
Abstract
Introduction:
The aim of our study was to compare the prevalence, etiology, and outcomes of sepsis and associated AKI in pre- and post-COVID-19 pandemic.
Methods:
We conducted a retrospective observational analysis in 144 patients with sepsis and AKI, in two periods of time, 2 years before and after COVID-19 pandemic, with 2 years’ washout period.
Results:
The comparative analysis between the two periods demonstrated more severe forms of sepsis with septic shock dominating in the post pandemic period (5 (10%) vs 23 (25%), p = 0.037). According AKI staging we found AKI stage 3 more frequently present after pandemic and more patients needed dialysis in the post COVID-19 pandemic (35 (70%) vs 79 (84%), p = 0.04; 31 (62%) vs 78 (54%), p = 0.02; 16 (32%) vs 51% (54%), p = 0.018), respectively. Patients in post COVID-19 era survived less longer (22.66 ± 11.32 vs 17.132 ± 12.66, p = 0.021) with almost doubled risk for mortality HR: 1.977; 95% CI (1.127 ± 3.469), p = 0.018. Regarding causative agents’ there was similar distribution in both periods, but the multiple antibiotic resistance index (MAR) was significantly higher in the post COVID-19 period for Staphylococcus coagulase negative (0.48 vs 0.62, p = 0.001).
Conclusion:
Sepsis and associated AKI occurrence, morbidity and mortality are significantly higher in the post COVID-19 pandemic and the increased MAR of the germs can be one of the main reason for it.
Introduction
COVID-19 pandemic dramatically changed the world. Although the pandemic has been declared over, SARS-CoV-2 virus is still active in human population causing more or less severe infections all over the world, we are at the stage of understanding and experiencing the long-term consequences on general health globally.1,2 A number of studies confirmed that COVID-19 pandemic did make permanent dysregulations and dysfunctions of the immune and vascular system and by that influenced each organic system.3,4 Rising trends of antimicrobial resistance and its threat to public health, has been of interest for researchers worldwide and many studies are dedicated to it, including scientists and data form North Macedonia. 5 It is believed that the inappropriate and uncontrolled use of antibiotics in the pandemic era substantially changed microorganisms and triggered expansion of the antimicrobial resistance (AMR) globally, influencing its’ clinical and therapeutic features. 6
Since the first consensus definitions for sepsis was established (1991), its incidence is constantly rising, posting considerable burden to health systems worldwide. 7 According to the latest consensus definition, sepsis is defined as a life-threatening organ dysfunction due to an inappropriate host reaction to infection, with septic shock being the most severe form. 8 Kidneys are one of the many affected organs and acute kidney injury (AKI) due to sepsis is common manifestation. Kellum et al. emphasizes that AKI can be early sign of sepsis, considering that half of patients with sepsis included in the study, presented with AKI even before consulting the emergency departments. 9 Despite continues improvements in recognizing and managing sepsis, sepsis-related mortality remains very high, and according to latest World Health Organization (WHO) statements, it represents 20% of all global deaths, especially in lower-middle- income countries. 10 Although these rising numbers can be partially explained by the new developed tools for fast and prompt diagnosis like the quick sequential organ failure assessment (qSOFA) score, especially useful for outpatients, it seems that there are other contributing factors that need to be analyzed yet.7,8
The aim of this study was to estimate how the COVID-19 pandemic changed prevalence, etiology, and outcomes of sepsis associated with AKI, comparing the pre- and post-COVID-19 pandemic period and also to address the distribution of different microorganisms as causative agents including their antimicrobial resistance.
Methods
Study design
We conducted a single-center retrospective, observational, comparative study in 144 patients with sepsis and associated AKI, hospitalized in our University Hospital of Nephrology in Skopje during period of 2 years before (2017–2019) and 2 years after (2022–2024) COVID-19 pandemic, with 2 year’s washout period. All patients with age over 18 that full-fielded sepsis-3 criteria, according to the latest consensus definition for sepsis in 2016, 11 were included in the analysis. Patients with kidney transplants, primary glomerulopathies, and vascular access related sepsis in patients with end stage kidney disease (ESKD) that require renal replacement therapy, were excluded from the study. This retrospective study was conducted as claimed by the principles of the Declaration of Helsinki, in agreement with institutional policy for obtaining informed consent at hospital admission.
Data collection and definitions
Population
The University Hospital of nephrology—Skopje, as a unique tertiary public hospital for kidney diseases provides care for referred patients from all over the state, covering approximatively two million citizens. It continually provides best practice recommended medicine, with all diagnostic and therapeutically possibilities, obtained by highly skilled personnel. All hospitalized patients from July 1, 2017 to July 31, 2024, excluding those in wash out period of COVID-19 pandemic (2019–2022) were reevaluated through sepsis criteria.
