
Abstract
Background:
Cardiogenic shock (CS) secondary to acute decompensated heart failure (ADHF) is a life-threatening condition that may require the use of mechanical circulatory support (MCS). Venoarterial (VA) extracorporeal membrane oxygenation (ECMO) represents one of the first-line temporary MCS options.
Methods:
We conducted a single-center, retrospective observational cohort study of adult patients with CS secondary to ADHF that required VA ECMO at our institution from 2014 to 2023. Patients requiring extracorporeal cardiopulmonary resuscitation (ECPR) or initially placed on venovenous (VV) ECMO were excluded. Baseline characteristics, ECMO support details, and clinical outcomes were analyzed. The primary outcomes were survival to hospital discharge and at 2 years.
Results:
A total of 69 patients were included. The median age was 55 years old and 60.9% were male. All patients were cannulated peripherally, with a median duration of support of 10 days. ECMO weaning was achieved in 73.9% and 56.5% survived to hospital discharge. The 2-year survival rate was 46.3%. From the total number of patients, 36.2% were bridged to durable MCS, 16% were weaned and survived to discharge, and 13% underwent heart transplantation. The most common complications included renal replacement therapy (34.8%), bleeding (20.3%), and infection (16%). Notable complications that were associated with worse outcomes included neurologic events, bleeding complications, and renal replacement requirement.
Conclusion:
In patients with ADHF-CS, VA ECMO is a viable short-term support strategy that facilitates bridging to recovery or advanced therapies.
Introduction
Cardiogenic shock (CS) is a complex syndrome with many underlying causes and is associated with high morbidity and mortality, regardless of the etiology. 1 It is characterized by insufficient tissue and end organ perfusion due to decreased cardiac output, secondary to a primary cardiac condition.
While the majority of CS admissions are secondary to acute coronary syndrome (ACS), a significant proportion of presentations are due to other etiologies.2,3 Recent observational studies suggest that non-ischemic etiologies, such as acute decompensated heart failure-CS, account for more than half of all CS causes.4,5 Though much of the literature has focused on CS secondary to myocardial infarction, far less is known about the identification and outcomes of the non-ACS population presenting with CS, particularly in patients with acute decompensated heart failure (ADHF). 2
The management of CS and heart failure has evolved significantly over the past five decades. Despite these improvements, outcomes have not significantly improved since the landmark SHOCK trial.6,7 This lack of benefit is often attributed to the heterogeneity of the patient population, encompassing variations in shock duration at presentation, underlying etiology, comorbid conditions, and adjunctive therapies employed. 8 Despite of the advancements in temporary mechanical circulatory support (tMCS) devices 9 and the development of multidisciplinary shock teams at many institutions, mortality rates among patients presenting with CS range from 25% to 50%.10,11 Moreover, there is insufficient data reporting CS survival rates beyond hospital discharge. 12
For the most critically ill patients with CS secondary to ADHF, Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS) level 1 or 2, 13 tMCS is the only viable option to prevent death. 14 In a study that included 2722 heart failure patients with cardiogenic shock, the rate of tMCS use increased from 2010 to 2019, with percutaneous left ventricular support device (Impella® Abiomed, Danvers, MA, USA) use showing a 344% increase in use, followed by VA ECMO that displayed a 112% increase in its use. 9
Venoarterial extracorporeal membrane oxygenation (VA ECMO) represents one of the first-line tMCS options, 15 either as a bridge to transplantation, durable device, decision, or recovery to baseline. Data from Extracorporeal Life Support Organization (ELSO) shows that ECMO use as a bridge to advanced therapies (BT-Adv) has increased over time, from 1.7% in 2010 to 22.2% in 2019 while the cumulative in-hospital mortality for patients bridged with ECMO to advanced therapies remains high at 28.9%. 16
The aim of this study is to describe the demographics, the INTERMACS profile, and Society for Cardiovascular Angiography and Interventions (SCAI) shock stage at the time of ECMO cannulation, ECMO-related complications, and outcomes at hospital discharge and 2 years post discharge for patients with CS secondary to ADHF.
Methods
A retrospective, single-center, observational study was performed on patients who received VA ECMO support for ADHF-CS at our institution between October 2014 and December 2023. Following approval from the Institutional Review Board (IRB # 23-003), data were extracted through retrospective review of electronic medical records.
Patients were cannulated either by a physician from our highly trained cardiac intensivist group, or by the referring cardio-thoracic surgeon at the outside institution or from our hospital. Further details on the referral process and ECMO cannulation strategies have been previously described. 17
We excluded from this study patients younger than 18 years, patients that required ECMO placement during cardiopulmonary resuscitation, VA ECMO patients with indications other than CS secondary to ADHF, and individuals that were placed initially on venovenous (VV) ECMO.
Patient data were reviewed for demographics, age, body mass index (BMI), VA ECMO cannulation type (peripheral vs central), cannulating physician (intensivist vs surgeon), the location of cannulation, prior mechanical circulatory support (MCS) before extracorporeal life support (ECLS), the need for continuous renal replacement therapy (CRRT) before ECMO, complications and the survival to discharge as well as the 2-year survival rate.
