
Abstract
Introduction:
This study aimed to investigate the association of exposure below various thresholds of mean arterial pressure (MAP), pump flow rates, and hemoglobin levels during cardiopulmonary bypass (CPB) with cardiac surgery-associated acute kidney injury (CSA-AKI).
Methods:
Adult patients undergoing cardiac surgery with CPB at a university hospital between April 2015 and August 2023 were included. The primary outcome was CSA-AKI within 7 days postoperatively. The primary exposures were the area under the threshold (AUT) of MAP, pump flow rate, and Hb during CPB. A multivariable logistic regression using covariates selected via Lasso regularization estimated the adjusted odds ratios (aORs) and 95% confidence intervals (CIs).
Results:
We finally analyzed 333 patients, of which 156 patients (46.8%) developed CSA-AKI. The AUT of hemoglobin, but not those of MAP and pump flow rate, was associated with CSA-AKI. The lower the threshold, the stronger the association (<8 g/dL, aOR = 1.132 per 10 g/dL × min, 95% CI = 1.036–1.243, p = 0.007; <9 g/dL, aOR = 1.048, 95% CI = 1.013–1.086, p = 0.007; and <10 g/dL, aOR = 1.027, 95% CI = 1.007–1.048, p = 0.010).
Conclusion:
Hemoglobin levels during CPB below 8.0 g/dL were associated with CSA-AKI, while MAP and pump flow rates indicated no such association.
Keywords
Introduction
Cardiac surgery-associated acute kidney injury (CSA-AKI) is one of the most serious complications of cardiac surgery, 1 with an incidence of 5%–43%. 2 It is caused by various factors, such as ischemia/reperfusion injury, neurohormonal activation, inflammatory response, oxidative stress, and surgical stress, in part owing to the adoption of cardiopulmonary bypass (CPB).1,3 CSA-AKI prevention is crucial as it is associated with increased postoperative morbidity and mortality rates, prolonged hospital stay, and high medical costs. 4
Previous studies have investigated the association between CSA-AKI and various intraoperative modifiable parameters, including mean arterial pressure (MAP), 5 oxygen delivery (DO2), 6 blood temperature, 7 blood loss, 8 transfusion, 9 infusion volume, 10 hemoglobin (Hb) level, 9 and CPB time. 11 Based on these findings, clinical guidelines for the prevention of CSA-AKI have been developed.12,13 Recently, goal-directed perfusion targeting a DO2 threshold of >280 mL/min/m2 has been recommended. 13 However, surgeons and anesthesiologists often rely on more direct and intuitive parameters such as MAP, pump flow rates, and Hb levels. Moreover, the optimal management goals for the key determinants of DO2, such as pump flow rates and Hb levels, have not been clearly established. While no advantages has been found in maintaining MAP at higher levels during CPB, 13 MAP remains a key circulatory parameter that is modifiable during CPB. Therefore, this study aimed to investigate the association of exposure below various thresholds of MAP, pump flow rates, and Hb levels during CPB with CSA-AKI.
Methods
The study was approved by the Nagoya City University Graduate School of Medical Sciences and the Nagoya City University Hospital Institutional Review Board (60-23-0125, January 9, 2024). Eligible participants were given the opportunity to opt out of the study on the website of the Nagoya City University Hospital Clinical Research Management Center (https://nagoya-cu.bvits.com/rinri/publish.aspx). The manuscript conforms to the guidelines of the “Strengthening the Reporting of Observational Studies in Epidemiology.” 14
Study design and subjects
This single-center retrospective cohort study included patients aged ⩾18 years who underwent cardiac surgery via CPB at Nagoya City University Hospital between April 1, 2015, and August 1, 2023. During this period, CPB techniques were standardized, allowing for the high-quality data collection. The exclusion criteria were patients managed with nonstandard CPB (applying circulatory arrest or partial extracorporeal circulation for aortic surgery), with preoperative renal failure (blood purification therapy within 7 days preoperatively, preoperative serum creatinine (sCr) level ⩾4.0 mg/dL or preoperative estimated glomerular filtration rate (eGFR) <15 mL/min/1.73 m2), with preoperative mechanical circulatory support, with preoperative mechanical ventilation, who received continuous infusion of inotropes or vasopressors preoperatively, who had undergone other surgery within 7 days preoperatively, or with missing outcome or exposure data.
Outcomes
The primary outcome was stage ⩾1 AKI diagnosed according to the Kidney Disease: Improving Global Outcomes (KDIGO) criteria within 7 days after surgery. 15 The secondary outcome was stage ⩾2 AKI, as diagnosed according to the KDIGO criteria.