Sampling septic patients
Patients with clinical manifestation for infection prior hospitalization and with blood cultures obtained in the first 3 days of hospital stay were included in the analysis. All data were obtained from National Electronic Health Records—“Moj termin” and from patients’ medical charts. We analyzed patients’ demographics (gender and age) and comorbidities (diabetes, obstructive nephropathy malignant and non-malignant, hypertension, pre-existing chronic kidney disease (CKD)) data. Also, laboratory results, admission, and clinical features, especially those related with organ dysfunction variables for sepsis detection and gradation (body temperature, respiration and hearth rate, oxygen blood saturation, systolic blood pressure, neurological affection, white blood cells and platelets count, C-reactive protein, creatinine levels, inotrope usage), 12 were included in the analysis. Based on sepsis-3 criteria, patients with clinical suspicion of infection and ΔSOFA score ⩾2 were defined as sepsis and were included in the analysis. 11 Regarding clinical stage of sepsis patients were divided in three groups, sepsis, severe sepsis, and septic shock. 11 The primary entrance site was ratified by thorough evaluation of clinical observations, comorbidities, radiology findings, and microbiological data. A comparation of blood culture results regarding causative agents and multiple antibiotics resistance index (MAR) was performed in both periods. MAR index was calculated as the ratio of the number of antibiotics to which the isolated microorganism is resistant, to the total number of antibiotics to which the isolated microorganism was exposed. 13
Acute kidney injury
Serum creatinine levels were monitored during first 30 days from start of hospitalization, including those from the hospital discharge day. According to KDIGO* criteria patients were assessed for AKI and were classified accordingly in stages 1, 2, and 3. 13 Due to the insufficient data for urine output, the classification relied on increase of serum creatinine levels and patients with increase in serum creatinine of ⩾26.5 µmol/l or 1.5–1.9 times baseline creatinine were classified as stage 1, those with increase to 2.0–2.9 times from baseline as stage 2 or stage 3 with increase greater than three times baseline serum creatinine or a peak serum creatinine ⩾353.6 μmol/l or initiation of renal replacement therapy (RRT). 14 Some patents required transfer to intensive care unit and those hospitalizations were reviewed as one.
AKI outcome and need of replacement therapy, as well as 30-days survival were analyzed.
Outcomes
AKI outcomes and need of replacement therapy were notified. Recovery from AKI was defined as returning to baseline kidney function, which was estimated by the most frequent serum creatinine level from 90 to 365 days prior acute illness. 15 This was made in order to distinguish non-recovery AKI from pre-existing CKD. Also, we evaluated the number of patients that required renal replacement therapy during and after hospitalization (the one that did not recover kidney function). An analysis of mortality and 30-day survival was performed.
Statistical analysis
The patients were grouped as hospitalized in pre- and post-COVID-19 pandemic period. Continuous variables were expressed as mean with standard deviation (SD). An absolute number with percentage was used for presentation of nominal data. We performed a comparative analysis and used chi-square or Fisher exact test for the comparison of the categorical variables and Wilcoxon rank test or Student’s t-test for the numerical data. p < 0.05 was counted as significant. We conducted a time-to-event analysis for 30-day mortality using Cox proportional hazards regression. In order to present the impact of sepsis on outcome, we used hazard ratios (HRs), 95% CI, and Kaplan–Meier survival curves. SPSS statistical package version 21 was used for analysis.
MAR index was calculated for each causative agent isolated from blood cultures as the ratio of the number of antibiotics to which the isolated microorganism is resistant, to the total number of antibiotics to which the isolated microorganism was exposed and for their comparison a Kolmogorov–Smirnov one sample test was used performed.
Results
Periodic prevalence of sepsis
Out of 3801 hospitalizations, 50 (1.3%) in the pre-COVID-19 pandemic period and 94 (2.5%) from 3760 hospitalizations in the post-COVID-19 pandemic period, were diagnosed as sepsis, indicating twice higher prevalence of sepsis in the post-COVID-19 pandemic period, out of almost same number hospitalizations annually as it is demonstrated in the population chart flow diagram below (Figure 1).