Additionally, the etiology of heart failure, biventricular involvement, degree of vasopressor/inotropic support, lactic acid, platelets, bilirubin, creatinine, sequential organ failure assessment (SOFA) score, SCAI shock stage, and INTERMACS profile prior to cannulation were recorded.
Statistical analysis
Data were presented as median (interquartile range (IQR)), or number (%). The differences between groups were analyzed using Mann–Whitney U test. Categorical variables were assessed using chi-square test and Fisher’s exact test when appropriate. Survival curves were generated using the Kaplan–Meier method and compared by the log-rank test.
All statistical tests were two-sided, and differences were considered significant when p ⩽ 0.05. Statistical analyses were performed using the SPSS statistical package (IBM, version 26, New York) and JMP Pro (version 12.0.1, SAS Institute, Cary, NC, USA).
Results
During the study period, 69 patients with ADHF-CS were placed on VA ECMO. The median age of the patients was 55 years old (41.5–65.5), and 42 patients (60.9%) were male while 27 (39.1%) were female. The median BMI was 28.5 kg/m2 (25.9–33.5), and median pre-ECMO length of stay (LOS) was 2 days (1–10). All patients that were placed on ECLS were cannulated peripherally. The majority of patients—65 (94%) were cannulated by an intensivist, while the remaining four patients (6%) were cannulated by a cardiothoracic surgeon. From the total number of patients, 60 (87%) were cannulated in the intensive care unit (ICU) while 9 (13%) were placed on support in the operating room (OR) or catheterization lab.
The etiology of heart failure was non-ischemic in 35 patients (50.7%) and ischemic in 34 (49.3%). Forty-five patients (65.3%) had isolated left ventricular failure, 23 (33.3%) had biventricular failure, and one patient had right ventricular failure. The majority of the patients, 64 (92.8%) were classified as INTERMACS profile 1, and five patients (7.2%) were INTERMACS profile 2.