The KDIGO criteria define the AKI stages as follows: stage 1, ⩾0.3-mg/dL increase in sCr level from baseline within 48 h, 1.5–1.9 times increase in sCr level from baseline, or urine output <0.5 mL/kg/h for ⩾6 h; stage 2, 2.0–2.9 times increase in sCr level from baseline or urine output <0.5 mL/kg/h for ⩾12 h; and stage 3, 3.0 times or ⩾4.0-mg/dL increase in sCr level from baseline, urine output <0.3 mL/kg/h for ⩾24 h, or newly started renal replacement therapy. In our hospital, most patients leave the intensive care unit (ICU) within 24 h, and hourly urine volume measurements are not conducted in the general wards. We therefore modified the KDIGO criterion for stage 3 as a decrease in urine output <0.3 mL/kg/h over 12 h. The baseline sCr was defined as the most recent preoperative measurement. Urine output was evaluated using hourly urine output recorded only in the ICU for up to 7 days postoperatively. If the patient was transferred from the ICU to the general ward within 7 days postoperatively or if the urine output was no longer recorded, the urine output was considered normal from that point onward. 16
Exposures
The two authors (TS and TN) determined the thresholds for each exposure variable (MAP, pump flow rate, and Hb) with reference to values commonly used in clinical guidelines, previous studies, and clinical experience.12,13 Specifically, MAP thresholds were set at 60, 70, and 80 mmHg in 10-mmHg increments; pump flow rates at 2.4, 2.6, and 2.8 L/min/m2 in 0.2-L/min/m2 increments; and Hb levels at 8, 9, and 10 g/dL in 1-g/dL increments.
Using time-series data recorded at 1-min intervals, four indices were calculated for each exposure threshold, namely, duration, proportion, area under the threshold (AUT), and time-normalized AUT. 17 For these indices, we determined that the primary exposures were the AUTs of MAP, pump flow rates, and Hb levels. For the AUT, the cumulative products of the magnitude of variation and the duration below each threshold during CPB were calculated for each exposure factor. Furthermore, the cumulative time below the threshold (duration), the percentage of time below the threshold during CPB (proportion), and the percentage of AUT divided by CPB time (time-normalized AUT) were calculated to explore the association with CSA-AKI.
Primary analysis
Many potential confounders related to CSA-AKI exist. First, we listed the candidate explanatory variables from the literature reporting on CSA-AKI.4,18–22 Second, two authors (TS and TN) chose the variables to be included in the study based on clinical knowledge. Third, we employed logistic regression models with Lasso (least absolute shrinkage and selection operator) regularization combined with five-fold cross-validation to prevent overfitting and reduce multicollinearity. In addition, we assessed multicollinearity using the variance inflation factor (VIF) to identify the explanatory variables to be included in the final logistic regression model. The VIF was considered appropriate if it was <10. The methods for the explanatory variable selection are described in Supplemental eAppendix 1. We also added a calculated index for each exposure into the multivariable logistic regression models.
Sensitivity analyses
For the sensitivity analyses, multivariable logistic regression models with the selected variables were used. In our preliminary survey, 25% and 14% of the patients had stage ⩾1 and ⩾2 AKI, respectively. Assuming a sample size of 400, eight and four variables were included for the primary (stage ⩾1 AKI) and secondary (stage ⩾2 AKI) outcomes, respectively (Supplemental eAppendix 2).
CPB Management
For CPB priming, bicarbonate Ringer’s solution, D-mannitol, hydroxyethyl starch solution, heparin sodium, and sodium bicarbonate were used. We used a centrifugal pump for blood pumping. During CPB, the patients were controlled for mild hypothermia (32°C–34°C). CPB management for each exposure factor in our hospital was as follows: MAP was adjusted to 50–80 mmHg using phenylephrine, noradrenaline, or nicardipine in consultation with the attending anesthesiologists. The pump flow rate was adjusted within the range of 2.0–3.0 L/min/m2 by monitoring the MAP, central venous pressure, mixed venous blood oxygen saturation (SvO2), tissue oxygenation index (NIRO-200NX, Hamamatsu Photonics K.K., Hamamatsu, Japan) attached to the patient’s forehead, and urine volume. During CPB, the Hb level was maintained at ⩾7.0 g/dL so as not to decrease tissue oxygenation and SvO2. Red blood cell (RBC) was transfused at the end of CPB to maintain the Hb level at ⩾10 g/dL. During the study period, there were no changes in the CPB management, including the CPB circuit, priming fluid, and blood pump.
Data source
Patient background, preoperative medication history, blood test results, and blood gas data were obtained from the electronic medical records of Nagoya City University Hospital. Data on intraoperative time-series MAP, pump flow rates, and Hb levels were extracted by two authors (TS and TN) from an anesthesia information management system (ORSYS, Koninklijke Philips N.V., Amsterdam, Netherlands). The postoperative urine volume in the ICU was obtained from a critical and acute patient information system (ACSYS, Koninklijke Philips N.V., Amsterdam, the Netherlands).
Preprocessing of intraoperative data
Cases with continuously missing time-series data for exposure during CPB for more than 10 min were excluded from the analysis. 17 A pump flow rate <1.5 L/min/m2 was expected at the beginning or end of CPB and was therefore considered to be inappropriate for the study objective, which was to investigate optimal management goals during CPB. Thus, only the period during CPB when the pump flow rate was ⩾1.5 L/min/m2 was analyzed.
Statistical analysis
The presence or absence of CSA-AKI was determined according to a prespecified statistical analysis plan. Data for continuous and categorical variables were expressed as median (interquartile range) and number (proportion), respectively. Patient backgrounds stratified with or without CSA-AKI were reported with standardized mean differences. The primary exposures (AUTs of MAP, pump flow rates, and Hb levels) between patients with or without CSA-AKI were compared using the Mann–Whitney U test. Univariate and multivariable logistic regression analyses were conducted to estimate the unadjusted odds ratios and adjusted odds ratios (aORs), along with their 95% confidence intervals (CIs). The R software (ver 4.4.0) was used for statistical analysis, and a p value <0.05 was considered to be statistically significant.
