
Abstract
Background:
This study aimed to evaluate the impact of sarcopenia and frailty on the quality of life of older hemodialysis patients.
Methods:
Seventy hemodialysis patients aged ⩾60 years were assessed. Daily living activities (Katz Index), depression (Yesavage Scale), frailty (Fried’s Criteria), and sarcopenia (EWGSOP2) were evaluated. Quality of life was measured using the KDQOL-36 questionnaire.
Results:
The median age was 67 years, and 50% were female. Nineteen patients (27.1%) were partially dependent, 71.4% were pre-frail, and 15.7% were frail. Probable sarcopenia was detected in 77.1%, and sarcopenia in 8.6% of patients. Sarcopenia was associated with older age, higher dependency, depression, lower income, and frailty (p < 0.05). It was also related to the KDQOL-36 physical component (p = 0.031), while frailty correlated with the symptom component (p = 0.047).
Conclusion:
Frailty and sarcopenia are common in older hemodialysis patients and adversely affect their quality of life.
Introduction
The prevalence of chronic kidney disease (CKD) in the general population is approximately 14%, while the prevalence of albuminuria is around 7%. 1 Globally, CKD accounted for 1% of disability-adjusted life years and 1%–3% of life lost in 2012. 2
Sarcopenia is associated with functional impairments, reduced quality of life, falls, osteoporosis, dyslipidemia, increased cardiovascular risk, metabolic syndrome, and immunosuppression. The decline in muscle mass and muscle function are linked to a 3.7-fold increase in mortality and a twofold increase in the risk of falls.3–5 Sarcopenia is also associated with a 50% higher risk of hospital admission, a 20-day increase in hospital length of stay, and approximately a 34% increase in hospital care costs.6,7 Frail older adults are less able to tolerate or adapt to stressors such as acute illness, surgery, medical interventions, or trauma compared to younger or non-frail older adults. 8 After adjusting for comorbidities, frailty predicts hip fractures, disability, and hospitalizations. 9 Furthermore, frailty is associated with adverse outcomes related to kidney transplantation and surgical interventions.10,11
The quality of life in hemodialysis patients can be adversely affected due to their dependence on the dialysis machine and the strict conditions they must adhere to. Psychiatric problems such as depression and anxiety are also frequently observed in this patient group, further impacting their quality of life. There is a lack of sufficient clinical studies focusing on frailty and sarcopenia in older hemodialysis patients. To the best of our knowledge, there is no study examining both syndromes and their effects on the quality of life in hemodialysis patients in our country.
The aim of this study is to investigate if sarcopenia and frailty affect the quality of life in older patients undergoing hemodialysis.
Materials and methods
This study included 70 hemodialysis patients from two centers. Ethical approval was obtained from the local ethics committee (approval no: 2019/005). Patients aged ⩾60 years who volunteered and were able to complete questionnaires were included. Those with active malignancy, recent hospitalization or surgery, acute infection, advanced dementia, psychiatric or degenerative neurological disorders were excluded. Demographic and clinical data were recorded. The Katz Index of Independence in Activities of Daily Living 12 assessed daily living activities, and the Yesavage Geriatric Depression Scale 13 evaluated emotional status. Comorbidity burden was determined using the Charlson Comorbidity Index. 14
Frailty was determined by Fried’s criteria.15,16 Patients meeting ⩾3 criteria were classified as frail, 1–2 as pre-frail, and none as robust. Sarcopenia was diagnosed using EWGSOP2 criteria. 17 Walking speed (4-m test), handgrip strength (CAMBRY EH101 dynamometer), and muscle mass (TANITA BC-418 MA bioimpedance) were measured. Cutoffs were ⩽0.8 m/s for slow walking, <22 kg (women) and <32 kg (men) for low grip strength, 18 and FFMI <17.51 kg/m² (men) or <14.52 kg/m² (women) for low muscle mass. 19 Low strength alone indicated probable sarcopenia; combined low strength and mass indicated sarcopenia; additional slow walking indicated severe sarcopenia. The Katz Index (0–6 points) measured independence. 12 The short-form Yesavage scale classified scores 0–4 as normal, 5–10 as mild depression, and >10 as moderate-to-severe. 20 Quality of life was evaluated using the KDQOL™-36, which includes general and kidney disease-specific sections with five subscales scored 0–100, where higher scores indicate better quality of life.21,22
Analyses were performed using SPSS 24.0 (IBM, Armonk, NY, USA). Categorical variables were compared using Chi-square or Fisher’s exact tests. Normality was assessed with the Kolmogorov–Smirnov test. Parametric data were analyzed with Student’s t-test or ANOVA; nonparametric data with Mann–Whitney U or Kruskal–Wallis tests. Correlations were evaluated with Spearman’s test, and p < 0.05 was considered statistically significant.
