
Abstract
Background:
The ideal dialysate potassium concentration for patients with hyperkalemia undergoing maintenance hemodialysis is debated. While low-potassium dialysate enhances potassium removal, a steep serum-todialysate potassium gradient may provoke arrhythmias. This study aimed to assess the efficacy of a two-phase dialysate potassium profiling strategy.
Materials and methods:
Patients aged 18–60 years with end-stage renal disease and predialysis hyperkalemia were randomized into two groups for twice-weekly hemodialysis. Group A received 2 mEq/L potassium dialysate for the first hour, followed by 0 mEq/L for the next 3 h. Group B received a constant 2 mEq/L potassium dialysate throughout the 4-h session. Serum potassium was measured pre-dialysis and hourly during the session. Patients were monitored for cardiac arrhythmias.
Results:
Of 145 patients screened, 60 were enrolled (30 per group). The majority were male (66.7% in Group A and 56.7% in Group B), with over 50% having diabetes and 85% hypertension, indicating high cardiovascular risk. Predialysis potassium levels were similar (6.00 ± 0.3 mEq/L in Group A vs 5.98 ± 0.34 mEq/L in Group B). Group A achieved significantly lower post-dialysis potassium levels (3.48 ± 0.22 mEq/L) than Group B (3.72 ± 0.42 mEq/L; p = 0.008). One case of ventricular ectopy was observed in each group, both managed conservatively.
Conclusion:
Two-phase dialysate potassium profiling effectively lowers serum potassium more than a fixed approach, without a significant increase in arrhythmic events, supporting its use in managing hyperkalemia in hemodialysis patients.
Keywords
Introduction
Hemodialysis patients often experience hyperkalemia, which increases the risk of arrhythmias and sudden cardiac death. Common management strategies include dietary restrictions, medication adjustments, diuretics, potassium binders, and dialysate potassium modulation. 1 However, diuretics are less effective with minimal residual renal function, and potassium binders have limited accessibility or tolerability.
One feasible approach to managing hyperkalemia is the use of low potassium dialysate. However, this strategy presents its challenges, such as accurately targeting the desired potassium gradient and the logistical need to source different dialysate formulations. Despite these difficulties, employing low potassium dialysate remains a practical option for addressing hyperkalemia in hemodialysis patients. The speed at which hyperkalemia is corrected during dialysis with low potassium dialysate has been linked to an increased risk of arrhythmias and sudden cardiac deaths. 2 The “rule of seven” suggests that the sum of serum and dialysate potassium should equal 7 to minimize the potassium gradient and reduce risk. 3
To address the challenge of balancing effective potassium removal with safety, this study tested a two-phase profiling approach: using 2 mEq/L dialysate potassium for the first hour, followed by 0 mEq/L for the next 3 h. This method was compared to the conventional use of a constant 2 mEq/L over 4 h, aiming to provide gradual potassium reduction while minimizing arrhythmia risk.
Materials and methods
This open-label, double-arm, randomized controlled study was conducted in the in-center hemodialysis unit of a tertiary care teaching hospital in northern India. The experimental protocol was approved by the ethical committee (IEC no. 80/18) and this clinical trial was registered before patient enrolment (CTRI/2019/08/020677). Subjects were randomized to enter into either of the two arms. In the first arm (Group A, Profiled dialysate arm), the dialysate bath contained 2 mEq/L potassium in the first hour and 0 mEq/L in the next 3 h. The second arm (Group B, fixed dialysate arm) received a dialysate of 2 mEq/L potassium during the full 4-h dialysis session. Participants were randomly assigned to either arm with a 1:1 allocation as per a computer-generated block randomization schedule using a block size of 10. The bicarbonate-based dialysate bath comprising 3.26 mEq/L of magnesium, 136 mEq/L of sodium, 3 mEq/L of calcium, and 200 mg/dL of glucose was the same for all patients. All patients were dialyzed using polysulfone dialyzers ranging in size from 1.2 to 1.5 m2. Blood flow was maintained at 300 mL/min and dialysate flow was kept at 500 ml/min in all patients for the full 4-h dialysis session in both groups. A bicarbonate concentration of 35 mEq/L was kept in the dialysate fluid. All basic laboratory values were derived from the predialysis (just before the initiation of dialysis) blood samples on the day of intervention. The pre-dialysis serum potassium levels were measured with a three-day interval following the previous dialysis session. Subsequently, the next pre-dialysis potassium level was assessed after a two-day gap prior to the subsequent dialysis session. Each patient participated in one monitored dialysis session as per the study protocol.