At the time of ECMO placement, eight patients (11.6%) had SCAI shock stage E, 44 patients (63.8%) SCAI shock stage D, and the remaining 17 patients (24.6%) had SCAI shock stage C. Prior to VA ECMO placement, 30 patients (43.5%) had already undergone other type of MCS, with 23 patients receiving an intra-aortic balloon pump (IABP), and seven patients receiving a percutaneous left ventricular assist device (pLVAD; six Impella CP, one Impella 5.5). Before initiation of VA ECMO support, 10 patients (14.5%) were requiring renal replacement therapy. Pre-ECMO baseline characteristics are presented in Table 1.
Pre-ECMO demographics and clinical characteristics of the overall cohort, with comparison between hospital survivors and non-survivors.
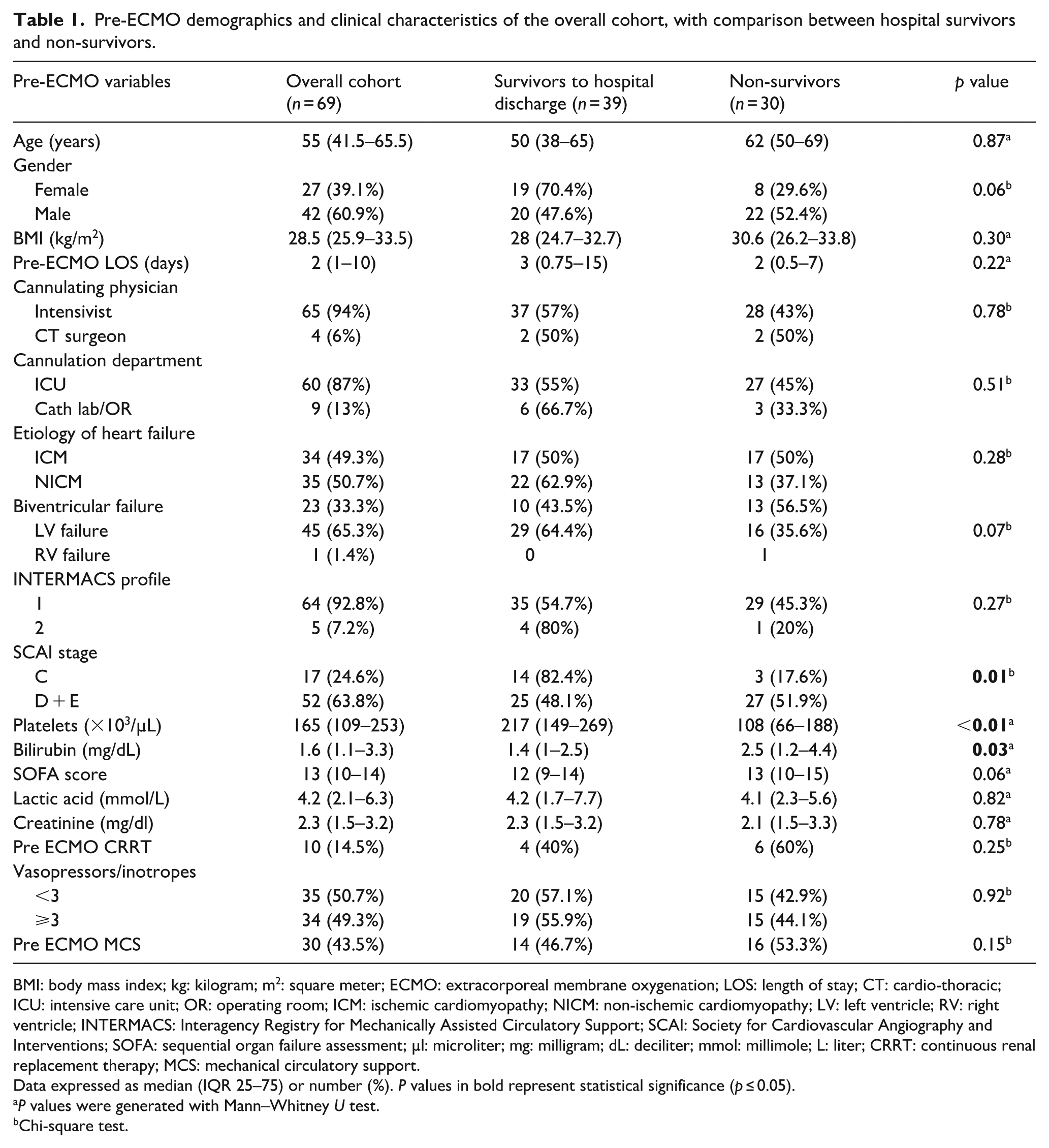
BMI: body mass index; kg: kilogram; m2: square meter; ECMO: extracorporeal membrane oxygenation; LOS: length of stay; CT: cardio-thoracic; ICU: intensive care unit; OR: operating room; ICM: ischemic cardiomyopathy; NICM: non-ischemic cardiomyopathy; LV: left ventricle; RV: right ventricle; INTERMACS: Interagency Registry for Mechanically Assisted Circulatory Support; SCAI: Society for Cardiovascular Angiography and Interventions; SOFA: sequential organ failure assessment; µl: microliter; mg: milligram; dL: deciliter; mmol: millimole; L: liter; CRRT: continuous renal replacement therapy; MCS: mechanical circulatory support.
Data expressed as median (IQR 25–75) or number (%). P values in bold represent statistical significance (p ≤ 0.05).
P values were generated with Mann–Whitney U test.
Chi-square test.
The median duration of VA ECMO support was 10 days (6.5–15), and the median hospital LOS was 34.5 days (17–54).
Complications are presented in Table 2. Notable complications that were associated with worse outcome included neurologic events (stroke, intracranial hemorrhage, and anoxic brain injury) in eight patients (11.6%), p < 0.01, bleeding complications (that included gastro-intestinal bleed, retroperitoneal bleed, ECMO cannula site bleed, and rectus sheath hematoma) in 14 (20.3%), p < 0.01 and renal replacement requirement in 24 patients (34.8%), p < 0.01.
Notable complications in the overall cohort, with comparisons between hospital survivors and non-survivors.
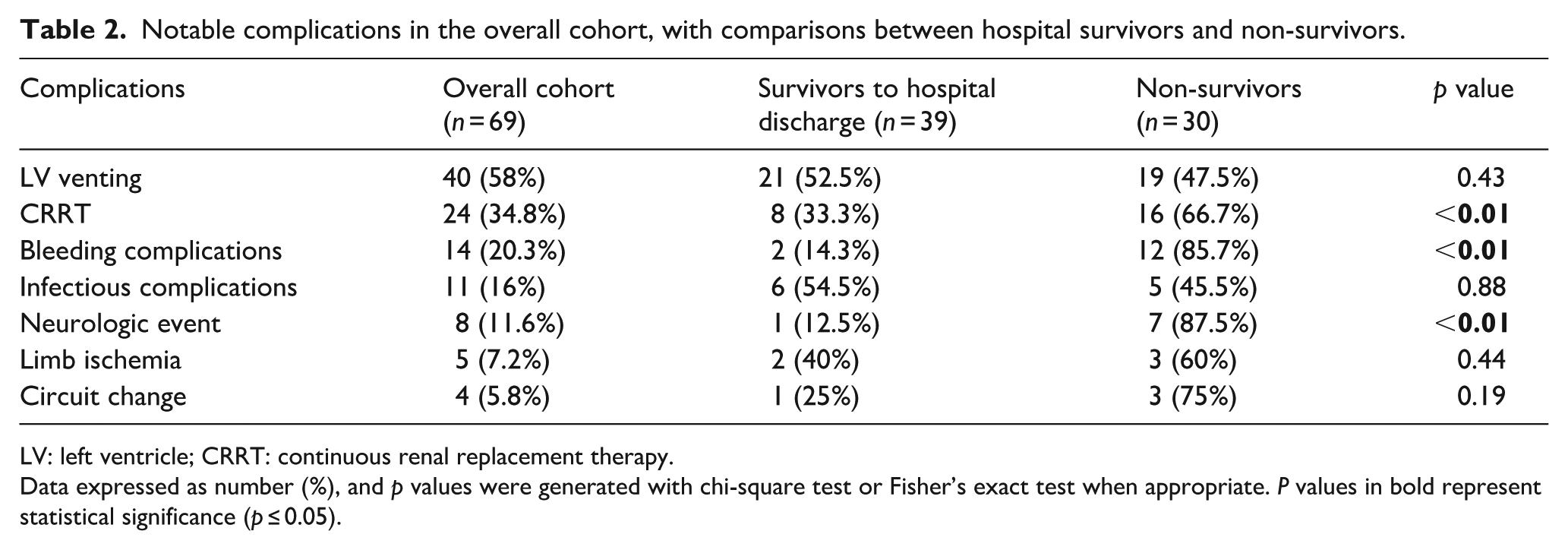
LV: left ventricle; CRRT: continuous renal replacement therapy.