Results
Of the 686 eligible patients, those with nonstandard CPB management, preoperative renal failure, and missing data were excluded. Finally, 333 patients were included in the analysis (Figure 1). Among the cohort, 156 patients (46.8%) developed CSA-AKI within 7 days postoperatively, of whom 76 (22.8%) and 23 (6.9%) had stage ⩾2 and stage 3 AKI according to the KDIGO criteria and 7 (2.1%) required renal replacement therapy.
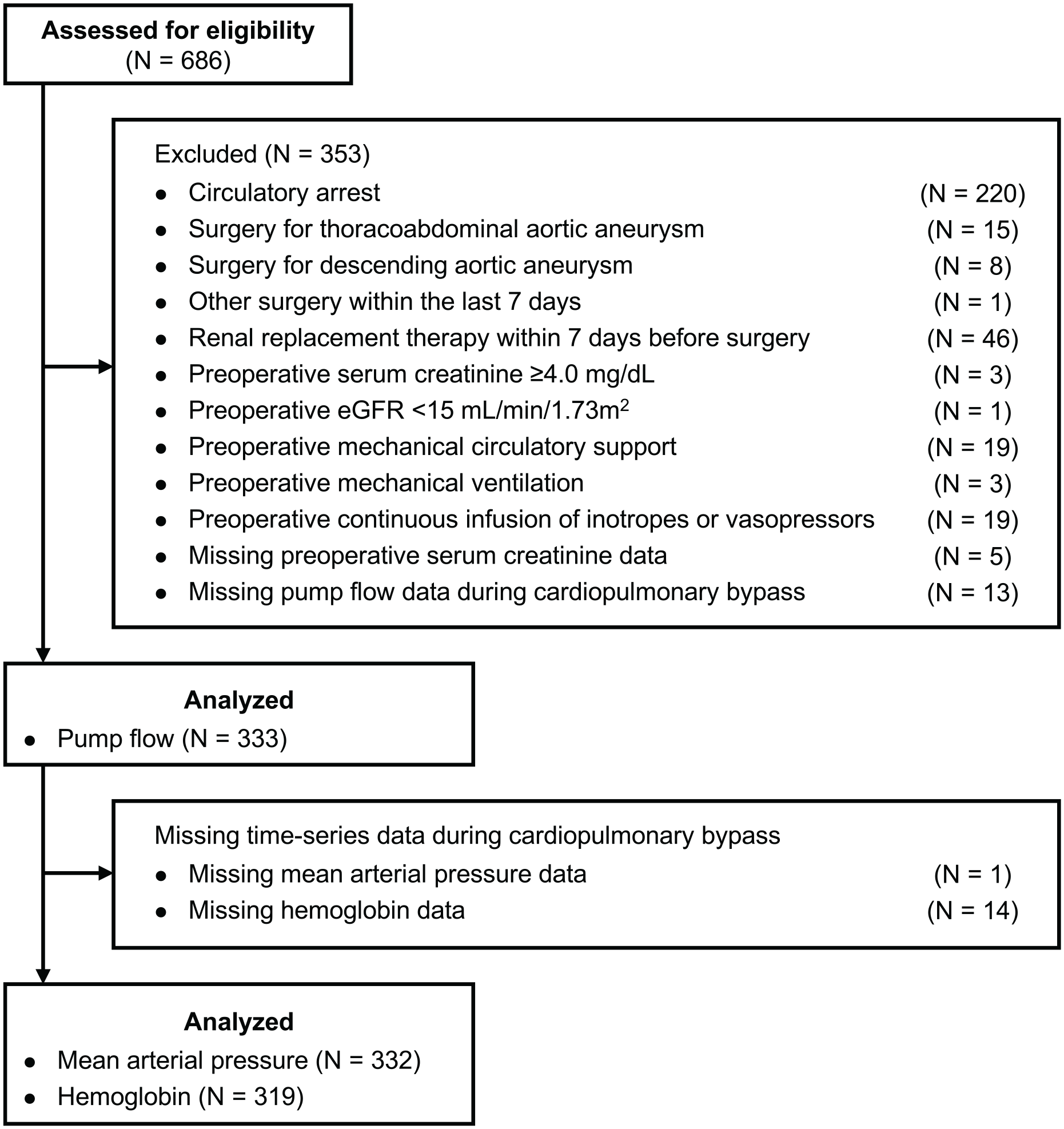
Study flow chart.
Table 1 presents the background and characteristics of patients who developed CSA-AKI and those who did not. The former group were older, had a higher body mass index (BMI), had lower preoperative Hb level and renal function, had longer surgical time, and received more blood transfusions during CPB. There were no significant differences in the AUTs of the MAP and pump flow rates between the two patient groups; however, patients who developed CSA-AKI had greater AUT of Hb (Table 2).
Patients’ background and intraoperative characteristics.