Serum potassium was measured pre-dialysis, after first, second, third hour of dialysis, and 15 min after the end of dialysis. A pre-dialysis blood sample for measuring serum potassium was also taken in the subsequent dialysis session. A cardiac monitor was used during the full course of dialysis until 3 h post-dialysis. When detecting any ectopic/arrhythmia in the monitor, a 12-lead ECG was printed and sent for a cardiac consultation. ECGs were interpreted by an independent cardiologist blinded to the group assignments. It was planned to shift patients to a dialysate bath of 3 mEq/L on detection of serum potassium of ⩽3 mEq/L during dialysis.
Inclusion criteria
End Stage Renal Disease (ESRD) patients in the age group between 18 and 60 years on twice-a-week maintenance hemodialysis receiving 4-h dialysis sessions giving written consent to participate in the study.
ESRD patients on hemodialysis for 6 months or more with predialysis serum potassium consecutively recorded ⩾5.5 mEq/L during last 3 months.
Exclusion criteria
Any previous history of congestive heart failure and arrhythmia.
Patients with serum potassium ⩾7 mEq/L before dialysis and interdialytic weight gain ⩾4 kgs.
Patients on digitalis and pregnancy.
Statistics
Sample size estimation: Assuming mean ± SD of the paired differences (between baseline and at the end of 4 h dialysis session) of Group A and Group B are 2.5 ± 0.2 and 2.0 ± 0.5, 4 at minimum two-sided 95% confidence interval and 80% power of the test, the calculated sample size for each of the two groups was 26 (total 52).
Analyses were performed using SPSS version 20.0 (SPSS, Chicago, IL, USA). We used descriptive statistics (mean ± standard deviation (SD)) for continuous variables. An Independent t-test was used to compare continuous variables. Chi-square was used to compare categorical variables between the two groups. Repeated measures ANOVA was used to compare variables at different time points. A two-sided p < 0.05 was considered statistically significant.
Results
Among 145 patients screened from those visiting the department’s OPD, 60 were finally included in the study, and 30 were randomized to either of the treatment arms Figure 1. Both arms were predominantly comprised of males (66.67% in Group A and 56.67% in Group B, respectively). Type 2 Diabetes Mellitus was present in over half of the study subjects in both groups. Participants had suboptimal hemoglobin levels in both groups (9.38 ± 1.45 in Group A and 10.02 ± 0.78 in Group B). The two groups were similar in both demographic and biochemical characteristics (Table 1).