Data expressed as number (%), and p values were generated with chi-square test or Fisher’s exact test when appropriate. P values in bold represent statistical significance (p ≤ 0.05).
Among the 69 patients with ADHF-CS supported with VA ECMO, 39 patients (56.5%) survived to hospital discharge, while 30 patients (43.5%) died. Of the 39 survivors, 20 patients were successfully bridged to durable left ventricular assist device (LVAD), 11 patients were weaned from VA ECMO to native cardiac recovery, and eight patients were bridged to heart transplantation. Among the 30 patients who died, 18 had care withdrawn while on VA ECMO, six were weaned off VA ECMO but subsequently died before discharge, five were bridged to durable LVAD and one patient was bridged to heart transplantation, but they did not survive to discharge (Figure 1).
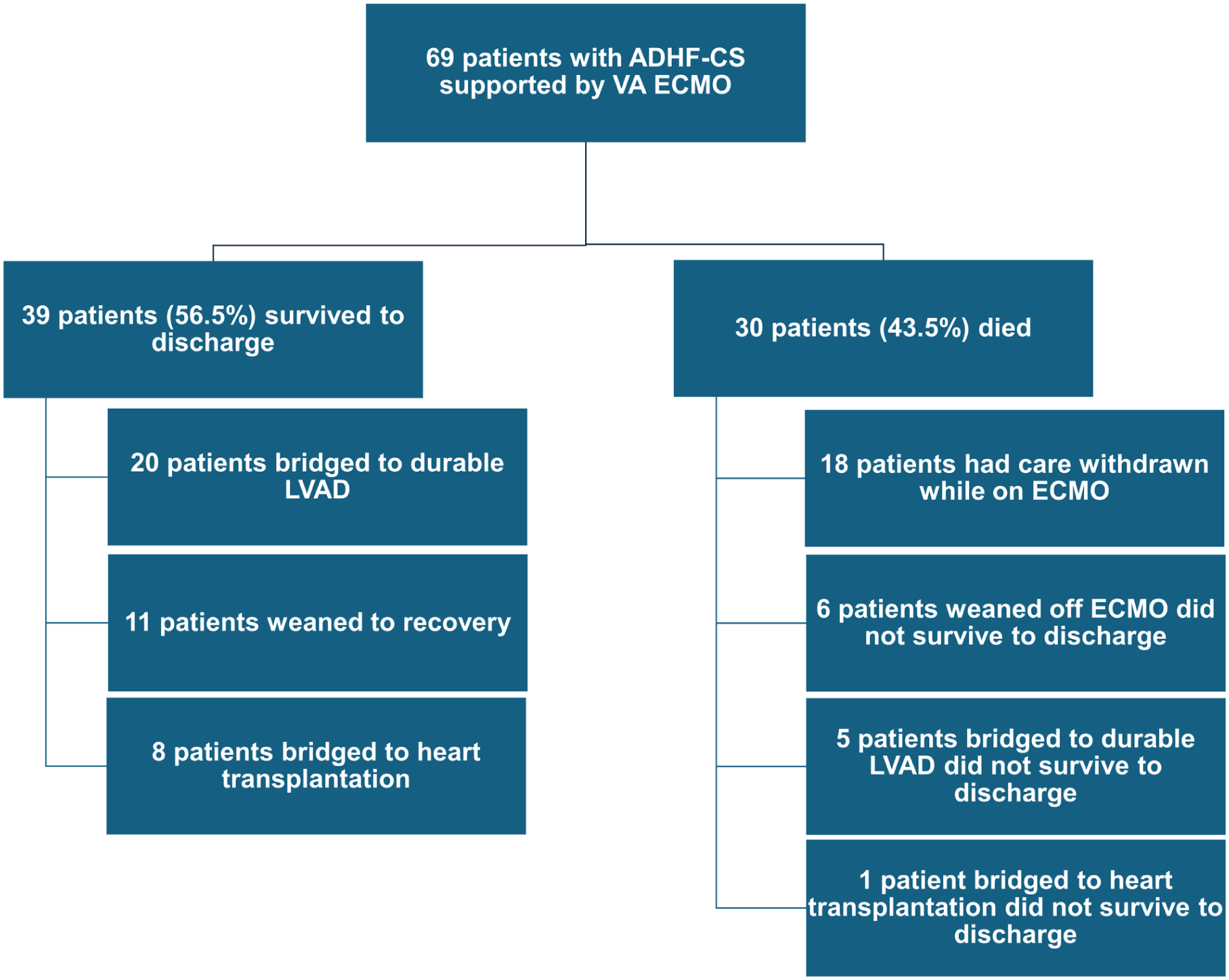
Outcomes of 69 patients with ADHF complicated by CS and supported with VA ECMO.