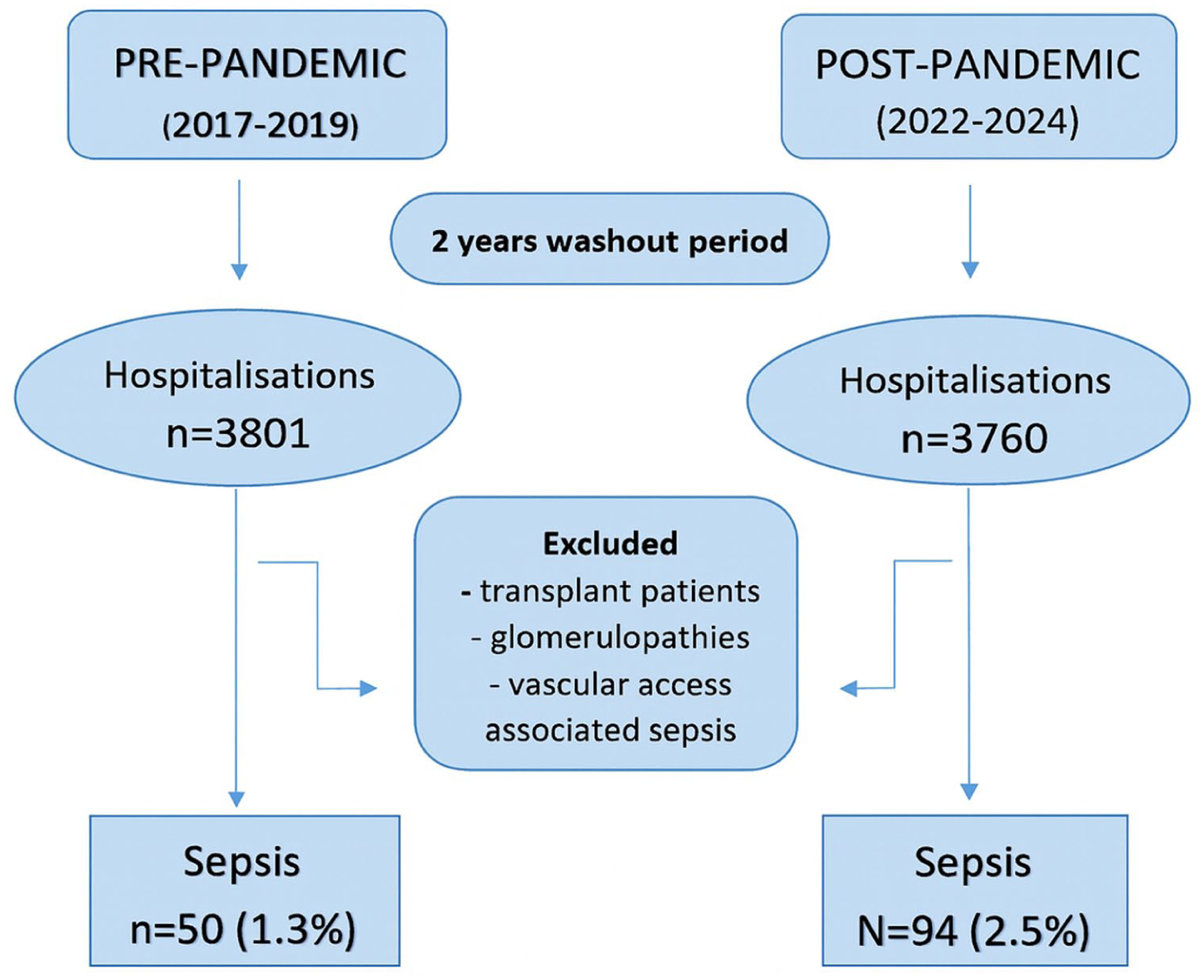
Flow diagram of the comparative analysis of demographics, clinical, and laboratory data between the two periods.
When the pre- and post-COVID-19 group were compared, no difference was found regarding the age, gender, diabetes, and hypertension (67.68 ± 11.43 vs 67.12 ± 11.54, p = 0.780; 25 (50%) vs 49 (52%), p = 0.946; 18 (36%) vs 42 (44%), p = 0.409; 34 (68%) vs 60 (63%), p = 0.752), respectively. According to sepsis staging, in the post-COVID-19 period there were more patients with septic shock (5 (10%) vs 23 (25%), p = 0.037), compared to pre-COVID-19 period, where the percentage of less severe sepsis was significantly higher (8 (16%) vs 2 (2%), p = 0.006), respectively. When all clinical features included in the sepsis staging were addressed separately, it was shown that in post-COVID-19 period there were more patients with lower blood saturation and mental status alteration (15 (28%) vs 48 (51%), p = 0.0014; 15 (30%) vs 66 (70%), p = 0.0001); respectively, also more patients had higher values of CRP (192.23 ± 91.70 vs 268.26 ± 12.38, p = 0.001) and required vasopressor and/or inotropes therapy more frequent (6 (12%) vs 30 (32%), p = 0.016), respectively. The overall number of patients with affection of two or more organ system was significantly higher in the post-COVID-19 period (26 (52%) vs 68 (72%), p = 0.025), as shown in Table 1.
Patients demographics, clinical, and laboratory data.