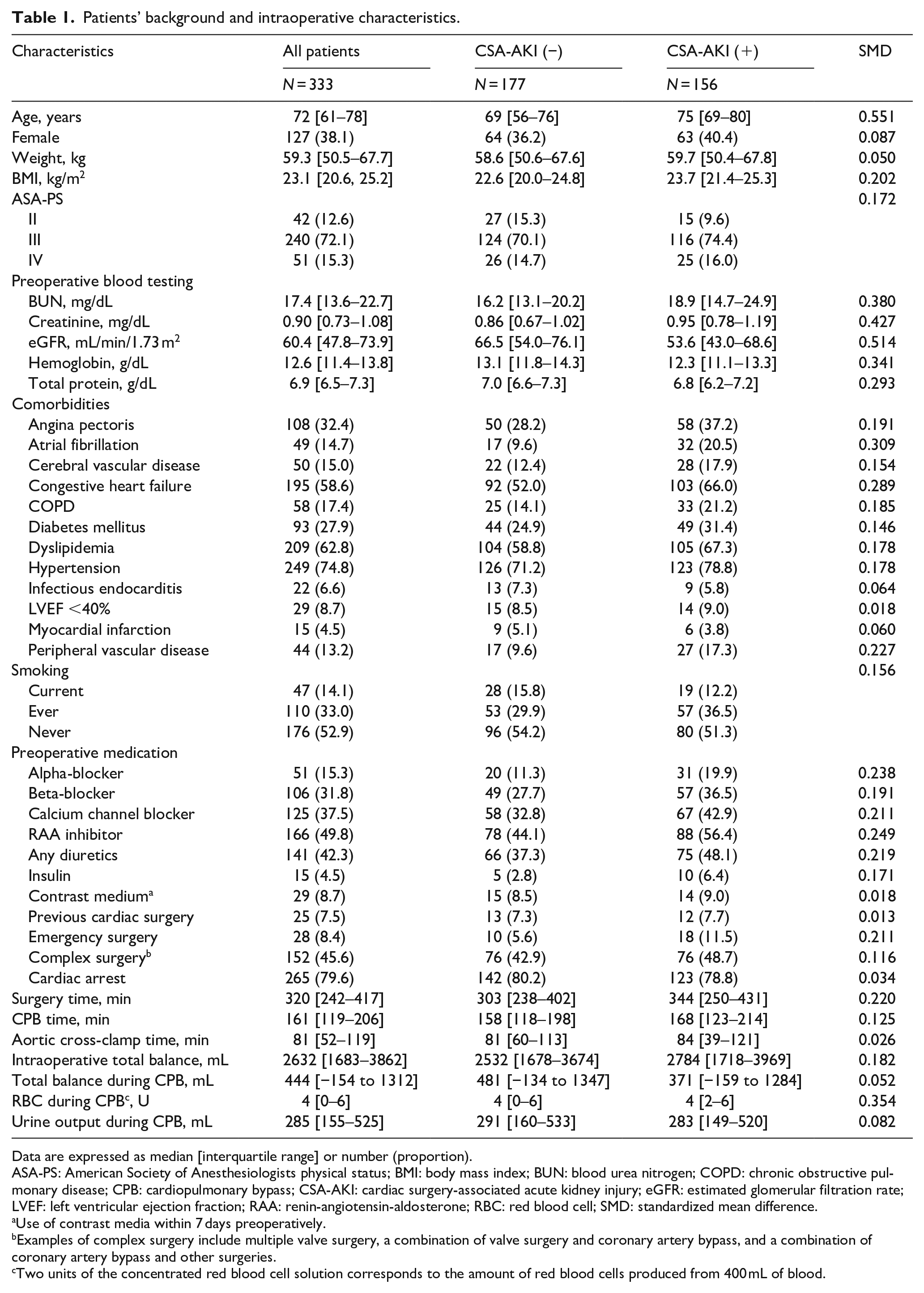
Data are expressed as median [interquartile range] or number (proportion).
ASA-PS: American Society of Anesthesiologists physical status; BMI: body mass index; BUN: blood urea nitrogen; COPD: chronic obstructive pulmonary disease; CPB: cardiopulmonary bypass; CSA-AKI: cardiac surgery-associated acute kidney injury; eGFR: estimated glomerular filtration rate; LVEF: left ventricular ejection fraction; RAA: renin-angiotensin-aldosterone; RBC: red blood cell; SMD: standardized mean difference.
Use of contrast media within 7 days preoperatively.
Examples of complex surgery include multiple valve surgery, a combination of valve surgery and coronary artery bypass, and a combination of coronary artery bypass and other surgeries.
Two units of the concentrated red blood cell solution corresponds to the amount of red blood cells produced from 400 mL of blood.
Comparison of the area under the threshold for mean arterial pressure, pump flow rates, and hemoglobin by cardiac surgery-associated acute kidney injury status.
