
Abstract
Background:
Refractory septic shock (RSS) in children carries high mortality despite advances in critical care. Extracorporeal membrane oxygenation (ECMO) is a rescue therapy when conventional management fails. Evidence from Latin America remains limited, with no detailed reports from Chile.
Methods:
We conducted a retrospective single-center study (2009–2024) in a Chilean Pediatric ICU. Patients aged 1 month to 17 years with septic shock unresponsive to maximal conventional therapy were included. We analyzed demographics, illness severity, ECMO modality, complications, and outcomes. Primary endpoint was survival to hospital discharge.
Results:
Nine patients received ECMO (median age = 6.3 years). All had RSS, frequently associated with severe ARDS. Configurations included venoarterial (VA; n = 4), venovenous (VV; n = 4), and venoarteriovenous (VAV; n = 1), all via peripheral cannulation. Pre-ECMO median vasoactive-inotropic score was 117, and 78% required renal replacement therapy during ECMO. Overall survival was 55% (5/9). Survivors had longer ECMO runs (median 11 days vs 3 days) and ICU stays (median 63 days vs 5 days). Hemorrhage was the most frequent complication (intracranial n = 3; gastrointestinal n = 1). One survivor developed hemiparesis; no cognitive impairment was observed at 1-year follow-up.
Conclusions:
ECMO can be an effective rescue therapy for pediatric RSS, even without central cannulation capability. Distinguishing cardiogenic from vasoplegic phenotypes and identifying severe ARDS guided configuration selection (VA vs VV). These findings highlight the feasibility of peripheral ECMO in carefully selected patients within resource-limited settings, achieving survival comparable to international reports.
Keywords
Introduction
Septic shock remains one of the leading causes of mortality in pediatric intensive care units worldwide. It is characterized by circulatory and metabolic dysfunction secondary to sepsis, which, if not promptly recognized and treated, can lead to multi-organ failure and death. 1 Despite advances in antimicrobial therapy, hemodynamic monitoring, and organ support, mortality in pediatric septic shock remains between 11% and 34% in high-resource settings. 2 Refractory septic shock (RSS), defined as shock unresponsive to maximal conventional therapy, carries a substantially higher mortality, often exceeding 50%. 3
Extracorporeal membrane oxygenation (ECMO) is considered a salvage therapy for pediatric RSS when all conventional measures fail. 3 Observational studies and registry analyses have reported variable survival rates, ranging from 36% to over 70%, depending on patient selection, timing of initiation, cannulation strategy, and delivered ECMO flow. 4 High-flow venoarterial ECMO (⩾150 mL/kg/min) and central cannulation have been associated with improved outcomes, 4 although peripheral approaches remain common in centers without routine cardiothoracic surgical support. Recent studies have also reported favorable results using peripheral ECMO configurations in pediatric septic shock—particularly when initiated early and managed by experienced multidisciplinary teams. 5
While large registries and multicenter series provide comprehensive data from North America and Europe, evidence from Latin America remains extremely limited. A single-center report from Brazil described the feasibility of an alternative peripheral cannulation strategy but did not include long-term outcomes. 6 The present work contributes contemporary data from a Chilean tertiary center, representing one of the few pediatric ECMO series for septic shock reported in the region over the past 15 years.
The objective of this study was to describe the demographic, clinical, and therapeutic characteristics of pediatric patients with refractory septic shock who received ECMO support in the Pediatric Intensive Care Unit at Clínica Las Condes, Santiago, Chile, and to evaluate survival, clinical outcomes, and associated complications.
Materials and methods
This retrospective study was conducted in the Pediatric Intensive Care Unit (PICU) of Clínica Las Condes, Santiago, Chile, between 2009 and 2024. The six-bed multidisciplinary PICU admits approximately 200 patients per year and provides ECMO support for cardiac and non-cardiac indications, including referrals from public and private hospitals. The unit does not perform cardiac surgery.
ECMO management is coordinated by a multidisciplinary team composed of intensivists, perfusionists, and anesthesiologists with cardiovascular training. All indications are discussed by the ECMO committee following institutional protocols that include septic shock as a potential indication when conventional therapy fails.
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Scientific Ethics Committee of Universidad Finis Terrae–Clínica Las Condes (Protocol ID 24-053; September 30, 2024, Session No. 26). The Committee waived the requirement for informed consent due to the retrospective design, absence of interventions, and exclusive use of de-identified clinical data.