Out of the total number of patients that required VA ECMO support, 25 patients (36.2%) were bridged to durable MCS, while nine patients were bridged to heart transplantation (13%). Notably, 11 patients (16%) were able to be weaned off VA ECMO support and survived to discharge.
The overall 2-year survival rate for this cohort was 46.3% (Figure 2). When stratified by treatment strategy, patients who were BT-Adv demonstrated significantly higher 2-year survival (70.6%) compared to those bridged to recovery (BT-R; 22.9%; p < 0.001; Figure 3). Additionally, a higher pre-ECMO BMI (Figure 4) and SOFA score (Figure 5) were associated with increased 2-year mortality (p = 0.036 and p = 0.035, respectively). In contrast, variables such as age, pre-ECMO lactic acid levels, prior MCS before ECMO, pre-ECMO CRRT requirement, and etiology of cardiomyopathy did not show a significant association with the 2-year survival.
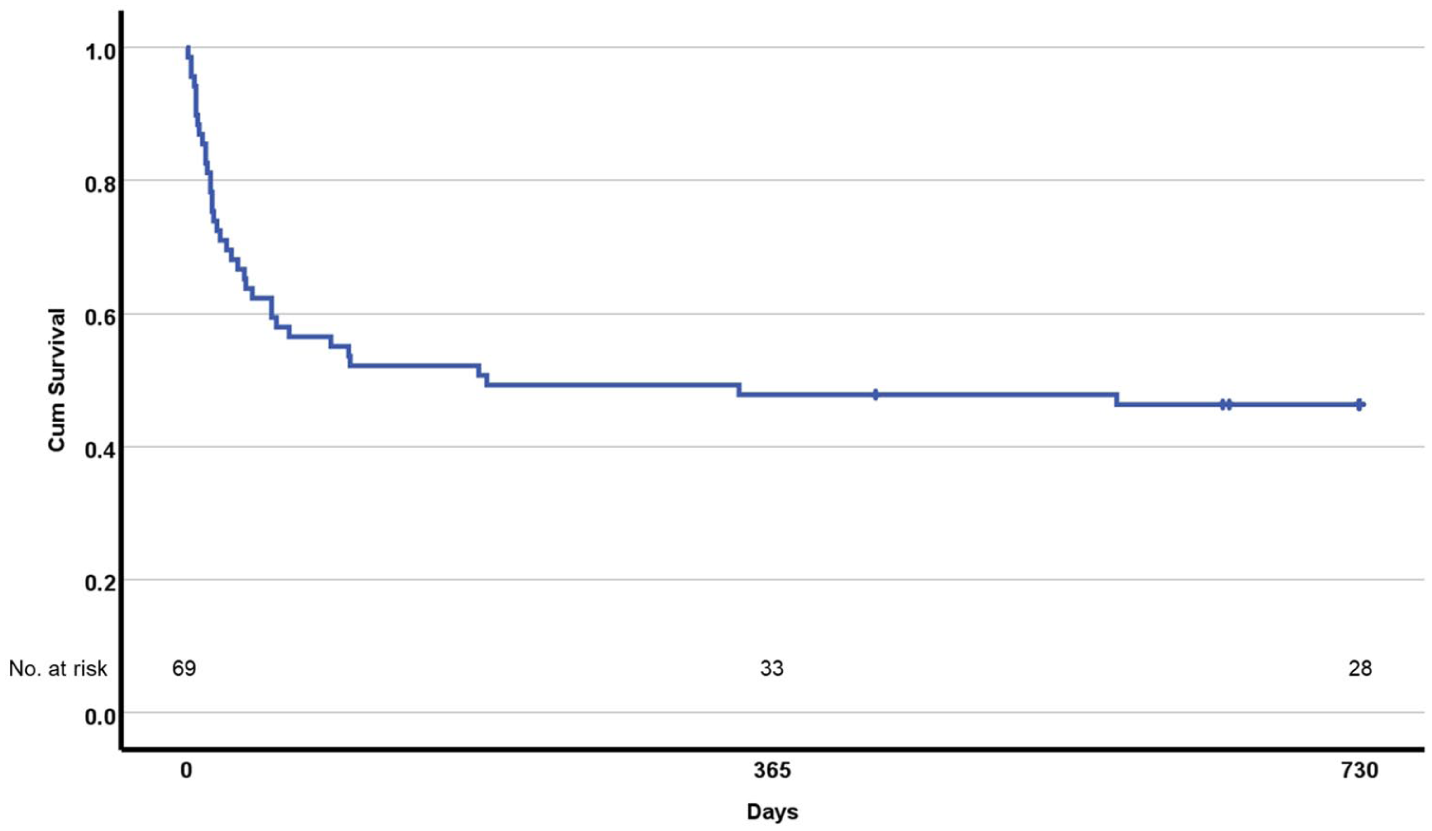
Two-year KM survival curve for the overall cohort (n = 69).