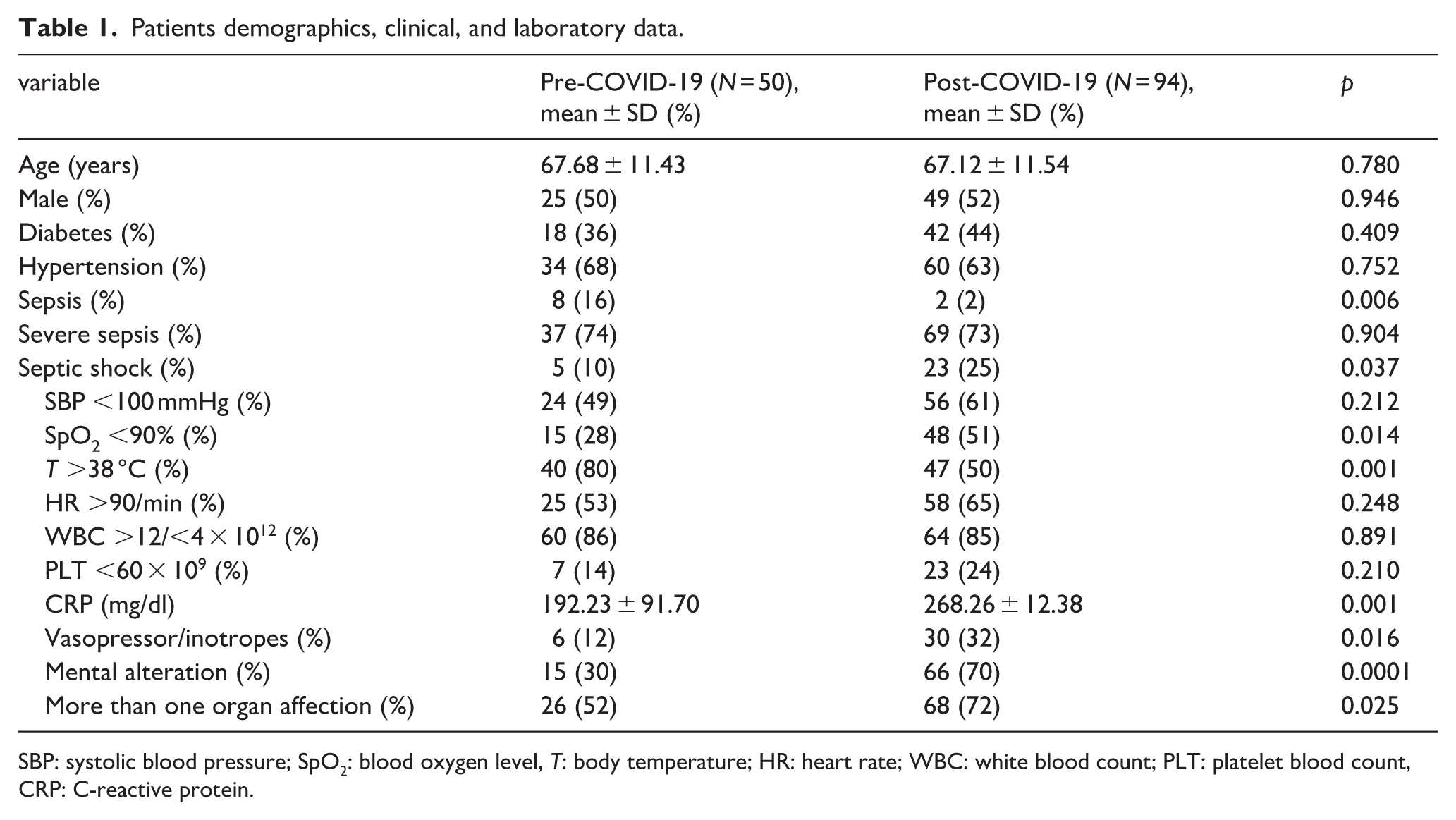
SBP: systolic blood pressure; SpO2: blood oxygen level, T: body temperature; HR: heart rate; WBC: white blood count; PLT: platelet blood count, CRP: C-reactive protein.
Kidney function affection and outcomes
Kidney function affection and outcomes are presented in Table 2. No difference was found regarding overall AKI incidence and pre-existing CKD between the two groups (94% vs 98%, p = 0.238; 60% vs 57%, p = 0.622), but there were more patients in the post-COVID-19 group with AKI stadium 3 (35 (70%) vs 79 (84%), p = 0.04) and more of them required renal replacement therapy (31 (62%) vs 74 (78%), p = 0.02).
Kidney function and outcomes.
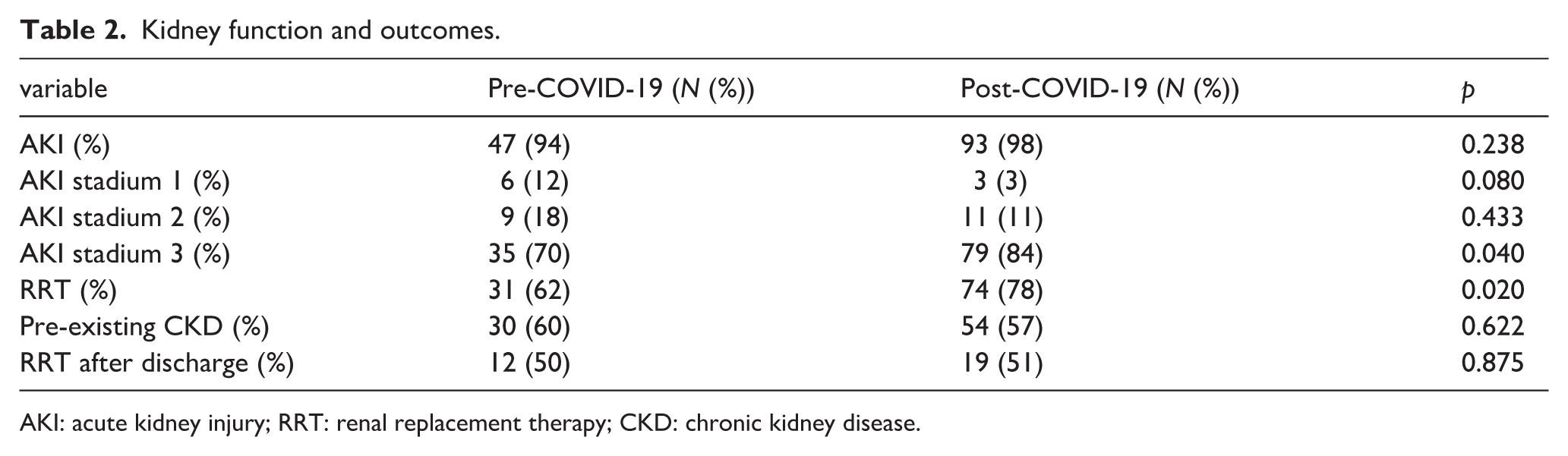
AKI: acute kidney injury; RRT: renal replacement therapy; CKD: chronic kidney disease.