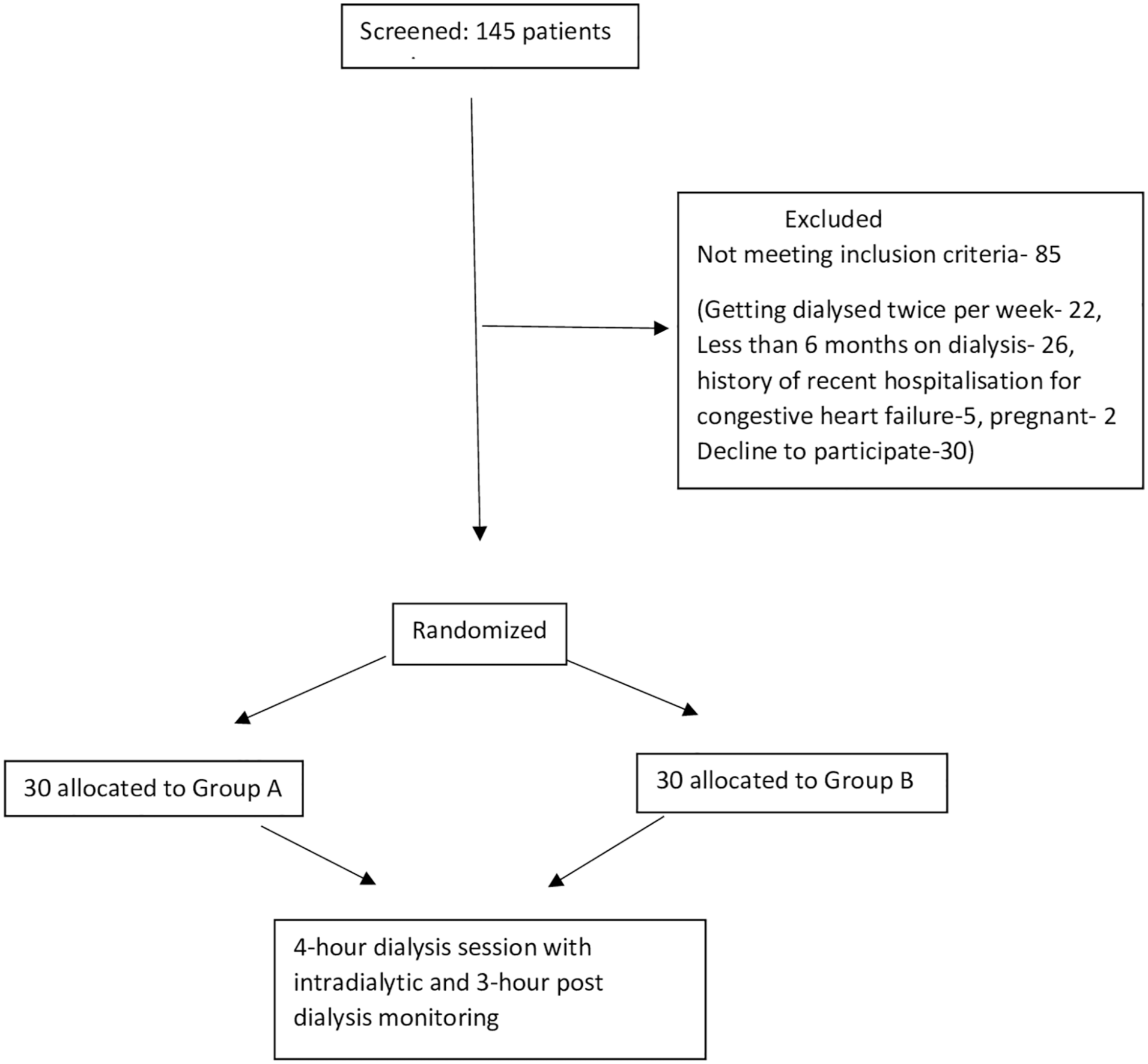
Flow diagram of the RCT.
Demographic and laboratory features of the experimental arms.