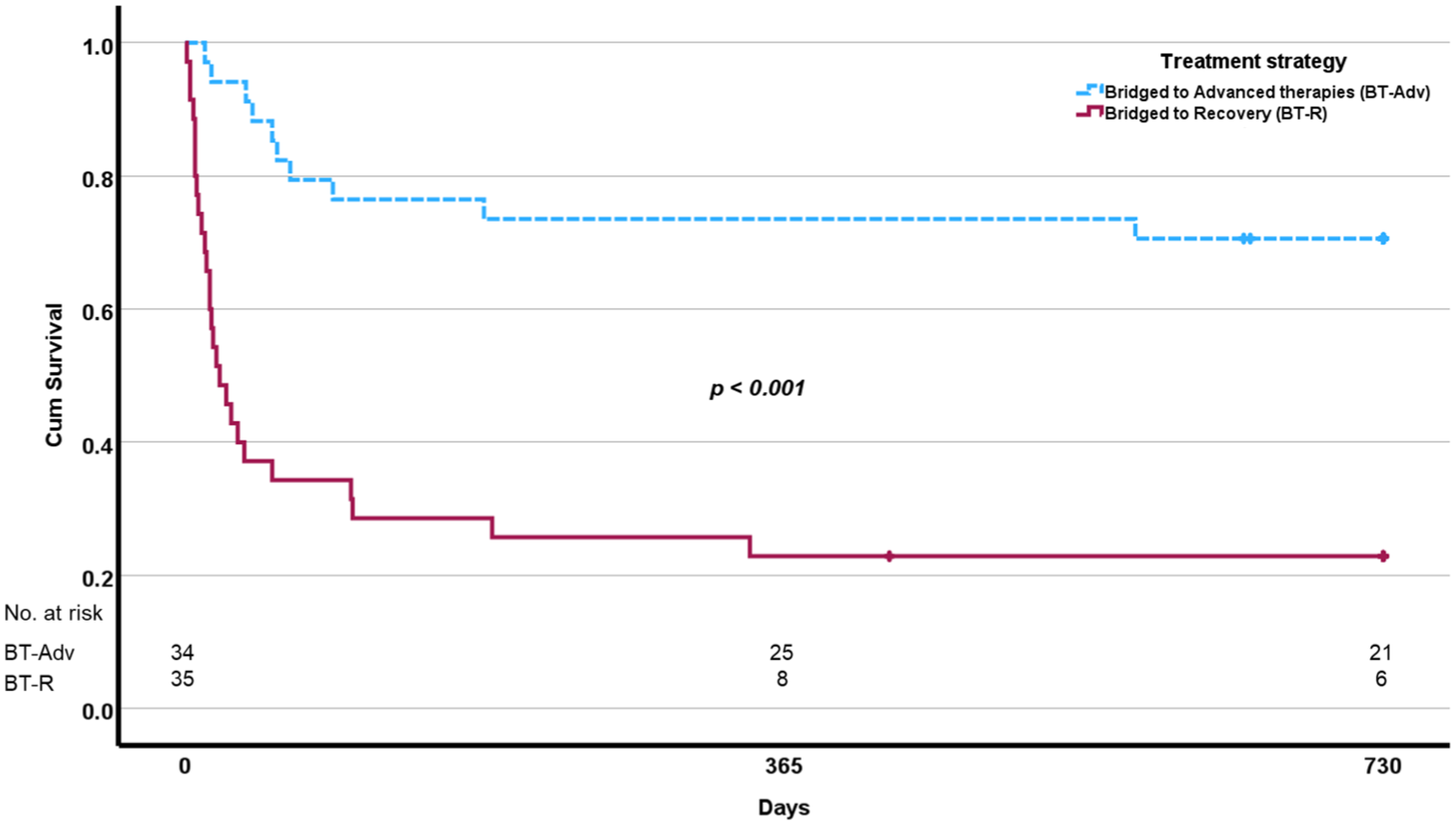
Kaplan–Meier survival curves comparing 2-year survival for patients BT-Adv compared to those BT-R. The p value was generated using log-rank test.
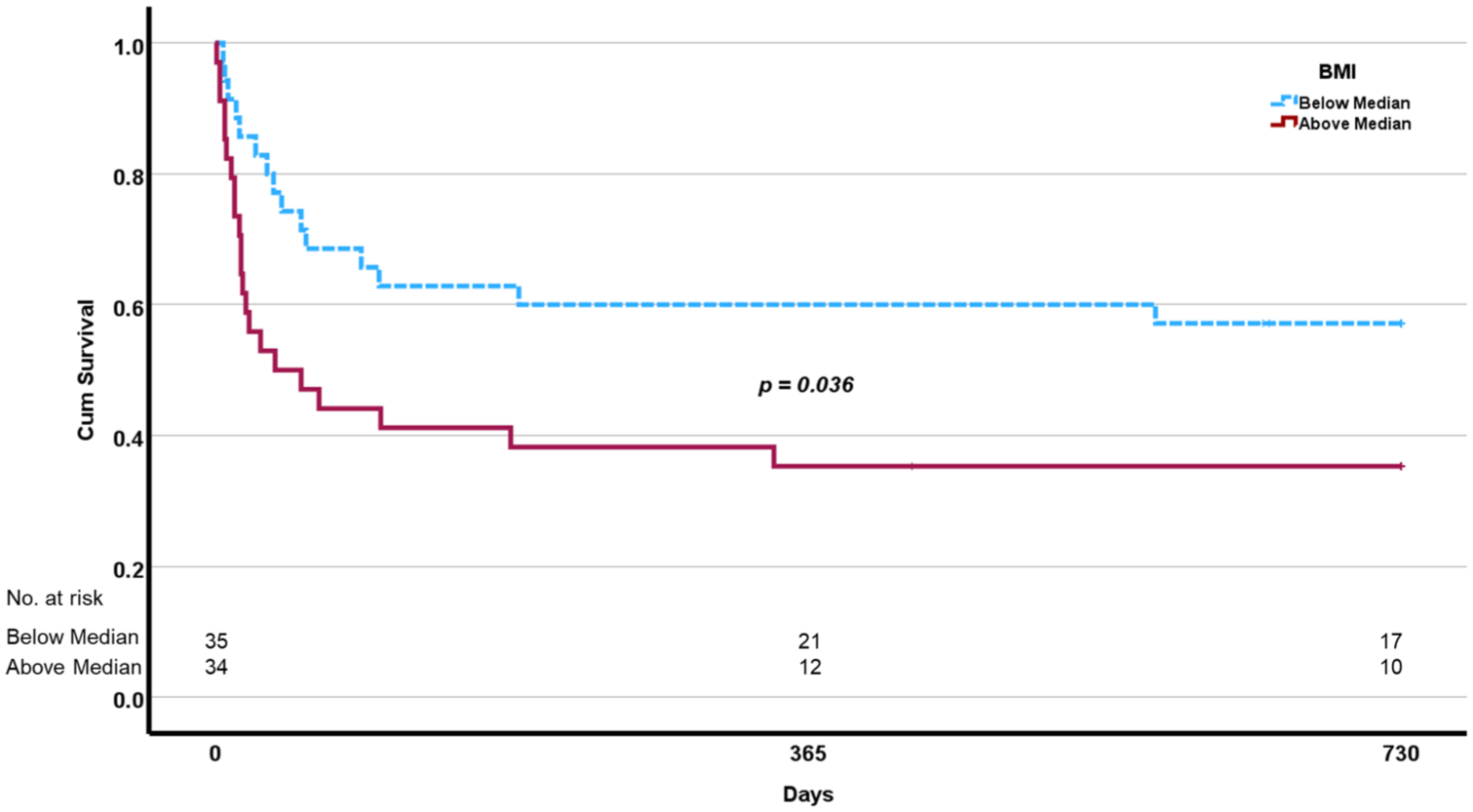
Kaplan–Meier survival curves comparing 2-year survival among patients with BMI above