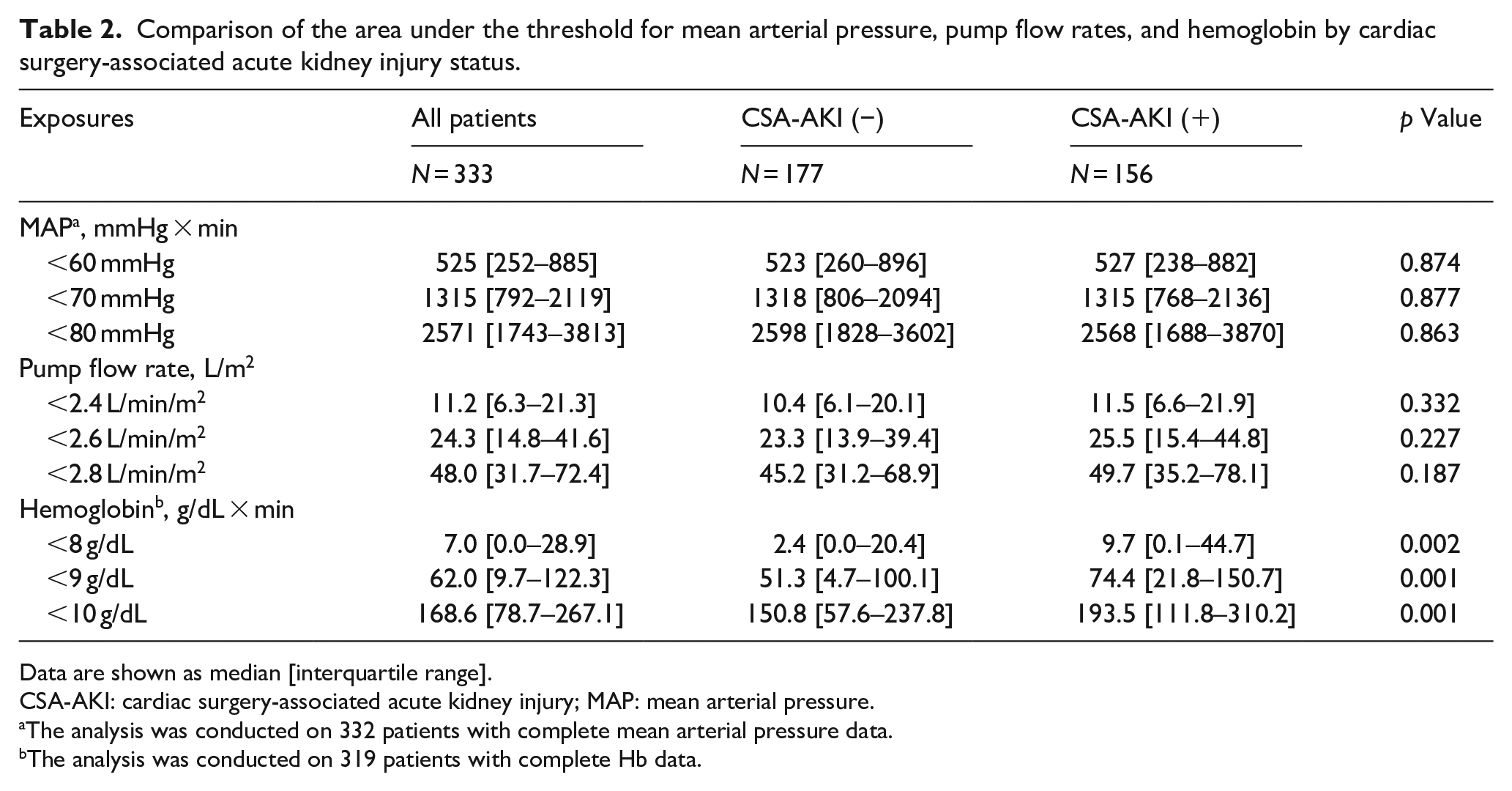
Data are shown as median [interquartile range].
CSA-AKI: cardiac surgery-associated acute kidney injury; MAP: mean arterial pressure.
The analysis was conducted on 332 patients with complete mean arterial pressure data.
The analysis was conducted on 319 patients with complete Hb data.
The explanatory variables selected via Lasso regression were age, BMI, emergency surgery, preoperative atrial fibrillation (Af), preoperative sCr, preoperative total protein, preoperative alpha-blocker medication, and number of RBC transfusion units during CPB (Supplemental eAppendix 1 and Supplemental Figure 1). Table 3 presents the association between AUT for each exposure and CSA-AKI. The AUTs of MAP and pump flow rates were not associated with CSA-AKI. Conversely, the AUT of Hb was associated with CSA-AKI, where lower thresholds were associated with higher aORs for CSA-AKI.
Association between acute kidney injury and area under the threshold for low mean arterial pressure, pump flow rates, and hemoglobin during cardiopulmonary bypass.