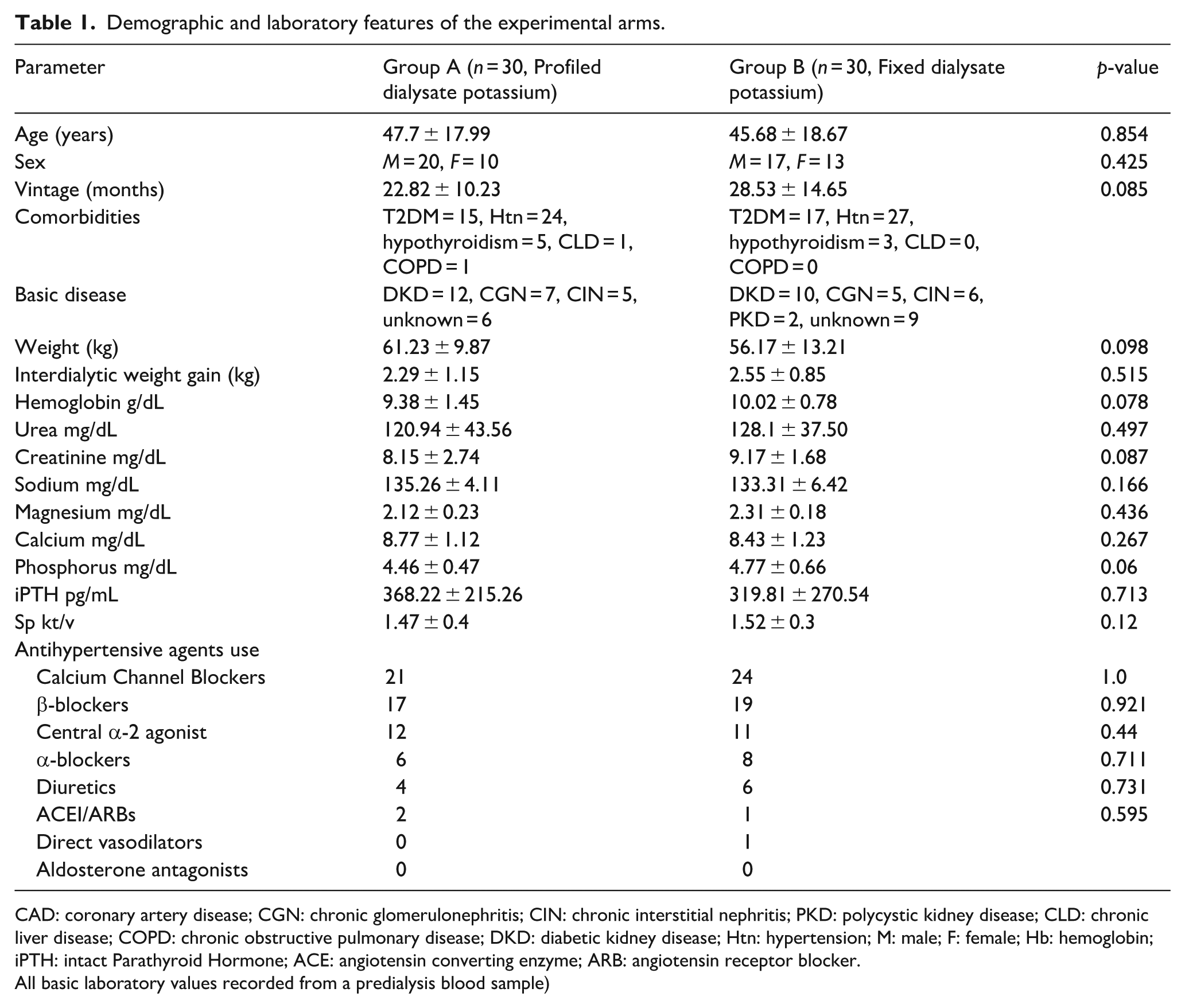
CAD: coronary artery disease; CGN: chronic glomerulonephritis; CIN: chronic interstitial nephritis; PKD: polycystic kidney disease; CLD: chronic liver disease; COPD: chronic obstructive pulmonary disease; DKD: diabetic kidney disease; Htn: hypertension; M: male; F: female; Hb: hemoglobin; iPTH: intact Parathyroid Hormone; ACE: angiotensin converting enzyme; ARB: angiotensin receptor blocker.