versus below the cohort median (28.5 kg/m2). The p value was generated using log-rank test.
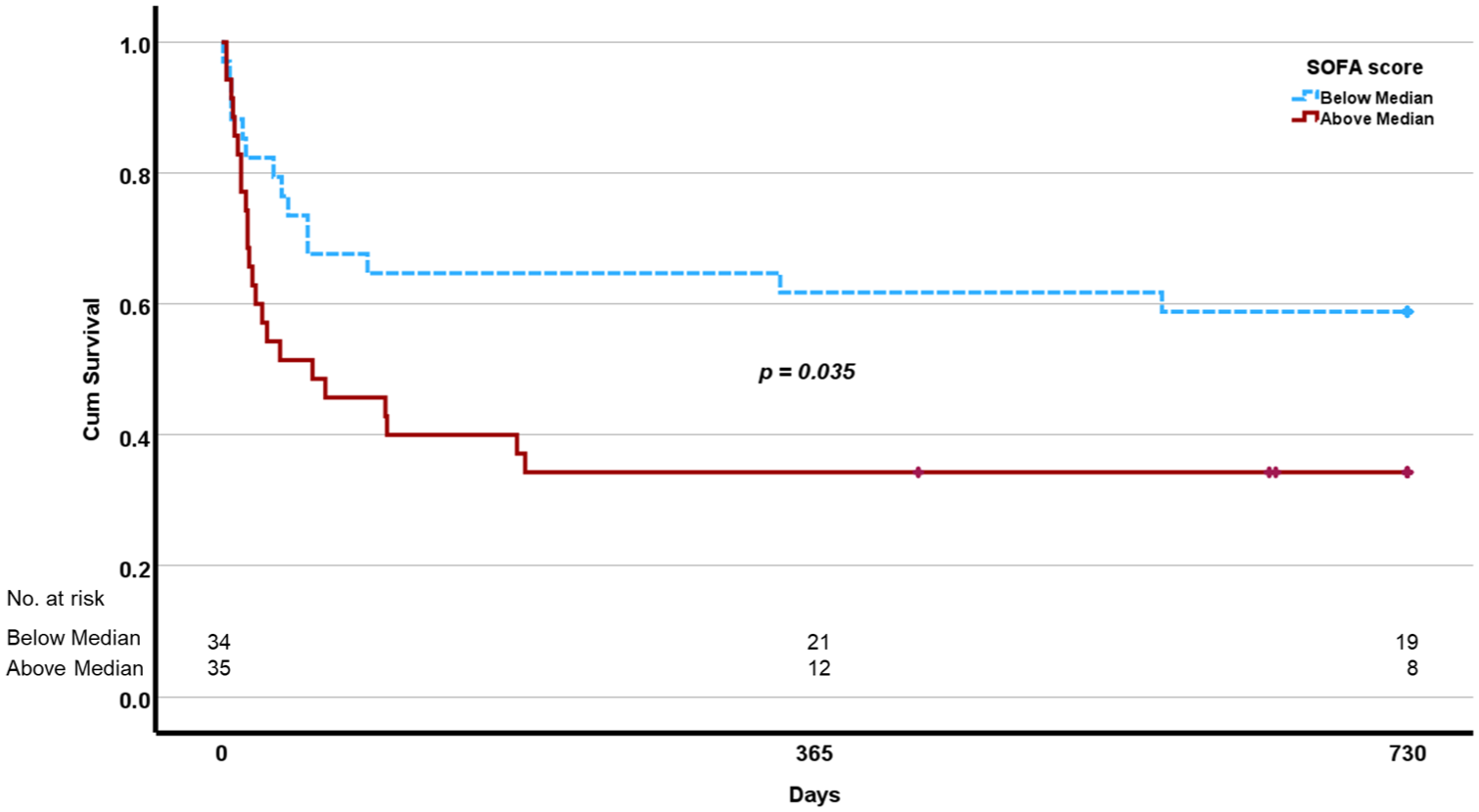
Kaplan–Meier survival curves comparing 2-year survival among patients with SOFA score above versus below the cohort median (13). The p value was generated using log-rank test.