The post pandemic period was endured by more clinically aggravated septic conditions as septic shock and increased severity of AKI with need of renal replacement therapy as in AKI stage 3 (Figure 2).
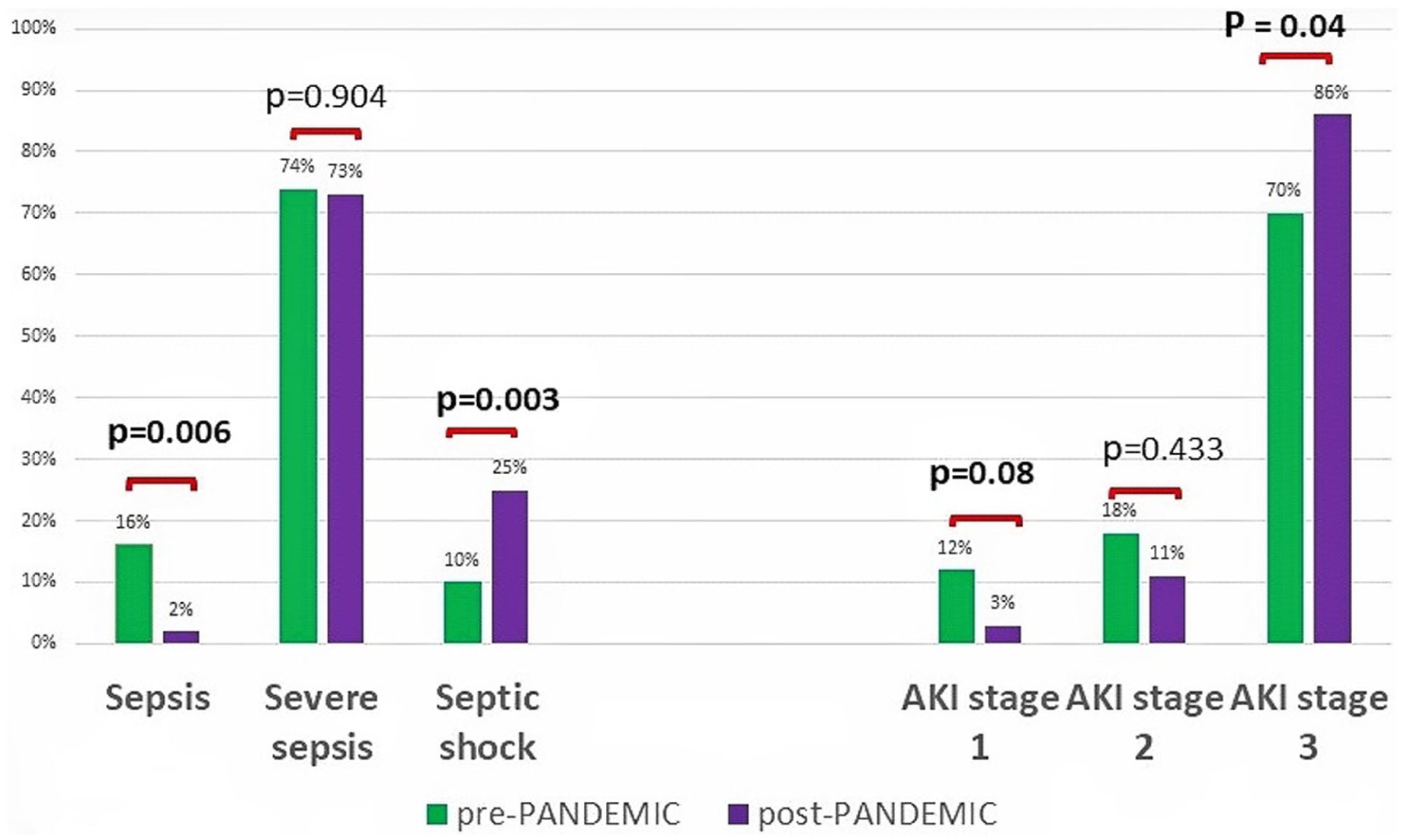
Sepsis and AKI staging before and after COVID-19 period.
The length of hospital stay of septic patients after COVID-19 was with significantly less duration than in the pre-COVID-19 period and those patients had also significantly shorter survival with death occurring almost twice more frequently (Table 3).
Hospital stay duration and survival.