Eligible patients were aged 1 month to 17 years, fulfilled criteria for septic shock (2005 International Pediatric Sepsis Consensus 2 or 2024 Phoenix definitions, 1 depending on year of admission), and were refractory to maximal conventional therapy—including mechanical ventilation and high-dose vasoactive support. While no formal exclusion criteria were established, initiation of ECMO was determined by a multidisciplinary team, considering the severity of organ dysfunction and the perceived potential for reversibility.7,8
All ECMO procedures were performed using peripheral cannulation. VA and VV configurations targeted flows of approximately 100 mL/kg/min. Anticoagulation consisted of continuous intravenous unfractionated heparin titrated to maintain an activated partial thromboplastin time (aPTT) between 50 and 60 s.
Demographic and clinical data were extracted from institutional records, including vasoactive-inotropic score (VIS), lactate, oxygenation index (IO), Pediatric Index of Mortality 2 (PIM 2), 9 days of mechanical ventilation before ECMO, need for renal replacement therapy (RRT), ECMO modality and duration, and complications. The primary outcome was survival to hospital discharge. Secondary outcomes included ECMO-related complications and neurological status at 1-year follow-up.
Myocardial dysfunction was classified by the treating intensivist and/or cardiologist as severe, moderate, mild, or preserved. This clinical classification integrated qualitative assessment with quantitative data (Ejection Fraction (EF) and Fractional Shortening (FS)) when available in the medical records. For quantitative classification, we used standardized pediatric reference ranges, defining severe dysfunction as an EF <45% or FS <25%, moderate dysfunction as an EF 45%–55% or FS 25%–29%, and preserved function as an EF >55% or FS >29%. 10 Due to the retrospective design, specific EF/FS values were not uniformly available for all patients; in such cases, the documented clinical classification from qualitative assessment or transfer summaries was utilized.
Results
Nine pediatric patients with refractory septic shock were supported with ECMO. The median age was 6.3 years (IQR: 1.5–11), and the median weight was 20 kg (IQR: 12–40). Five patients (55%) were from the private healthcare system and 4 (45%) from the public system; 55% resided in the capital region. Four patients (44%) received mobile ECMO support, being transferred from referring centers located 10–120 km away from our institution.
Infectious sources included respiratory (n = 2), cutaneous/burn-related (n = 1), cervicofacial (n = 1), cardiovascular/endocardial (n = 1), musculoskeletal (n = 2), central nervous system (n = 1), and disseminated fungal infection (n = 1). Identified microorganisms included Staphylococcus aureus (n = 3), Haemophilus influenzae, Kingella kingae, and Candida albicans. All infections were severe and associated with multiorgan dysfunction. Eight patients developed severe ARDS—two with primary pulmonary infection and six secondary to septic shock.
Before ECMO initiation, all patients presented with severe shock and multiorgan dysfunction. The median duration of mechanical ventilation before ECMO was 2 days (IQR: 1–3). High-frequency oscillatory ventilation and inhaled nitric oxide were used in six and two patients, respectively, as rescue therapies for refractory hypoxemia. The median OI was 40 (IQR: 35–45), consistent with severe ARDS in most patients. PIM 2 was available in 7/9 patients, with a median of 65% (IQR: 30–70). Lactate levels were markedly elevated (median 28 mg/dL; IQR: 22–78). All patients required multiple vasoactive agents—most frequently norepinephrine, epinephrine, dobutamine, and dopamine, with additional use of milrinone in two patients and vasopressin in two patients. The median VIS was 117 (IQR: 84–294), underscoring the profound hemodynamic compromise preceding ECMO support. Detailed pre-ECMO demographic and clinical characteristics of individual patients are presented in Table 1.
Baseline demographic and clinical characteristics prior to ECMO initiation.