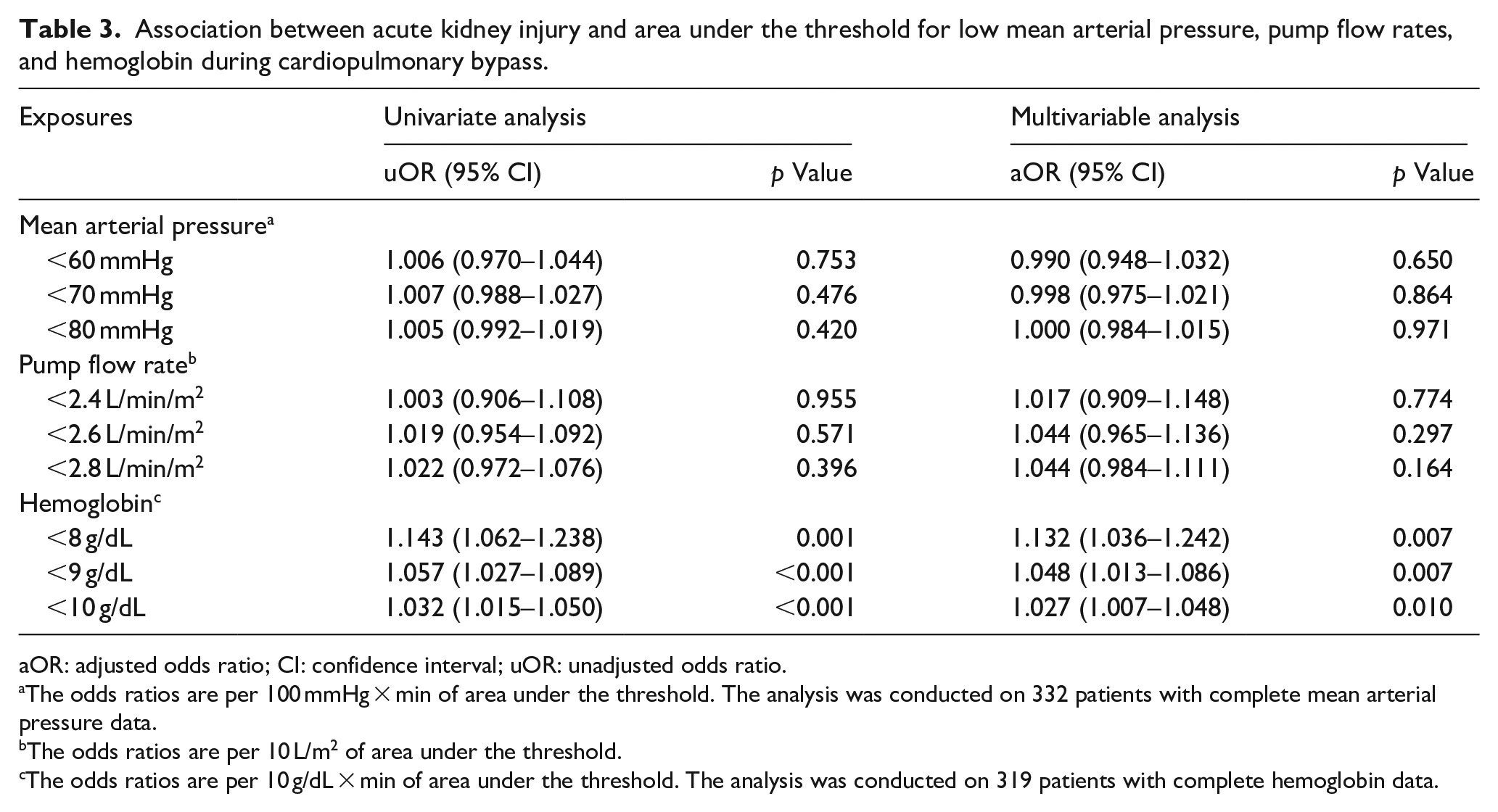
aOR: adjusted odds ratio; CI: confidence interval; uOR: unadjusted odds ratio.
The odds ratios are per 100 mmHg × min of area under the threshold. The analysis was conducted on 332 patients with complete mean arterial pressure data.
The odds ratios are per 10 L/m2 of area under the threshold.
The odds ratios are per 10 g/dL × min of area under the threshold. The analysis was conducted on 319 patients with complete hemoglobin data.
Supplemental Tables 1–3 present the results of analyses using the other indices, including duration, proportion, and time-normalized AUT of each exposure. MAP did not show an association with CSA-AKI at any threshold across all analyses. In this exploratory analysis, the duration of low Hb as well as the duration and proportion of pump flow rate <2.4 L/min/m2 was associated with CSA-AKI (Supplemental Tables 1 and 2). Furthermore, sensitivity analysis using clinically determined variables revealed that MAP and pump flow rates were not associated with CSA-AKI; conversely, Hb showed an association with CSA-AKI (Supplemental Table 4).
Supplemental Table 5 presents the characteristics of patients with and without stage ⩾2 AKI. In the multivariable logistic regression analyses, low MAP, pump flow rates, and Hb levels during CPB did not show an association with stage ⩾2 CSA-AKI (Table 4).
Association between stage ⩾2 acute kidney injury and area under the threshold for low mean arterial pressure, pump flow rates, and hemoglobin during cardiopulmonary bypass.