Cumulative survival percentages at the 10th day were 33% higher pre pandemic (0.8 cumulative survival) in comparison to the post pandemic percentage (0.6 cumulative survival), as shown in Figure 3. Numerically, there was an extra death in every three patients post pandemic. Nearly half of patients did not survive at 20th day post pandemic and consistently remained <50% to the end of follow up. Overall, compared to the septic patients’ survival in the pre-pandemic period, there was a significantly shorter survival in post pandemic period, as shown in with Kaplan Meier analysis (log rank, p = 0.013). The Cox regression analysis confirmed 1.97 times higher risk of deaths in septic post pandemic patients (HR 1.977, 95% CI 1.127–3.469, p = 0.018).
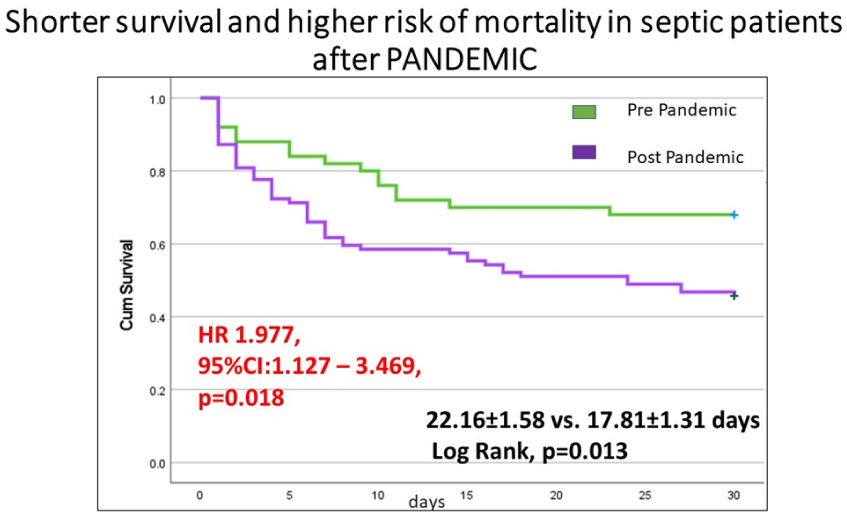
Kaplan–Meier survival curve illustrating shorter survival and higher mortality risk for patients with sepsis after the COVID-19 period.
Etiology of sepsis and multiple antibiotic resistance (MAR) indexing
Blood culture results were analyzed for the two periods. The number of positive blood cultures was around 70% and did not differ between the two groups (36 (72%) vs 52 (70%), p = 0.927). Regarding etiology of sepsis, the dominant door of entrance in both periods was the urinary tract (34 (68%) vs 57 (61%), p = 0.547), but the number of patients with obstructive nephropathy was significantly higher in the pre-pandemic group (31 (62%) vs 32 (34%), p = 0.001). When calculated the multiple antibiotics resistance (MAR) index in order to assess the association of the antibiotic resistance of the isolated causative agents of sepsis with the level of antibiotic use in analyzed periods, an important rise of MAR for Staphylococcus coagulase negative (0.48 vs 0.62, p = 0.001) and borderline rise for Escherichia coli (0.29 vs 0.35, p = 0.005) isolates in the post-pandemic group was noted (Table 4).
Blood cultures, causative agents, and MAR index.
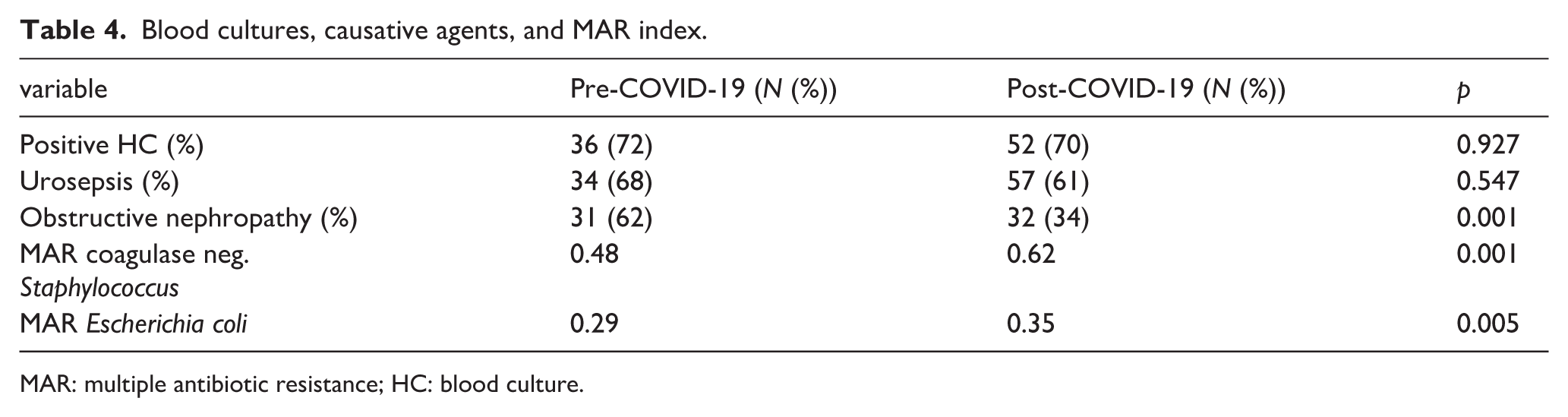
MAR: multiple antibiotic resistance; HC: blood culture.
