
Abstract
Introduction:
Aortic dissection is characterized by an intimal tear resulting in blood flowing into the aortic media, creating a false lumen along the aorta. In acute type A aortic dissection surgery, grafts are used for ascending aortic replacement.
Methods:
This retrospective study examined 113 patients who underwent surgery for type A aortic dissection at the Cardiovascular Surgery Clinic of Konya City Hospital between December 2020 and October 2025. After exclusion criteria, 62 patients were included in the study. The cut-off point for graft area was based on the median value of the dataset, which is 6120 mm2. Patients were divided into two groups: those with a graft area >6120 mm2 and those with a graft area ⩽6120 mm2.
Results:
The findings suggest that larger graft areas may be associated with a more pronounced postoperative inflammatory response, reflected in increased leukocyte subtypes and inflammatory markers; while the decreases in hemoglobin and hematocrit observed in smaller graft areas may suggest different perioperative physiological or hemodilution mechanisms.
Conclusion:
These findings are consistent with the literature supporting the central role of systemic inflammation in the postoperative pathophysiology of cardiac surgery and point to the potential clinical significance of integrating graft-size-dependent inflammatory responses into perioperative risk stratification and patient management. However, well-designed prospective studies are needed to clarify the causal relationship and determine the impact of interventions targeting postoperative inflammation on clinical outcomes.
Keywords
Introduction
Aortic dissection is defined as blood flow into the media of the aorta due to an intimal tear of the aorta, resulting in a pseudo-aortic lumen along the long axis of the aorta. 1 There are two classification methods for aortic dissection: the DeBakey and Stanford classifications. Stanford type A aortic dissection involves the ascending aorta or the total aorta. 2 Acute type A aortic dissection is a disease with a high mortality risk. According to the findings of the International Registry of Acute Aortic Dissections (IRAD), the mortality of surgically treated patients ranges from 18% to 25%. Despite recent advances in perioperative strategies, acute type A aortic dissection remains a serious aortic disorder. 3 The results of some studies in the literature have shown that the patient’s age, white blood cell count, preoperative neutrophil–lymphocyte ratio (NLR), plasma D-dimer level, platelet count, and C-reactive protein (CRP) are determinants of mortality in patients. 4 Aortic grafts are used for ascending aortic replacement in acute type A aortic dissection surgery. Aortic grafts used in current clinical practice are made of woven or mesh-structured Dacron (polyester) material, with the inner surface impregnated with bovine collagen or gelatin to reduce blood leakage. 5 Aortic graft replacement is generally associated with an inflammatory response. 6 One of the possible mechanisms of the inflammatory response may be an immune reaction to the collagen and gelatin used in the impregnation of the grafts. In addition, it is thought that endotoxins, which can be found as contaminants in grafts coated with bovine collagen and gelatin, may also play a role in the development of inflammation. 7 The aim of this retrospective study is to examine the effect of graft size on inflammation markers and clinical outcomes in patients who underwent aortic graft implantation due to acute Type A aortic dissection. To our knowledge, this topic has not been previously reported in the literature.
Materials and methods
This retrospective study examined 113 patients who underwent surgery for type A aortic dissection at the Cardiovascular Surgery Clinic of Konya City Hospital between December 2020 and October 2025. Exclusion criteria included the simultaneous use of different graft materials in the same patient, hybrid procedures combining endovascular and open surgical methods, and a history of previous surgery or major trauma within 30 days prior to the procedure. Patients with missing body temperature or C-reactive protein (CRP) data, as well as those with postoperative complications that could affect inflammatory markers such as urinary tract infection, pneumonia, atelectasis, and hematoma, were excluded from the study. In addition, patients who experienced in-hospital mortality were also considered within the scope of the exclusion criteria. After the exclusion criteria, 62 patients were included in the study. Collected patient data included demographic characteristics (e.g. gender, age, body mass index), medical history (e.g. hypertension, diabetes mellitus, chronic obstructive pulmonary disease, cerebrovascular events, peripheral artery disease, chronic kidney disease, liver disease, atrial fibrillation, hyperlipidemia), preoperative and postoperative laboratory findings, preoperative and postoperative computed tomography findings, preoperative and postoperative echocardiography findings, postoperative fever monitoring, and surgical notes. All data were collected from clinical records and electronic hospital databases.