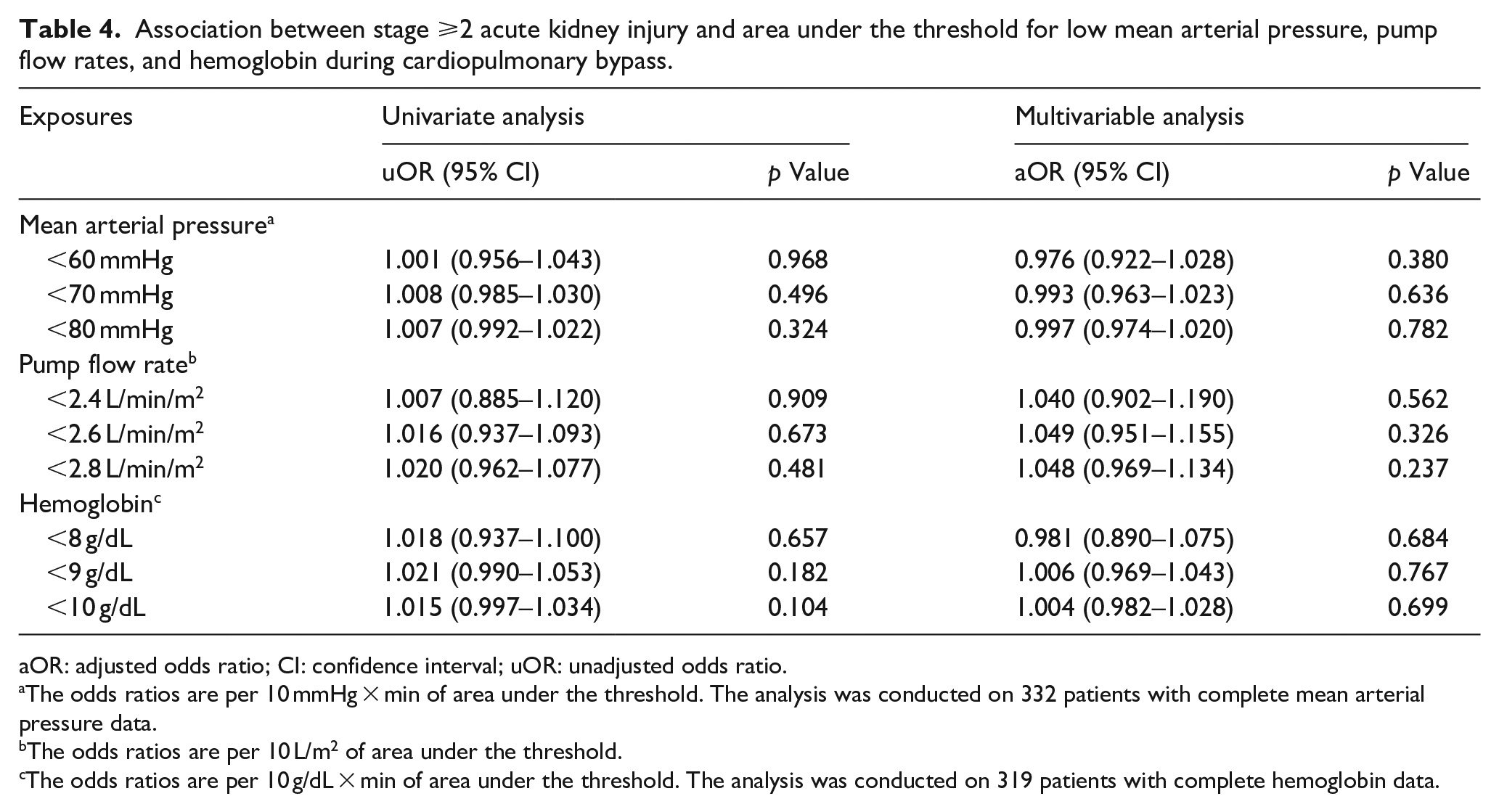
aOR: adjusted odds ratio; CI: confidence interval; uOR: unadjusted odds ratio.
The odds ratios are per 10 mmHg × min of area under the threshold. The analysis was conducted on 332 patients with complete mean arterial pressure data.
The odds ratios are per 10 L/m2 of area under the threshold.
The odds ratios are per 10 g/dL × min of area under the threshold. The analysis was conducted on 319 patients with complete hemoglobin data.
Discussion
This study investigated the exposure below various thresholds of MAP, pump flow rates, and Hb levels during CPB to explore the optimal management goals for CSA-AKI prevention. Lower Hb levels during CPB were found to be associated with CSA-AKI; the lower the threshold, the stronger the association. Contrarily, MAP and pump flow rates during CPB did not show an association with CSA-AKI.
In our study, no association was found between MAP and the development of CSA-AKI. A previous meta-analysis and two large-scale retrospective studies revealed that low MAP was associated with CSA-AKI outside of CPB, but not during CPB.23–25 In addition, clinical guidelines have noted that a high blood pressure target during CPB may have little to no effect on patient outcomes such as CSA-AKI and mortality, and that further research is warranted. 26 Consistent with these findings, low MAP during CPB was not associated with CSA-AKI in our cohort. Our results do not support the management goal of maintaining MAP ⩾60 mmHg during CPB for the prevention of CSA-AKI.
Furthermore, the study found no association between pump flow rates and CSA-AKI development when examining the threshold range of 2.4–2.8 L/min/m2. However, the exploratory analyses revealed that the longer duration and proportion of pump flow rates below the 2.4 L/min/m2 threshold were associated with increased risk of CSA-AKI (Supplemental Tables 1 and 2). A previous study that compared pump flow rates >2.2 L/min/m2 versus >2.4 L/min/m2 during CPB reported a lower incidence of the composite of death, renal replacement therapy, and persistent renal dysfunction at postoperative day 30 when the pump flow rate was managed at >2.4 L/min/m2. 27 As the increased duration or proportion of pump flow rate below 2.4 L/min/m2 was associated with CSA-AKI in our study, a pump flow rate of <2.4 L/min/m2 may have been associated with CSA-AKI. Our findings do not support the management goal of maintaining a pump flow rate target of 2.4 L/min/m2 or higher to prevent CSA-AKI.
Our study showed a significant association between lower Hb thresholds and CSA-AKI risk. However, this association disappeared in the secondary outcome, which was limited to stage ⩾2 AKI. In a previous study, the risk of CSA-AKI increased by 25%–30% when the Hb levels dropped below 8 g/dL during CPB. 9 Our study also observed an increase in CSA-AKI risk when the Hb levels fell below 8 g/dL. RBC transfusions are used to maintain Hb levels during CPB; however, they are reportedly a risk factor for CSA-AKI. 28 We included the number of RBC units administered during CPB in our multivariable logistic regression models as an explanatory variable. This approach allowed for the evaluation of the independent relationship between low Hb levels and CSA-AKI risk, separate from the influence of RBC transfusion volume. Our findings suggest that maintaining Hb levels ⩾8 g/dL during CPB may prevent CSA-AKI. However, further studies are warranted to confirm this effect, particularly on stage ⩾2 CSA-AKI.