All basic laboratory values recorded from a predialysis blood sample)
Serum potassium
The predialysis mean serum potassium levels were 6.00 ± 0.3 and 5.98 ± 0.34 mEq/L in Groups A and B, respectively (Table 2). After that, the fall in serum potassium levels in the first hour was similar in both the groups in concordance with an equal dialysate potassium bath being used. In the first hour of dialysis, the fall in serum potassium levels were 0.81 and 0.76 mEq/L in Group A and Group B, respectively. However, at the end of the second hour, the fall in serum potassium level was greater in Group A (0.91 mEq/L) on changing the dialysate potassium bath to 0 mEq/L compared to 0.54 mEq/L in Group B with a dialysate bath of 2 mEq/L of potassium. In the next 2 h, serum potassium kept falling in both groups at a slower rate. The lines depicting a graphical trend of fall in serum potassium levels began to separate from the second hour onwards with the introduction of 0 mEq/L potassium dialysate bath in group A (Figure 2). A repeated measure ANOVA with a Greenhouse-Geisser correction showed that mean potassium differed significantly between time points in both groups (p = 0.03). The serum potassium levels at various time points viz. second hour, third hour, and end of dialysis in the two groups were significantly different (p = 0.004, 0.012, and 0.001, respectively). The mean serum potassium levels achieved at the end of dialysis were 3.48 ± 0.22 and 3.72 ± 0.42 mEq/L in Groups A and B, respectively (p = 0.008). The effect of lowering potassium levels persisted to the next dialysis session, with pre-dialysis serum potassium levels recorded lower in the profiled dialysate group (Group A—5.26 ± 0.32 mEq/L) compared to the fixed dialysate potassium group (Group B—5.52 ± 0.27 mEq/L) which was also significant (p = 0.0012).
Serum potassium at specific time intervals (all sessions of 4 h each).
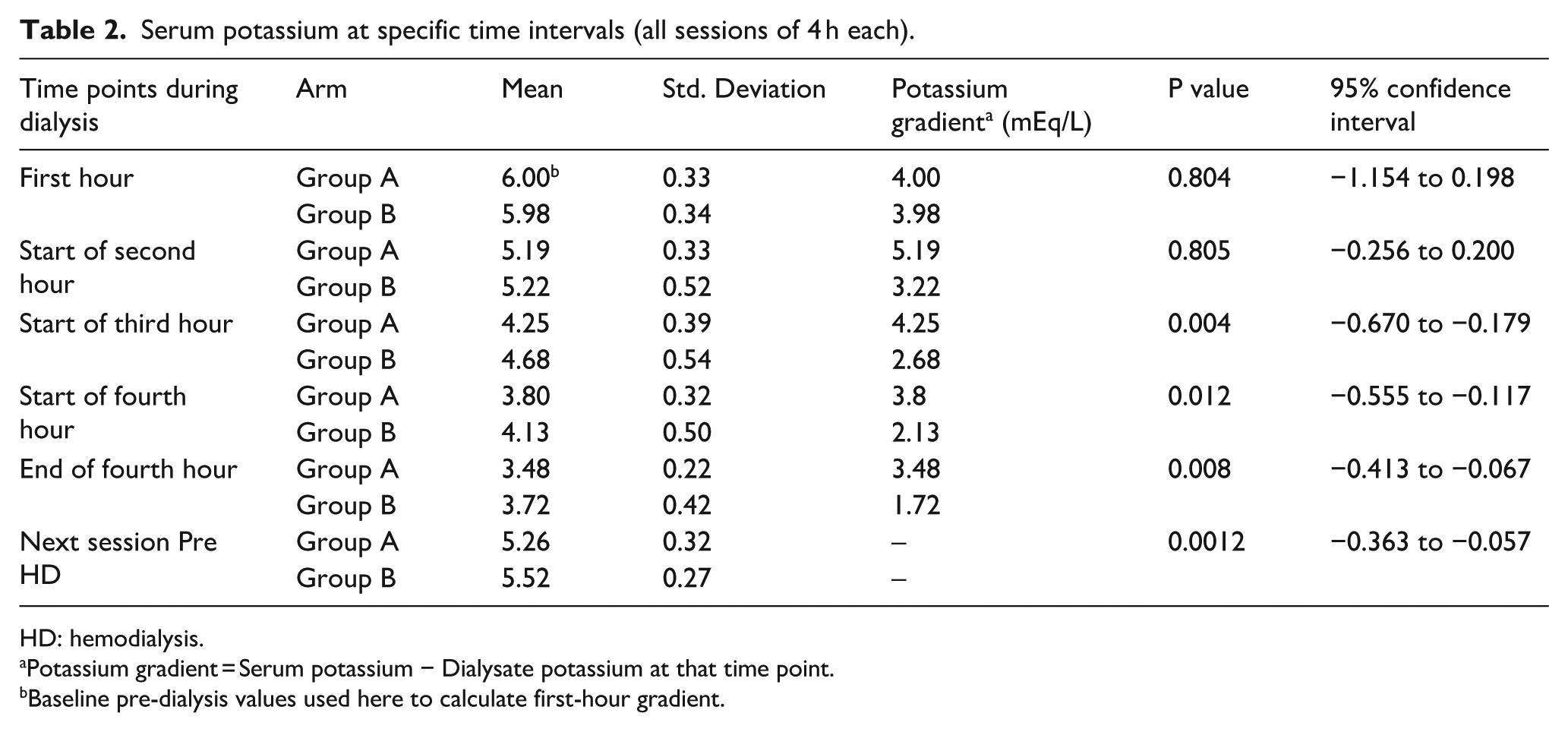
HD: hemodialysis.