Results
A total of 70 patients participated in the study, with 35 (50%) female. The median age of the participants was 67 years (range 60–80). The median duration of hemodialysis was 24 months (range 1–240). According to the Katz scale, 51 participants (72.9%) were fully independent, while 18 (25.7%) had mild depression based on the Yesavage scale. In terms of depression severity, 16 participants (22.9%) were classified as having moderate to severe depression. Regarding frailty status, 50 participants (71.4%) were pre-frail, and 11 (15.7%) were frail. According to the EWGSOP2 criteria, 54 participants (77.1%) had probable sarcopenia, and 6 (8.6%) had sarcopenia.
When comparing the clinical characteristics of patients based on sarcopenia status, it was found that sarcopenic patients were older, weaker, more frail, had higher Yesavage scores, and lower activity of daily living scores (all had p-value <0.05). A statistically significant relationship was found between sarcopenia and KDQOL36’s physical component (p = 0.031; Table 1).
Comparison of patients based on sarcopenia status.
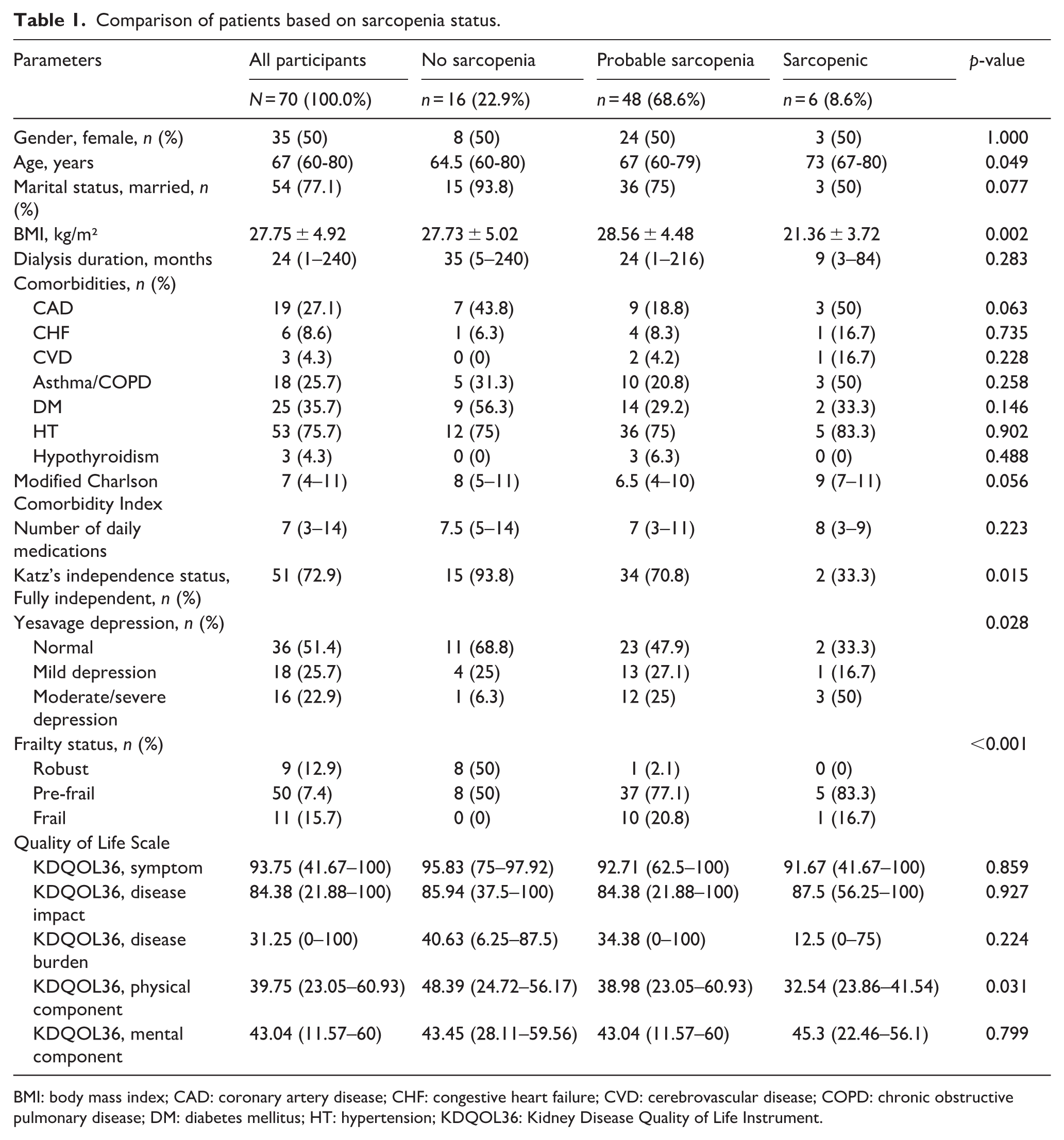
BMI: body mass index; CAD: coronary artery disease; CHF: congestive heart failure; CVD: cerebrovascular disease; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; HT: hypertension; KDQOL36: Kidney Disease Quality of Life Instrument.