Patients underwent surgical procedures for type A aortic dissection following standard techniques. Demographic, clinical, laboratory, and imaging characteristics of the patients were analyzed. Patients’ laboratory values immediately before surgery and at 48 h postoperatively were evaluated. The rate of postoperative atrial fibrillation during hospital admission was assessed. Postoperative fever was defined as a fever ⩾38 °C occurring within the first 1–3 days after surgery. The relationships between the graft area used during surgery and the data were statistically compared. The lateral area of the aortic graft used was calculated using the formula 2πrh, where π was considered to be 3. The median value, representing the central tendency of the dataset, was used to determine the cut-off point for the graft area. This approach created an objective threshold for classification by dividing the data into two equal groups. The cut-off point for the graft area was based on the median value of the dataset, which was 6120 mm2. Patients were divided into two groups: those with a graft area >6120 mm2 and those with a graft area ⩽6120 mm2. The primary endpoint of the study was the relationship between the amount of graft used during surgery and postoperative laboratory values and clinical outcomes.
Statistical analysis
Research data were evaluated using the SPSS 27.0 statistical program. The normality of the distribution of continuous variables was investigated using visual (histogram and probability plots) and analytical methods (Kolmogorov–Smirnov/Shapiro–Wilk tests). Descriptive statistics of the research were presented using number (n), percentage (%), mean, standard deviation (SD), median, minimum, and maximum. The chi-square test was used to show whether there was a difference between categorical variables in the research. Student’s t-test was used to compare continuous variables with parametric properties in independent groups, Mann–Whitney U test was used to compare continuous variables without parametric properties in independent groups, dependent groups t-test was used to compare continuous variables with parametric properties in dependent groups, and Wilcoxon test was used to compare continuous variables without parametric properties in dependent groups. For statistical significance, the p value was found to be <0.05.
Ethical considerations
Ethical approval for this study was obtained from the Non-Interventional Clinical Research Ethics Committee of Konya City Hospital (approval date: August 12, 2025; approval number: 2025/235).
Surgical intervention
Patients diagnosed with acute type A aortic dissection were urgently prepared for surgery. Surgical strategies were determined preoperatively using clinical data and imaging methods. Patients underwent endotracheal intubation under general anesthesia, followed by arterial cannulation via the right axillary artery and/or femoral artery. Right atrial venous cannulation was performed after sternotomy. Cardiopulmonary bypass (CPB) was initiated when the active clotting time exceeded 480 s after appropriate heparin administration. After cross-clamping, the heart was stopped using modified Del-Nido cardioplegia at a dose of 20 mL/kg at 5 °C. CPB was stopped when the hypothermic circulation stopping temperature of 22 °C–24 °C was reached. Cerebral tissue was perfused with selective cerebral perfusion. For distal aortic repair, one of the following options was performed: total aortic arch replacement with frozen elephant trunk, ascending aortic replacement + half-arch replacement, or ascending aortic replacement alone, depending on the patient’s needs. Master Series™ Aortic Valved Graft was used in patients with indications for aortic valve replacement. FlowWeave Bioseal® vascular grafts were used in patients not requiring aortic valve replacement. CPB was restarted, and systemic temperature reached 32 °C–34 °C. During this time, one of the following procedures suitable for proximal aortic treatment was performed: ascending aortic replacement, Bentall procedure, or Wheat procedure.
Post-surgical observation
Patients’ blood pressure, heart rhythm, laboratory results, and oxygen saturation were monitored in the intensive care unit. Patients were generally extubated within the first 12 h after surgery. Emergency treatment was planned for patients who developed complications. Patients were transferred to the ward for observation once their general condition stabilized. Discharge was planned for patients whose general condition remained stable during ward observation.
Results
A total of 62 patients were included in the study. The cut-off point for graft area was based on the median value of the dataset, which was 6120 mm2. Patients were divided into two groups: those with a graft area >6120 mm2 and those with a graft area ⩽6120 mm2.
Table 1 summarizes the demographic and clinical characteristics according to graft area. The frequency of aortic valve replacement was significantly higher in patients with a graft area >6120 mm2 compared to those with a graft area ⩽6120 mm2. In addition, postoperative fever was significantly more frequent in the >6120 mm2 group. No statistically significant differences were observed between the groups in terms of gender, age, diabetes mellitus, hypertension, hyperlipidemia, chronic obstructive pulmonary disease/asthma, smoking status, or the occurrence of postoperative atrial fibrillation (AF; all p > 0.05).
Demographic and clinical characteristics according to graft area.