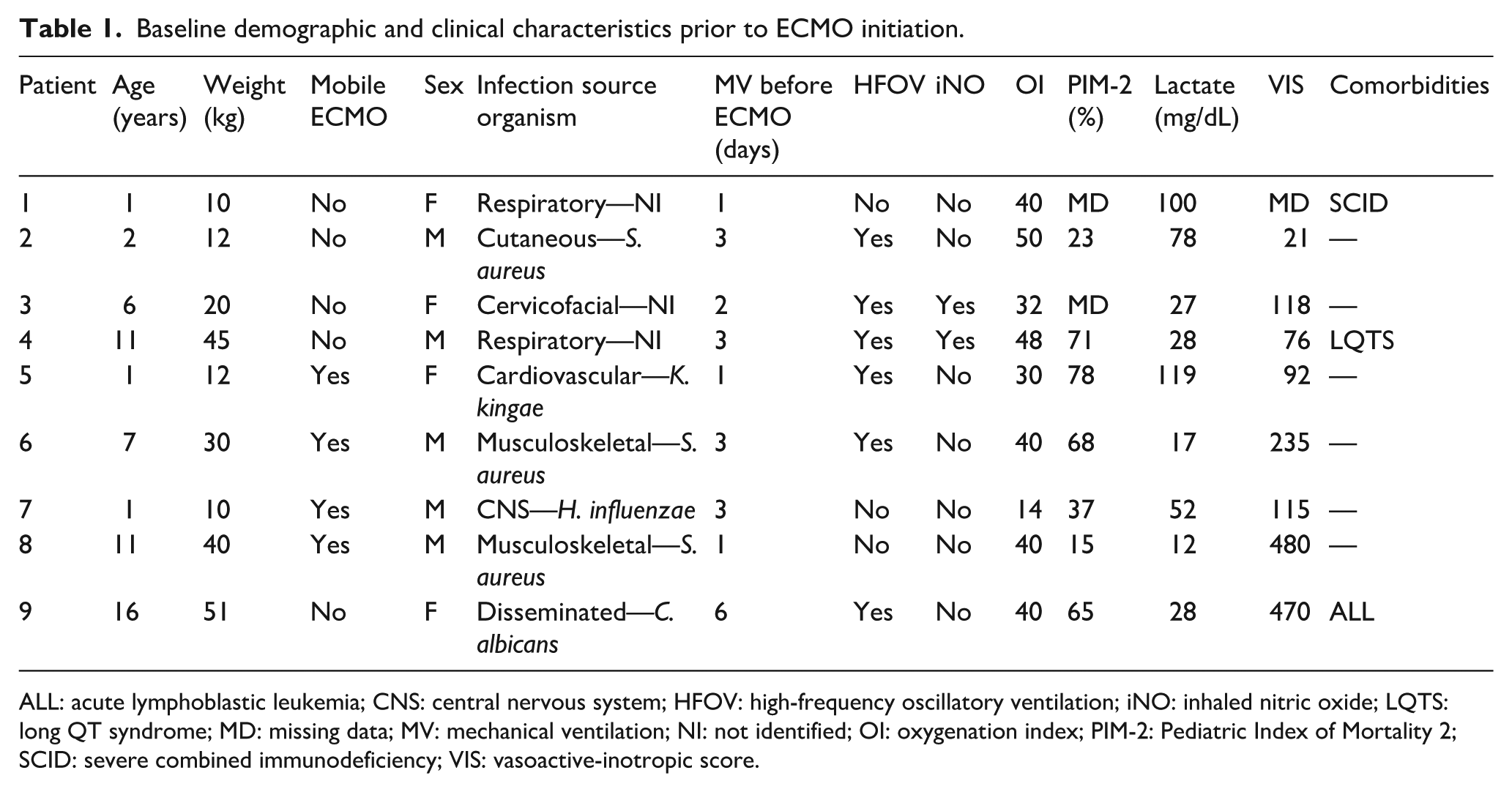
ALL: acute lymphoblastic leukemia; CNS: central nervous system; HFOV: high-frequency oscillatory ventilation; iNO: inhaled nitric oxide; LQTS: long QT syndrome; MD: missing data; MV: mechanical ventilation; NI: not identified; OI: oxygenation index; PIM-2: Pediatric Index of Mortality 2; SCID: severe combined immunodeficiency; VIS: vasoactive-inotropic score.
Echocardiography performed before ECMO revealed severe myocardial dysfunction in five patients, corresponding to the cardiogenic phenotype. Four of these patients were managed with VA-ECMO, regardless of the presence of severe ARDS, while the fifth was supported with VAV-ECMO due to severe myocardial dysfunction combined with refractory ARDS that could not be fully managed with VA configuration alone. The remaining four patients presented either moderate myocardial dysfunction (n = 2; mixed phenotype) or preserved cardiac function (n = 2; vasoplegic phenotype). All four also had severe ARDS, and therefore a VV-ECMO configuration was initially attempted. This approach achieved satisfactory hemodynamic improvement in three patients (two survived, and one had ECMO support discontinued after massive cerebral hemorrhage once shock was resolving). The fourth patient, a 16-year-old with refractory vasoplegic shock secondary to systemic candidiasis and an underlying oncologic disease with bone marrow aplasia, did not improve with VV support. Conversion to VA was considered but deemed inappropriate after multidisciplinary discussion, given her clinical condition and the likely need for central cannulation to achieve adequate flow.