Regarding causative agents, distribution was similar in both periods with slight increase in the percentage of patients with coagulase-negative Staphylococci after pandemic, evidence of appearance of Enterobacter cloacae and fungal septicemia in four patients in the post-pandemic period was observed (Figure 4(a) and (b)).
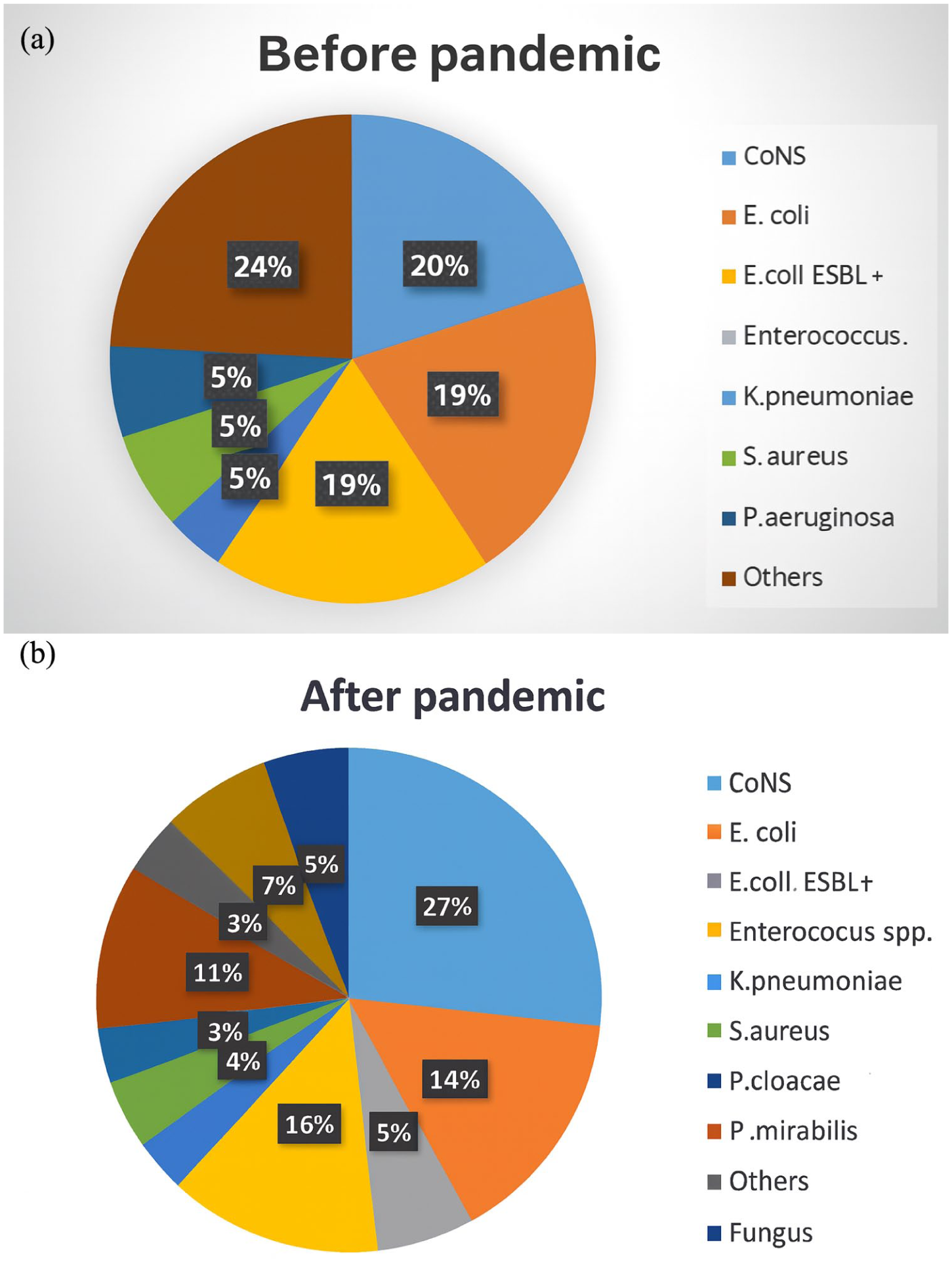
Causative agents in the (a) pre-pandemic period and (b) post-pandemic period.