Potassium gradient = Serum potassium − Dialysate potassium at that time point.
Baseline pre-dialysis values used here to calculate first-hour gradient.
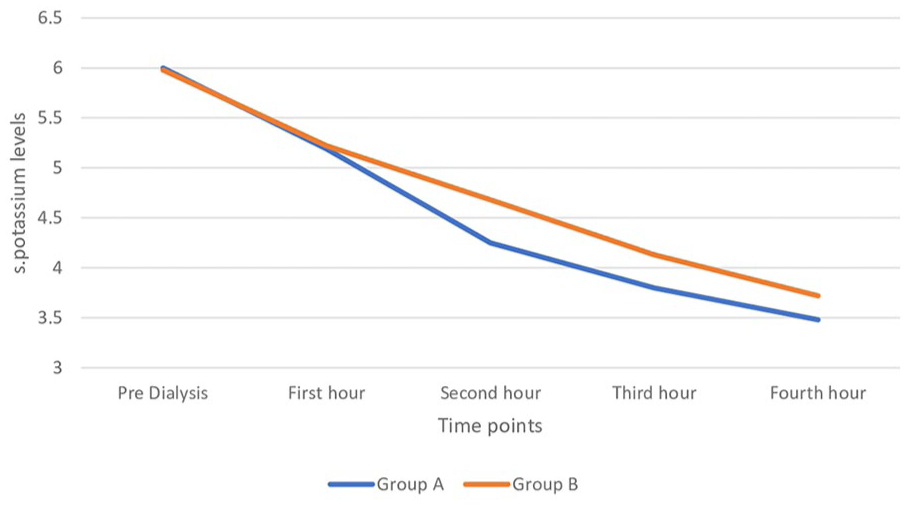
Serum potassium concentration at various time points.
Adverse events
One patient from group A and one patient in group B recorded ventricular ectopics. In Group A they were seen in the second and third hour of dialysis, respectively, whereas in Group B it was seen in the fourth hour of dialysis; the frequency in all was less than two ectopics per 6-s recording strip. All patients were managed conservatively with resolution within 2 h of the end of dialysis. A potassium level of less than 3 mEq/L was recorded in one patient at the end of the dialysis session in Group A, who was asymptomatic with a normal ECG and didn’t require any intervention. All other ECG parameters were found to be within the normal range.
Discussion
With diffusion accounting for a majority of potassium removal in conventional dialysis, the rate and total amount removed from the body depend on the gradient between blood and dialysate fluid. High potassium gradient during dialysis has been linked to higher rates of cardiovascular hospitalizations. 5 Singh et al. 6 in their study reported lower mortality in end-stage renal disease patients with hyperkalemia (>6.5 mEq/L) using dialysate potassium of 1 mEq/L. By implementing dialysate potassium profiling, which involves transitioning from high to low potassium concentrations, it is possible to reduce the steep potassium gradient typically observed in the initial hour of dialysis when using low potassium baths from the beginning. 7 Our analysis shows that although potassium gradients were similar in the first hour, the gradient was higher in the profiling arm during the second and third hours of dialysis. This finding reflects the protocol design, in which the dialysate potassium was reduced to 0 mEq/L after the first hour. The higher mid-session gradient could theoretically increase arrhythmia risk in this phase of dialysis. However, in our study, no clinically significant arrhythmias were observed, and only isolated ventricular ectopics occurred in one patient from each arm. The potential trade-off between achieving a lower end-of-dialysis serum potassium and exposure to higher mid-session gradients warrants further research. This study represents a novel approach to exploring the potential benefits of targeting a lower serum potassium level at the conclusion of dialysis through the use of variable dialysate potassium concentrations.
