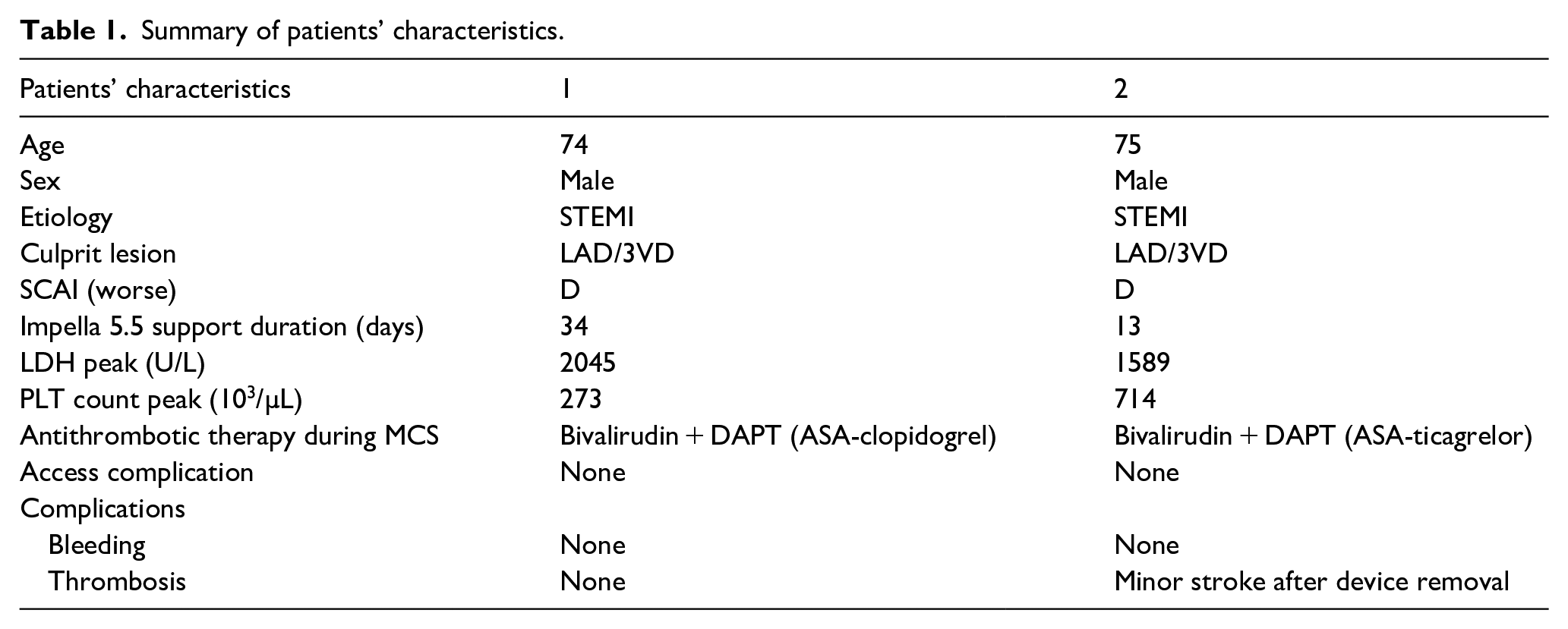
The two patients had different initial absolute platelets levels, but they exhibited a similar increasing trend during mechanical support; no significant difference was observed in lactate dehydrogenase (LDH) release. As a matter of fact, our two patients, despite sharing similar baseline clinical profile and antithrombotic treatment (Table 1), showed different MP release and clinical outcomes: MP were significantly increased in patient 2 (Figure 1); at pump removal and discontinuation of bivalirudin, they both presented a rebound increase in platelet count and MP levels. Interestingly, the stroke occurred 4 days after device removal, as if persistent high level of circulatory MP could represent a mid-term signal of thrombotic risk, which was probably early mitigated by systemic anticoagulation with Bivalirudin.
Summary of patients’ characteristics.
In this perspective, the hemocompatibility adverse event presented after Impella support might be considered not necessarily “pump associated,” rather as a rebound phenomenon following an abrupt change of the hemostatic milieu. This concept might turn into clinically relevant management, as identification of this risk profile, as assessed via MP, would turn into a continuation of systemic anticoagulation until these phenomena definitely vanish.
At present, the contemporary management of Impella pumps is based on a standardized protocol of systemic anticoagulation with unfractionated heparin or bivalirudin, and single antiplatelet therapy or DAPT are usually administered on the basis of extrapump indications (mainly acute coronary syndrome and PCI). A thorough evaluation of the hemostatic context and the availability of targeted therapies might significantly improve clinical results, especially thrombotic complications which are currently identified only when clinically overt. On top of that, enhanced pump management (pump positioning and speed optimization, avoidance of suction) might also play a role. Potential acknowledgement of the hemostatic effects of pump removal might as well envision new management strategies.
In conclusion, the broad application of Impella support for cardiogenic shock calls for urgent in depth evaluation of the coagulation background of this therapy and new clinical approaches in order to reduce the hemocompatibility related adverse events. Signals for detection of thrombotic risk are needed. Cells fragmentation via the pump rotation and MP generation might play a role. Their quantification, correlated to clinical data, could become a new strategy for early stratification of thrombotic risk in patients supported by Impella 5.5 and potentially a marker to guide patient tailored clinical management.
Footnotes
Acknowledgements
We thank the CTV ICU nurses of AOU SS. Antonio e Biagio e Cesare Arrigo, Alessandria.
Author contributions
NDE: design of the work; acquisition, analysis, and interpretation of data; and manuscript drafting. AC and GM: acquisition and interpretation of data. AP, TB, and MMC: lab assays and interpretation of data. FP: conceptualization and design of the work; analysis and interpretation of data; and manuscript drafting and final revision.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: FP is consultant for Abiomed. All other authors have nothing to disclose.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations and consent to participate statements
In accordance to the EU Regulation 536/2014, all competent patients provided written informed consent, whereas consent was waived for patients who were not competent on admission. Institutional Review Board number and date of approval: ASO.RianCTV.21.01 CE 18/11/2021, prot.n°0003914- 07/01/2022.