When comparing patients based on frailty status, statistically significant relationships were found between frailty and the Katz dependency score, asthma/COPD diagnosis, Yesavage depression status, dialysis duration (p = 0.012, p = 0.037, p = 0.01, and p = 0.003, respectively), and sarcopenia (p < 0.001). When assessing the quality of life using the KDQOL36 scale according to frailty status (robust, prefrail, and frail), no statistical significance was observed between the symptom, disease impact, disease burden, and physical and mental component groups. However, upon a detailed examination of each subgroup, it was visually observed that the scores worsened as the frailty status progressed from the robust to the frail group. On the other hand, when the patients were divided into two groups as having or not having frailty, it was observed there was a significant relation between frailty and the KDQOL36 symptom component (p = 0.047; Table 2).
Comparison of patients based on frailty status.
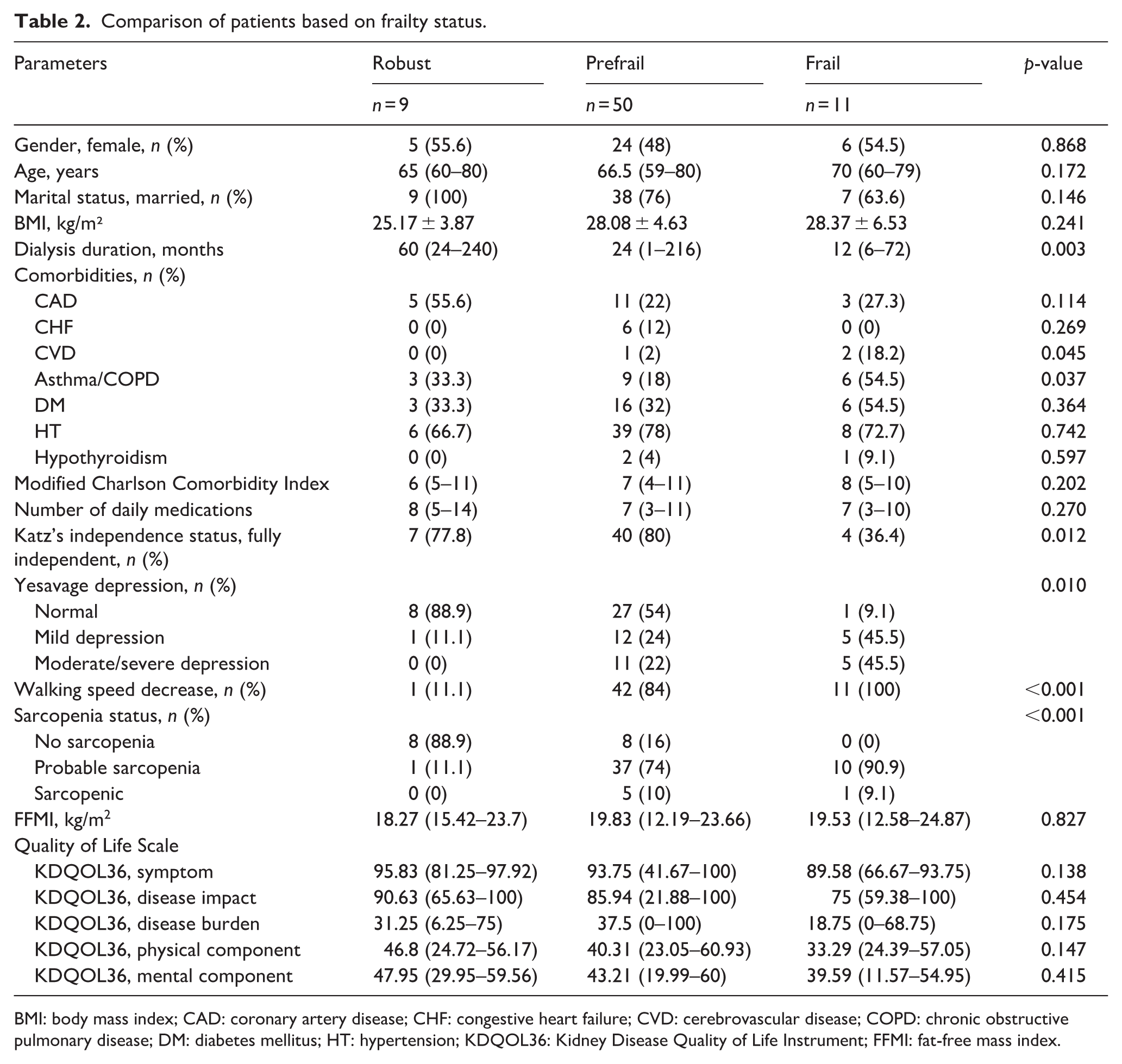
BMI: body mass index; CAD: coronary artery disease; CHF: congestive heart failure; CVD: cerebrovascular disease; COPD: chronic obstructive pulmonary disease; DM: diabetes mellitus; HT: hypertension; KDQOL36: Kidney Disease Quality of Life Instrument; FFMI: fat-free mass index.