Median ECMO duration was 8 days. Cannulation was performed predominantly through the cervical vessels, with two femoro-cervical configurations. Seven patients (78%) required renal replacement therapy during ECMO. Overall survival was 55% (5/9). Survivors had longer ECMO runs (median 11 days vs 3 days) and longer ICU stays (median 63 days vs 5 days). Among survivors, two had received VA-ECMO, two VV-ECMO, and one VAV-ECMO.
Hemorrhage was the most frequent complication (4/9, 44%), predominantly intracranial (n = 3) and gastrointestinal (n = 1). Among patients with intracranial hemorrhage, one experienced a massive event leading to intracranial hypertension and ECMO discontinuation. The other two presented mild bleeding; one, who had a cervical cannulation, developed residual hemiparesis without cognitive impairment, and the other had no neurological sequelae. The patient with gastrointestinal bleeding had no major consequences.
Ischemic events occurred in three patients, resulting in digital amputations in two cases and a lower-limb amputation in one.
Comorbidities included long QT syndrome diagnosed after cardiac arrest, acute lymphoblastic leukemia with secondary bone marrow aplasia, and severe combined immunodeficiency identified postmortem. The latter two patients, both with profound immunosuppression, did not survive.
ECMO configuration, physiologic phenotype, complications, and patient outcomes are summarized in Table 2.
ECMO configuration, clinical course, complications, and outcomes.
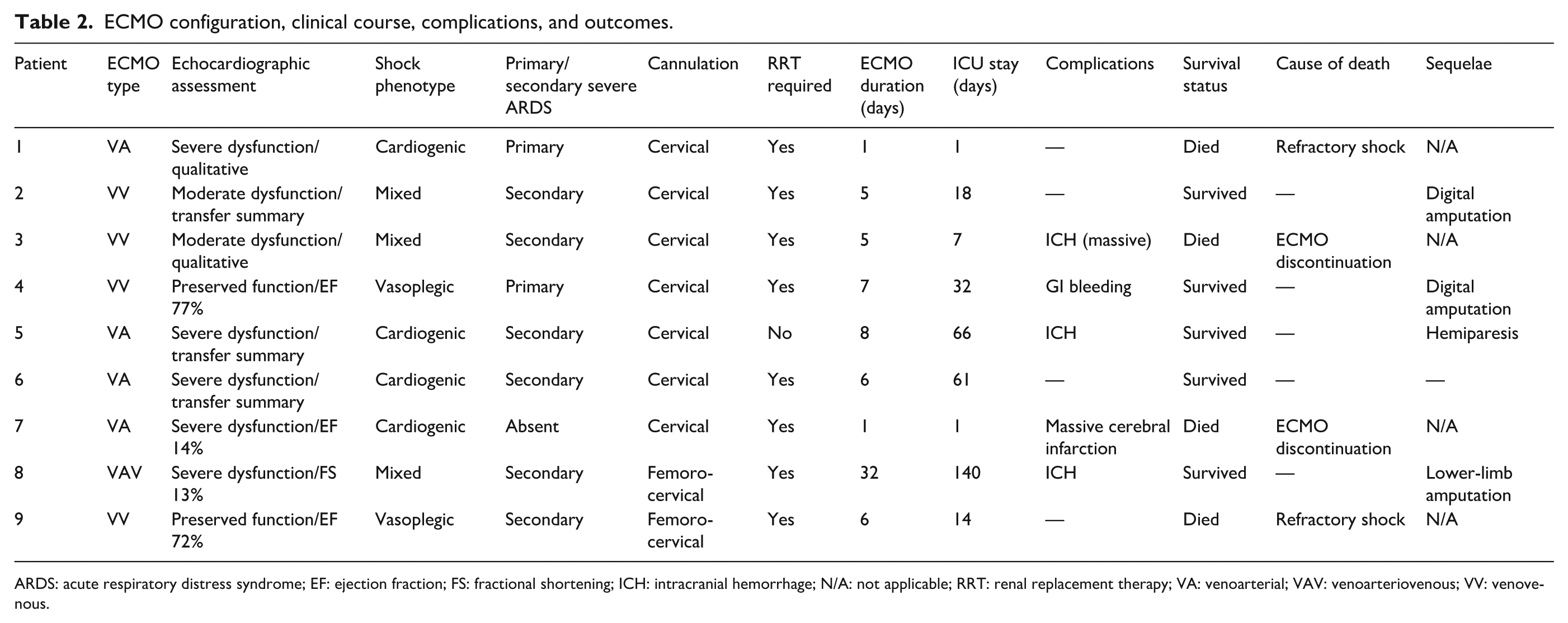
ARDS: acute respiratory distress syndrome; EF: ejection fraction; FS: fractional shortening; ICH: intracranial hemorrhage; N/A: not applicable; RRT: renal replacement therapy; VA: venoarterial; VAV: venoarteriovenous; VV: venovenous.