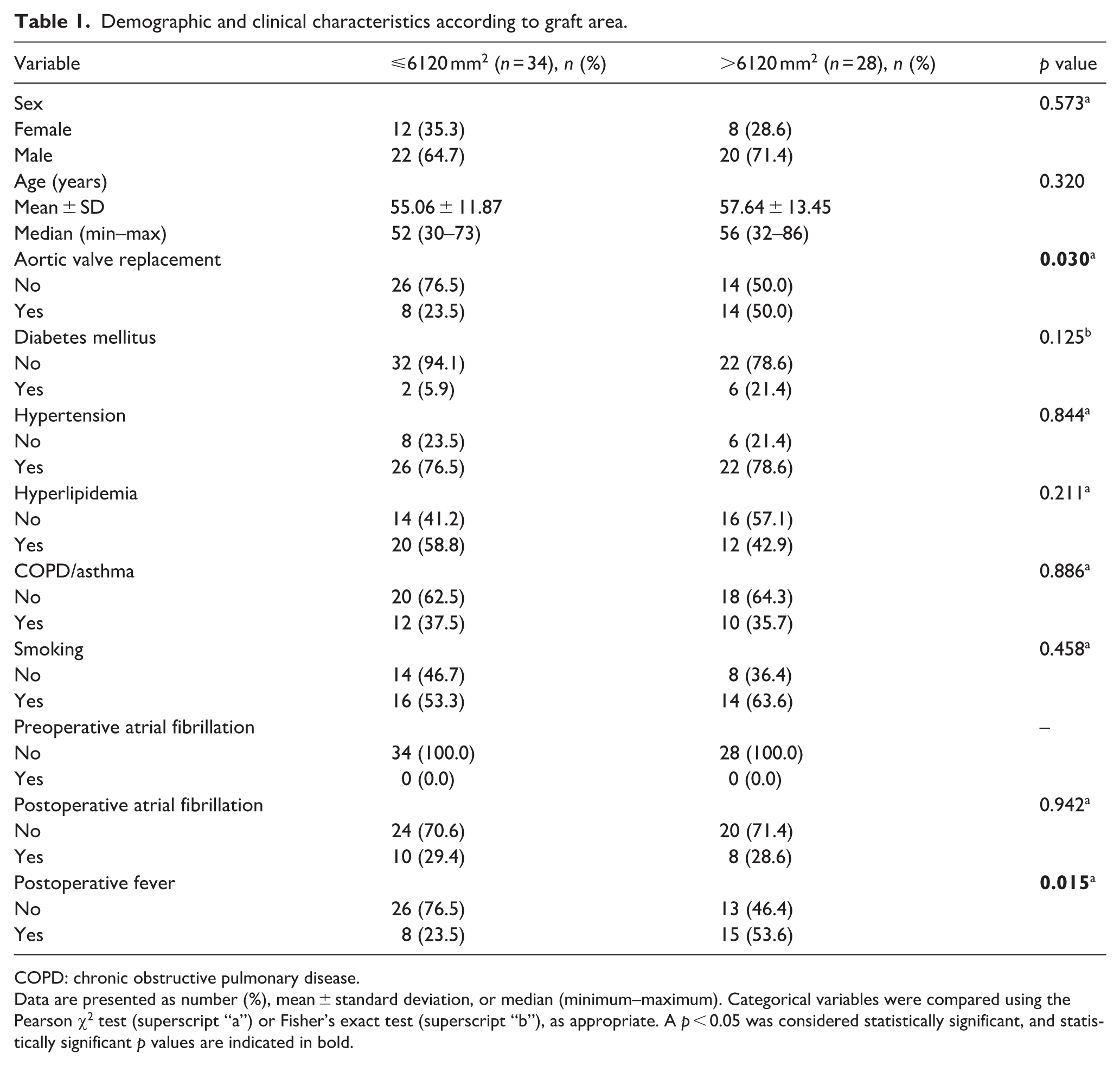
COPD: chronic obstructive pulmonary disease.
Data are presented as number (%), mean ± standard deviation, or median (minimum–maximum). Categorical variables were compared using the Pearson χ2 test (superscript “a”) or Fisher’s exact test (superscript “b”), as appropriate. A p < 0.05 was considered statistically significant, and statistically significant p values are indicated in bold.
As shown in Table 2, patients with graft area >6120 mm2 had significantly higher postoperative lymphocyte count, C-reactive protein, erythrocyte sedimentation rate, and D-dimer levels, while patients with graft area ⩽6120 mm2 had significantly lower postoperative glomerular filtration rate; no significant differences were observed between the groups in terms of other postoperative laboratory parameters or ejection fraction. Changes in laboratory parameters according to graft area are presented in Table 3. Compared to patients with graft area ⩽6120 mm2, significantly larger changes were observed in white blood cell count, lymphocyte count, neutrophil count, C-reactive protein, erythrocyte sedimentation rate, and D-dimer levels in patients with graft area >6120 mm2; conversely, changes in hemoglobin and hematocrit values were significantly more pronounced in the ⩽6120 mm2 group. No significant differences were observed between groups in changes in platelet count, procalcitonin, international normalized ratio, troponin, neutrophil-lymphocyte ratio, creatinine, or glomerular filtration rate (all p > 0.05).