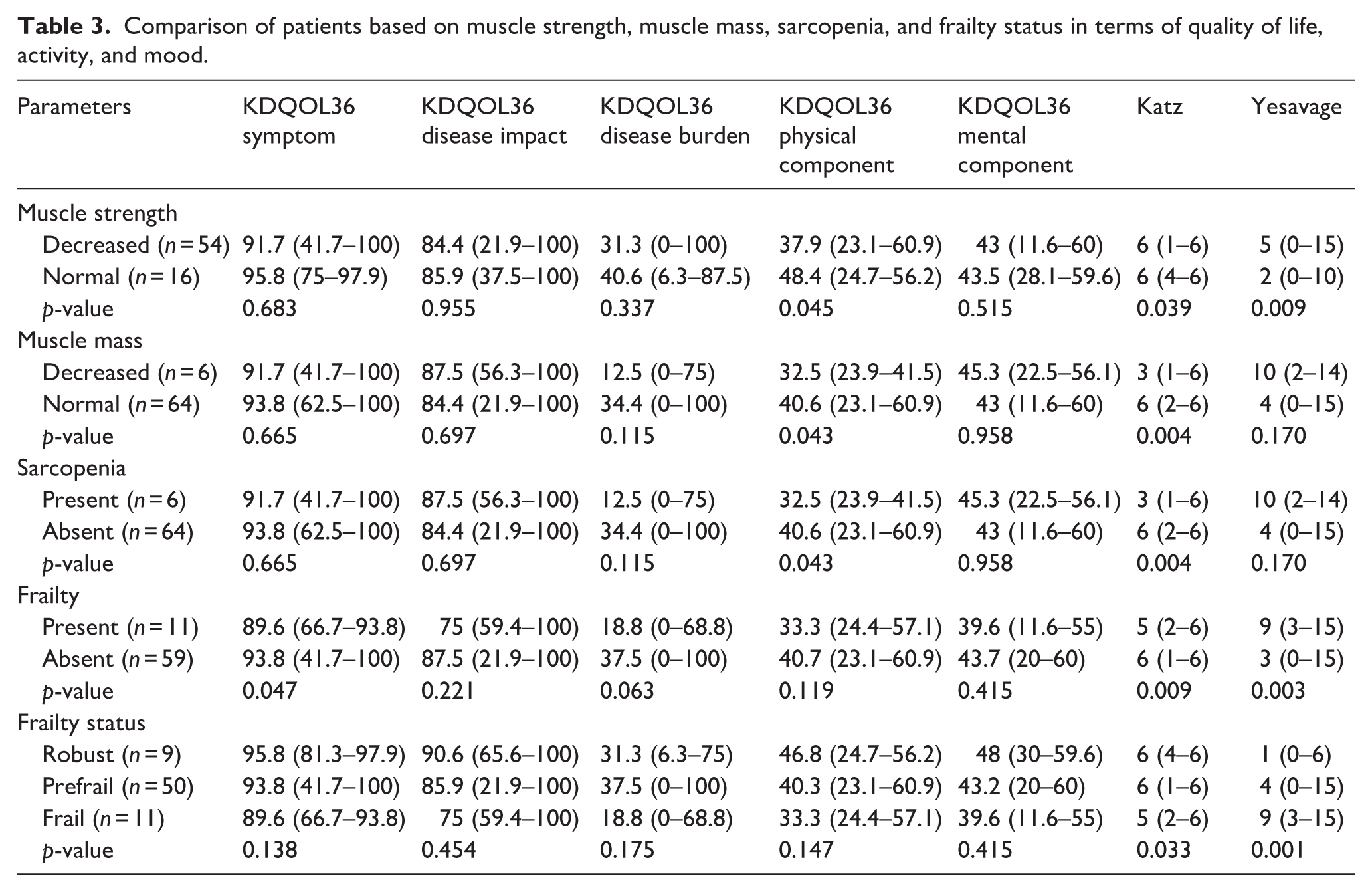
A statistically significant relationship was found between decreased muscle strength, muscle mass loss, and sarcopenia with the KDQOL36 SF-12 physical component and between frailty and the KDQOL36-Symptom component. A statistically significant relationship was found between muscle strength and mass decreases, frailty, sarcopenia, and the Katz dependency score. A statistically significant relationship was also found between decreased muscle strength, frailty, and the Yesavage depression score. Detailed comparisons are provided in Table 3.