Discussion
This single-center Chilean experience demonstrates that ECMO can be effectively implemented as a rescue strategy for pediatric refractory septic shock, achieving a survival rate of 55%. This figure lies within the range reported in international series, where survival varies between 44% and 68%, depending on patient selection, timing of initiation, and ECMO configuration.4,5,11 Despite the absence of central cannulation and the resource limitations of our setting, outcomes were comparable to those reported in larger cohorts.
Patient characteristics in our cohort—marked by high vasoactive–inotropic requirements, frequent need for renal replacement therapy, and a predominant presentation with severe ARDS—were consistent with those described in multicenter studies of pediatric septic shock supported by ECMO. 12 Similarly, the distribution of ECMO modalities in our series, with both VA and VV configurations achieving comparable survival, aligns with recent reports suggesting that institutional expertise and early initiation may mitigate the historically lower survival associated with VA-ECMO.
Refractory septic shock usually requires VA-ECMO support because of the frequent coexistence of cardiovascular failure and myocardial dysfunction. However, in carefully selected patients with severe ARDS and mild-to-moderate myocardial dysfunction—not severe—VV-ECMO may still provide sufficient support to reverse shock. In our series, this approach achieved satisfactory hemodynamic stabilization in most patients, supporting previous reports suggesting that this configuration may be appropriate when cardiac output is only moderately compromised.13,14 These findings reinforce the importance of tailoring ECMO configuration according to the predominant pathophysiologic phenotype.
All patients exhibited rapidly progressive multiorgan dysfunction and high vasoactive-inotropic scores before cannulation, reflecting the severity of pre-ECMO status. Early cannulation—after a median of only 2 days of mechanical ventilation—likely contributed to the favorable outcomes observed, consistent with evidence supporting early initiation before irreversible organ failure occurs. 11
Bleeding was the most frequent complication, consistent with previous pediatric ECMO literature.15,16 Balancing anticoagulation and bleeding risk remains a key challenge, underscoring the need for individualized protocols and close neurologic surveillance.
Ischemic complications were observed in three patients, all of whom had presented with severe shock, high vasoactive-inotropic requirements, and signs of peripheral hypoperfusion prior to cannulation, which may have contributed to these outcomes.
Even within a resource-limited setting, our results demonstrate that peripheral ECMO for pediatric refractory septic shock is both feasible and effective when conducted by experienced multidisciplinary teams. Recognition of physiologic phenotypes—including the coexistence of severe ARDS—and timely initiation are central to optimizing outcomes. These findings support ECMO as a viable life-saving therapy in developing healthcare systems.
Footnotes
Author contributions
All authors contributed to the study conception and design. Material preparation, data collection, and analysis were performed by Loreto Godoy, Mauricio Yunge, Jorge Rufs, Alejandra Gatica, Carlos Muñoz, and Cristian Valverde. The first draft of the manuscript was written by Loreto Godoy and Cristian Valverde, and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and analyzed during the current study are not publicly available due to patient privacy and institutional restrictions. De-identified data may be available from the corresponding author on reasonable request and with permission of Clínica Las Condes.
Ethical considerations
This retrospective study was conducted in accordance with the Declaration of Helsinki and was approved by the Scientific Ethics Committee of Universidad Finis Terrae–Clínica Las Condes (Protocol ID 24-053; September 30, 2024, Session No. 26). The Committee waived the requirement for informed consent due to the retrospective design, absence of interventions, and exclusive use of de-identified clinical data.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Code availability
Not applicable.