In our study population, more than 50% of the subjects were diabetics, while hypertension was present in 85% of cases, putting them in a high cardiovascular risk category. 8 Hyperkalemia is an important modifiable risk factor for adverse cardiovascular events in this subset of patients. We were able to reduce serum potassium levels by dialysate profiling to a greater extent compared to a standard continuous 2 mEq/L dialysate bath. This is in contrast to the study by Munoz et al. 9 where no difference in post-dialysis serum potassium was reported while comparing potassium-profiled dialysate with constant potassium dialysate. The dialysate potassium concentration differed in Munoz’s study, which was 3.2–4 mmol/L at the beginning and 1–1.3 mmol/L at the end of dialysis.
The rate of fall in serum potassium levels in our study in the first hour were 0.81 and 0.76 mEq/L in different groups which is lower than the reported fall of 1 mEq/L by Pun et al. 10 This could be related to the different blood and dialysate flows used in our study. This also indicates a lower potassium gradient achieved in our study resulting in a lower incidence of arrhythmias.
While some have reported a direct relationship with high cardiovascular events particularly arrhythmias in the initial hours of dialysis using low potassium dialysate 11 others reported better survival with low potassium dialysate in cases of hyperkalemia as compared to high dialysate potassium concentration. 12 Our study results provide evidence in favor of no significant increased risk of arrhythmias with the use of potassium profiling in patients with serum potassium levels between 5.5 and 7 mEq/L. However, the current study was not powered to confirm the safety of dialysate profiling. There is an increased risk of sudden cardiac death in the long gap period between two dialysis sessions. In cases of persistent predialysis hyperkalemia, achieving a lower serum potassium concentration at the end of each dialysis might help prevent cardiac deaths occurring due to hyperkalemia in the interdialytic period.
While low potassium dialysate baths are expected to result in arrhythmias due to abnormal membrane polarization, in the current study, one patient in the potassium profiling arm and one in the fixed potassium arm experienced ventricular ectopics with both experiencing a smooth recovery in the post-dialysis period. High use of β-blockers, 56.7% in Group A and 63.3% in Group B could have provided an additional cardioprotective effect. A similar safety profile was reported by Santoro et al. 13 while using declining potassium profiling in dialysis-sensitive arrhythmic patients.
The study provides evidence in favor of using decreasing dialysate potassium profiling in cases of predialysis hyperkalemia when targeting a lower value at the end of the dialysis session. The cardiac safety of this approach needs to be studied further for wider application.
Limitations
The sample size taken for the study was small. A longer post-dialysis monitoring period with added information about the recovery time of the patients could have added more value to the study. The study was not powered to check for the safety of such dialysate profiling. No data was collected on residual kidney function, although 80% of the participants were anuric, and 10% of them were passing less than 200 mL of urine in 24 h. Serum bicarbonate levels were not measured, which may have influenced the serum potassium levels of the patients.
Conclusion
In maintenance hemodialysis settings, the use of a potassium profiling strategy to target lower serum potassium values may provide protection from a high potassium gradient in the initial hours of dialysis and achieve lower potassium levels at the end of dialysis. This strategy is likely to work in those who don’t adhere to dialysis prescriptions and in Asian countries where a twice weekly dialysis schedule is commonly practiced in more than two-thirds of patients 14 and subsequently have persistent high pre-dialysis serum potassium levels. Studies with larger sample sizes and longer post-dialysis follow-up periods with cardiovascular endpoints need to be designed to establish the safety and clinical utility of targeting low potassium levels.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.