Comparison of patients based on muscle strength, muscle mass, sarcopenia, and frailty status in terms of quality of life, activity, and mood.
Discussion
In our study, the prevalence of frailty and sarcopenia among hemodialysis-dependent CKD patients was 15.7% and 8.6%, respectively. Frail and sarcopenic patients showed marked impairments in quality-of-life domains, particularly in the physical and symptom components, as well as in daily activities and emotional well-being.
Previous studies have reported high dependency rates among older dialysis patients. Cook et al. 23 found that 85 of 162 patients over 65 years were dependent, while Johansen et al. 24 showed that physical performance declined with age, low serum albumin, and dialysis dose. Similarly, we found a dependency rate of 25.7%, underlining the need for early identification and management of contributing factors.
Depression is also common in this population. Reported rates range from 17% to 51%,25–27 while in our study, 25.9% had mild and 22.7% had moderate-to-severe depression. The higher rate may be attributed to the older age of our cohort.
Meta-analyses and cohort studies have shown frailty rates between 21% and 56% in dialysis patients.28–30 Our study found 71.4% pre-frailty and 15.7% frailty, likely reflecting the older age of participants. Patient education, prevention strategies, and targeted management are essential.
Sarcopenia prevalence in dialysis patients varies between 8% and 33% depending on criteria31–33; our finding of 8.6% aligns with these reports. Sarcopenia screening and intervention should be part of routine care. Consistent with previous studies, 66.7% of sarcopenic patients in our cohort were partially dependent,34–36 emphasizing the importance of effective sarcopenia management.
Depression was also frequent in sarcopenic patients, with rates of 51%–67% reported in the literature37,38 and 66.7% in our study, highlighting the need for psychological assessment in this group.
Studies have shown reduced quality of life in sarcopenic individuals, particularly in mobility and physical domains.39,40 We also observed lower physical component scores, though not statistically significant, likely due to limited sample size. Identifying and addressing modifiable factors remains crucial.
Frailty has also been linked to lower quality of life.41,42 Although our study did not demonstrate statistically significant differences, quality-of-life scores declined progressively from robust to frail patients. Correlations between FFMI, handgrip strength, walking speed, and quality-of-life subdomains support that both sarcopenia and frailty are major determinants of well-being in dialysis patients.
Conclusion
Our findings indicate that frailty and sarcopenia are common in older dialysis patients and negatively impact their quality of life. Addressing these conditions may enhance patient well-being. The main limitations of this study are its small sample size and cross-sectional, single-center design. Despite the lack of statistical significance, the trend toward lower quality-of-life scores in sarcopenic patients provides valuable insights for future research.
Footnotes
CRediT authorship contribution statement
FBÇK: Conceptualization, Methodology, Investigation, Formal analysis, Writing – original draft. FE: Conceptualization, Investigation, Visualization, Writing – review & editing ÇK: Conceptualization, Investigation, Visualization. Writing – review & editing FS: Conceptualization, Investigation, Visualization, Writing – review & editing IG: Software, Formal analysis, Writing – original draft, Visualization Conceptualization, Methodology, Writing – review & editing, Supervision. MCK: Conceptualization, Methodology, Formal analysis, Writing – review & editing, Supervision
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval statement
Approval was obtained from the Ethics Committee for Non-Drug and Non-Medical Device Research of Necmettin Erbakan University on May 17, 2024, with the decision number 2024/4986.
Consent to participate
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Non-Drug and Non-Medical Device Research of Necmettin Erbakan University (no. 2024/4986) on May 17, 2024, with the need for written informed consent waived.
Consent for publication
Not applicable.