Discussion
In this single-center, retrospective study, we describe the clinical characteristics, ECMO-related complications, and 2-year outcomes of patients with CS secondary to ADHF who required VA ECMO support. Our findings contribute to the growing body of evidence suggesting that this unique subpopulation—distinct from the more commonly studied acute myocardial infarction-related CS cohort—faces high in-hospital mortality and post-discharge challenges, despite being treated at specialized centers with access to advanced therapies and multidisciplinary shock teams.
The majority of our cohort presented with INTERMACS profile 1 or 2 and were classified as SCAI shock stage D or E, consistent with a critically ill population with high predicted mortality. Notably, 56.5% of patients survived to hospital discharge, a figure, that is, consistent with historical data showing in-hospital mortality rates ranging from 50% to 75% in similar populations. 12 Additionally, 36.2% of patients were successfully bridged to durable MCS, and 13% to heart transplantation, reaffirming the viability of VA ECMO as a bridge strategy in carefully selected patients. Interestingly, 16% of patients were weaned from ECMO and discharged without requiring further MCS, suggesting that a subset of ADHF patients with CS retain sufficient myocardial reserve for native recovery. This observation aligns with prior reports that highlight the heterogeneity in clinical trajectories among patients with ADHF-CS. 4
Our analysis identified several complications associated with mortality, including neurologic events, bleeding, and the need for renal replacement therapy. These findings reinforce existing literature emphasizing the significant morbidity burden associated with ECMO support. 9 Importantly, while factors such as pre-ECMO lactic acid, and age did not correlate significantly with 2-year mortality, a higher SOFA score, and BMI were associated with worse long-term outcomes. This may reflect the interaction between obesity, systemic inflammation, and end-organ dysfunction in the setting of ECMO, although further investigation is warranted.
Long-term survival in our cohort remained comparable, with an overall 2-year survival rate of 46.9%. However, patients who were bridged to advanced therapies had significantly better survival compared to those bridged to recovery (70.6% vs 22.9%, p < 0.001). These findings are consistent with data from the ELSO registry and other recent studies, highlighting the importance of early identification of candidates for durable support or transplantation. 16 In a study by Saeed et al. that included a total of 531 patients bridged to durable MCS after ECMO, the 1- and 3-year survival rates were 53% and 43%, respectively. Predictors for 1-year outcome were: age, female sex, lactate value, Model of End-Stage Liver Disease XI score, history of atrial fibrillation, redo surgery, and body mass index >30 kg/m2. 18 Similarly, another study by Tsyganenko et al. that analyzed 100 patients that underwent LVAD implantation post ECLS, showed a 1- and 2-year survival post LVAD implantation of 43.0% and 37.1%, respectively. Predictors for increased 1-year mortality included bilirubin increase per mg/dl, C-reactive protein increase, ECLS duration >7 days, BMI >30 kg/m2, and female gender. 19 In our analysis, only a higher pre-ECMO BMI (>28.5 kg/m2) and SOFA score >13 were associated with increased 2-year mortality.
Limitations
This study has several limitations. It is a retrospective, single-center analysis and may not be generalizable to centers with differing protocols, experience levels, or patient populations. The relatively small sample size limited subgroup analyses and precluded multivariate modeling. Additionally, longer-term (5+ years) follow-up data were not available, preventing evaluation of post-discharge outcomes and quality of life.
Conclusion
In patients with ADHF-CS, VA ECMO is a viable short-term support strategy that facilitates bridging to recovery or advanced therapies. Early intervention, patient selection, and multidisciplinary management are critical to optimizing outcomes. Future studies are needed to refine timing strategies, clarify the role of pre-ECMO support, and improve risk prediction models in this high-risk population.
Footnotes
Acknowledgements
We thank our team of advanced practice providers, nurses, and everyone involved in the care of these patients, as well as the rest of the INTEGRIS Baptist Medical Center team, for their clinical and administrative support.
Declaration of conflicting interests
All authors declare no conflict of interest relevant to the subject matter or materials discussed in this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.