During CPB, DO2 is a critical parameter for assessing oxygen supply to prevent ischemia in the patient’s organs and tissues. DO2 is primarily the product of Hb levels and pump flow rates corresponding to cardiac output. Goal-directed perfusion based on DO2 has been recommended in clinical guidelines to reduce the incidence of early-stage CSA-AKI. 13 We did not include DO2 in our analysis for two reasons. First, there is a gap between daily clinical practice and the guidelines’ recommendation based on DO2, as surgeons and anesthesiologists typically rely on more direct and intuitive parameters such as MAP, pump flow rates, and Hb levels. Second, DO2 is a composite variable derived from multiple components, making it difficult to isolate the independent effects of each factor. Therefore, we focused on evaluating individual, routinely monitored variables to better reflect clinical decision making in daily practice.
In the present study, the incidence of CSA-AKI within 7 days postoperatively was 46.8%. As CSA-AKI reportedly occurred in 5%–43% of cases, 2 its incidence was relatively high. A possible explanation for this was that we used the KDIGO criteria with urine criteria to define the CSA-AKI. Studies using this combination reported higher incidence of AKI than those that did not use the urine criteria.29,30 Thus, the incidence of CSA-AKI in our study was higher than in previous ones that used the Risk, Injury, Failure, Loss, End-stage (RIFLE) classification (23.5%–30.0%), or the KDIGO criteria without urine criteria (38.5%–41.4%).11,18,31–33
The strengths of our study were as follows: First, we used a high-quality dataset with minute-by-minute recorded vital signs and CPB parameters during CPB. Second, we comprehensively identified the risk factors for CSA-AKI and performed variable selection via Lasso regression. Our final model included preoperative Af and alpha-blocker medication selected via Lasso regression and well-known risk factors, such as age, emergency surgery, preoperative sCr, and number of RBC units. Nevertheless, the association between preoperative Af and CSA-AKI needs to be examined in the future. Third, we used the KDIGO criteria that included urine output in the ICU, which allowed for the detection of CSA-AKI with high sensitivity. Finally, we confirmed the association between low Hb levels during CPB and CSA-AKI in the sensitivity analysis, which is similar to the primary analysis. It can support the robustness of the primary results.
This study also has several limitations that need to be acknowledged. First, it is a retrospective, single-center study, and the small sample size may limit statistical power. The association between stage ⩾2 CSA-AKI and low pump flow rates may not have been detected owing to the small number of patients with stage ⩾2 CSA-AKI. Future multicenter studies involving a larger sample size are warranted. Second, as our study was exploratory in nature, no adjustment for multiple comparisons was performed. Therefore, the results should be interpreted with caution, and further confirmatory studies with appropriate correction for multiple testing are warranted. Third, we used urine volume data only during ICU admission as it was not frequently measured after discharge from the ICU. Finally, we excluded cases in which the CPB management differed from standard CPB techniques, such as circulatory arrest. Therefore, the results of our study are only applicable to cases managed with standard CPB techniques.
Conclusions
Hb levels during CPB below 8.0 g/dL were associated with CSA-AKI, while MAP and pump flow rates indicated no such association. Our results indicated that the lower the Hb levels, the stronger the association, suggesting the need for future studies evaluating the efficacy of maintaining Hb ⩾8.0 g/dL during CPB for CSA-AKI prevention.
Supplemental Material
sj-pdf-1-jao-10.1177_03913988251365814 – Supplemental material for Association of exposure below various thresholds of hemodynamic parameters during cardiopulmonary bypass with acute kidney injury
Supplemental material, sj-pdf-1-jao-10.1177_03913988251365814 for Association of exposure below various thresholds of hemodynamic parameters during cardiopulmonary bypass with acute kidney injury by Takumi Sasaki, Toshiyuki Nakanishi, Tatsuya Tsuji, Eisuke Kako, Tetsuya Tamura, Koichi Fujiwara, Miho Murashima, Takayuki Hamano and Kazuya Sobue in The International Journal of Artificial Organs
Footnotes
Author contributions
TS contributed to the study conceptualization, study design, data acquisition, data analysis, data interpretation, and manuscript drafting. TN contributed to the study conceptualization, study design, data acquisition, data analysis, data interpretation, funding acquisition, supervision, and drafting, reviewing, and revising the manuscript. TTsuji, EK, TTamura, KF, MM, TH, and KS contributed to the study design, data interpretation, and reviewing and revising the manuscript.
Data availability statement
The data of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by JSPS KAKENHI (24K19467) and the Nitto Foundation (JOSE205112).
Ethical considerations
The study was approved by the Nagoya City University Graduate School of Medical Sciences and the Nagoya City University Hospital Institutional Review Board (60-23-0125, January 9, 2024).
Consent to participate
The Nagoya City University Graduate School of Medical Sciences and the Nagoya City University Hospital Institutional Review Board have waived informed consent to participate. Eligible participants were given the opportunity to opt out of the study on the website of the Nagoya City University Hospital Clinical Research Management Center (![]() ).
).
Consent for publication
Not applicable.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.