Discussion
Our comparative analysis included 144 patients with sepsis and associated AKI. Almost all of them presented with AKI before admission, what was the reason for their initial hospitalization and treatment at our Nephrology Clinic. The number of patients with sepsis and associated AKI was twice higher in the post pandemic period which is consistent with the rising incidence of sepsis globally. 16 There are a lot of studies that analyze factors that are responsible for these higher numbers of patients diagnosed with sepsis and many of them implicate COVID-19 pandemic and its consequences as important contributing factor.17–20 COVID-19 pandemic did improve the awareness for prompt and early recognition of infection diseases and sepsis in general, but also permanently influenced our immunological systems and microbiological profile and distribution of the germs.18–20 Although there was no difference between the two groups regarding their comorbidities, age and gender, the clinical presentation and severity of sepsis and AKI itself was significantly worse in the post-COVID-19 group patients. Respectively, there were more patients with AKI stadium 3, septic shock, and multiorgan affection. Patients in the post-COVID-19 group also had higher values of inflammatory markers, so we assume that the well described long-lasting alterations of the immune system after COVID-19 infection, like immunosuppression and hyper inflammation with their consequent increase of susceptibility to bacterial and fungal infections can partly explain the incidence and severity of sepsis in the post pandemic period.19,20 Even though it did not reach statistical significance, it was evident that patients in the post pandemic group had lower platelets count. It is well known that platelets have important role in sepsis and many pathophysiological mechanisms can lead to low platelet count. 21 There are several published studies that suggest that the frequency of thrombocytopenia in sepsis may have been increased after pandemic.21–23 The exact cause of this is not well understood, but the post-COVID-19 immune dysregulation, long-term endothelial damage end residual effects of COVID-19-associated coagulopathy are numbered as possible significant contributing factors.21–23 Also, the vaccine-induced immune thrombocytopenia and thrombosis (VITT) linked to adenoviral vector in COVID-19 vaccines is recognized in some patients, although there is no strong evidence for a clinically relevant difference in VITT occurring after Ad26 or ChAdOx1. 24 Regardless of the underlying mechanism, thrombocytopenia is recognized as independent predictive factor for worse outcome and mortality from sepsis in general, which is consistent with the shorter survival observed in our post pandemic group, that presented with lower platelet values.25,26 Patients in the post pandemic group with sepsis had significantly shorter in-hospital stay and experienced death more often and this correlates with a multicentric German study where an observation of increased 30-day mortality from sepsis in hospitals in Germany, after the pandemic was analyzed. 27 One of the main cause for this was the impact that pandemic had on health care resources and capacities, public health policies, leading to delayed hospitalizations in more advanced and severe form of the disease. 28 In our analysis the risk of mortality was significantly higher for the post pandemic group and these is consistent with the excessive mortality rates observed in the post-pandemic period worldwide.28–31 Latest published study highlights the lasting mortality impact of pandemic among vulnerable populations, specifically in the older population, possibly due to the post-COVID-19 conditions and an excessive mortality after the pandemic due to cardiovascular events was reported in younger patients. 28 Also, there is a study from Japan that indicates that there are serious adverse effects after repetitive m-RNA vaccine against COVID-19 that could lead to increased morbidity and mortality after the pandemic. 29
Factors of limitation of our study were the small number of patients included in the study, the fact that it was a single center study, also the insufficient data for patients regarding their previous COVID-19 disease experience or vaccination, but it is certainly worth thinking about it and investigating in the future.
Beside not well understood contributing factors for this state, what is for sure is that a lot of studies and reports from national and international agencies document the persistence of this phenomenon of long-lasting excessive mortality in a lot of countries and according to the report of Swiss Re institute report it’s predicted that the excess mortality will gradually tail off by 2033.30–32
In order to understand the rising prevalence, severity, and increased mortality from sepsis in the post- pandemic period we compared blood culture isolates between the two periods. A positive isolate was obtained in around 70% of study population with sepsis and 30% had negative blood cultures, with almost equal distribution between the two periods. This percentage is in line with numbers in studies that demonstrate that the proportion of negative blood cultures in septic patients ranges from 28% to 49%33,34 and this is partly explained by the fact that some of them were previously treated with antibiotics in local medical centers and they got sterile results on the analysis. The urinary tract remained dominant door of entrance in both periods, but in less number of cases in the post pandemic period was complication of an obstructive nephropathy. When we addressed the most common isolated causative agents and their MAR indexes, we did find increased index of antibiotic resistance for coagulase-negative Staphylococcus and Escherichia coli. A MAR index of 0.2 or greater suggests association with high antibiotic use. These corresponds with recent published literature that emphasizes the importance of the rising trends od multidrug resistance of some bacteria as a result of the antibiotics overuse during the COVID-19 pandemic and its impact on incidence and course of infection diseases in general.35–37 What was also of big significance for our study was the occurrence of fungal sepsis only in the post pandemic period, indicating more immunocompromised state of the patients in these group as a result of the numerous direct and indirect effects of the virus itself. Centers for Disease Control and Prevention (CDC) reports from 2022 determined that COVID 19 did create a perfect storm by increasing antibiotic-resistant infections and death in hospital for 15%, putting an alert for potential new epidemic on the rise. 38
Conclusion
Sepsis and associated AKI occurrence and mortality are significantly higher in the post-COVID-19 pandemic period. The increased multidrug resistance of causing microorganisms is evidential, and provides some of the explanation for to the rising incidence and mortality of sepsis. Further studies on larger groups of patients are needed to evaluate additional contributing factors to this state, to upgrade our knowledge and expertise in early recognizing and management with this alarm condition and by that improve quality of care and survival from sepsis in general.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.