Postoperative laboratory and clinical parameters according to graft area.
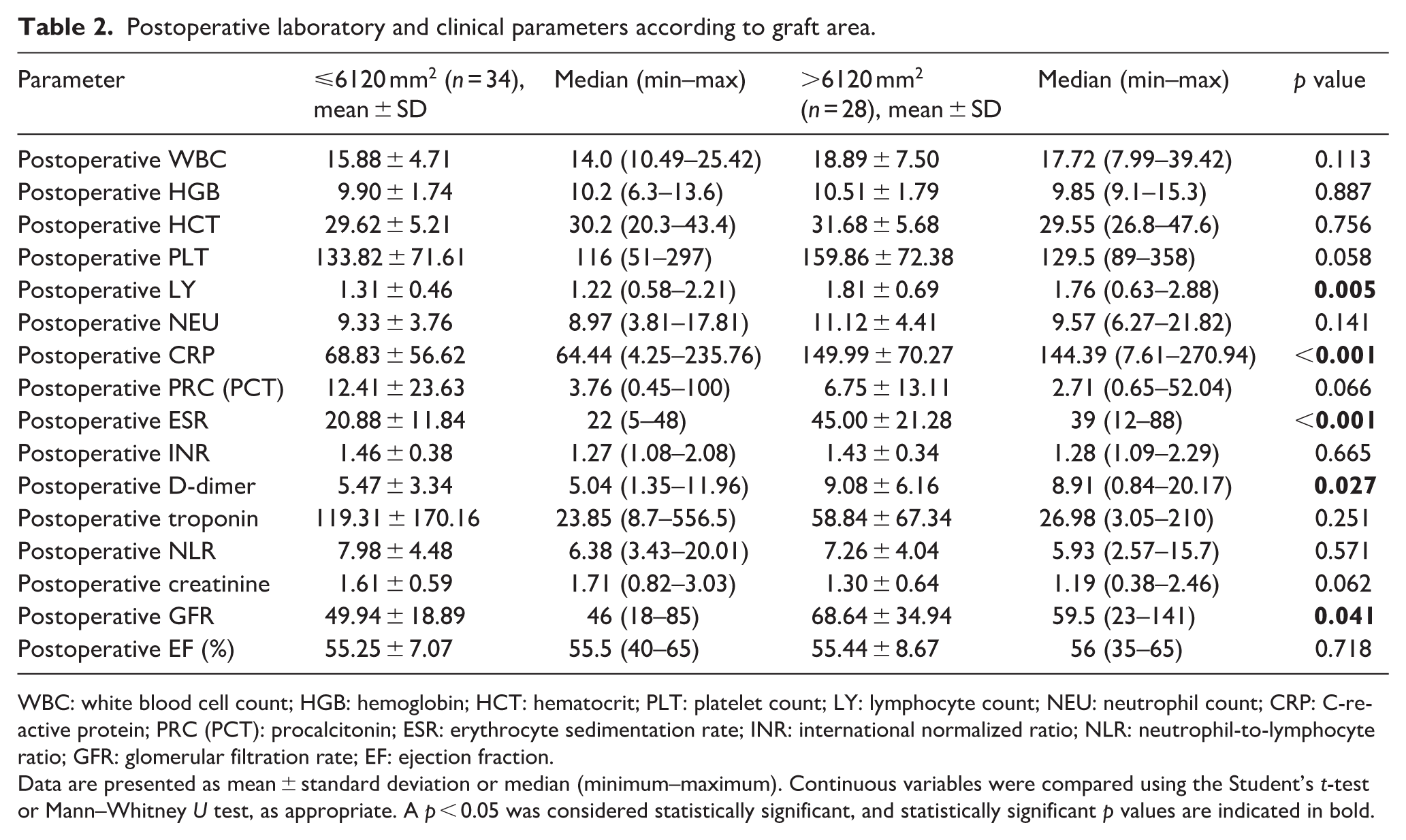
WBC: white blood cell count; HGB: hemoglobin; HCT: hematocrit; PLT: platelet count; LY: lymphocyte count; NEU: neutrophil count; CRP: C-reactive protein; PRC (PCT): procalcitonin; ESR: erythrocyte sedimentation rate; INR: international normalized ratio; NLR: neutrophil-to-lymphocyte ratio; GFR: glomerular filtration rate; EF: ejection fraction.
Data are presented as mean ± standard deviation or median (minimum–maximum). Continuous variables were compared using the Student’s t-test or Mann–Whitney U test, as appropriate. A p < 0.05 was considered statistically significant, and statistically significant p values are indicated in bold.
Comparison of laboratory parameter changes according to graft area.
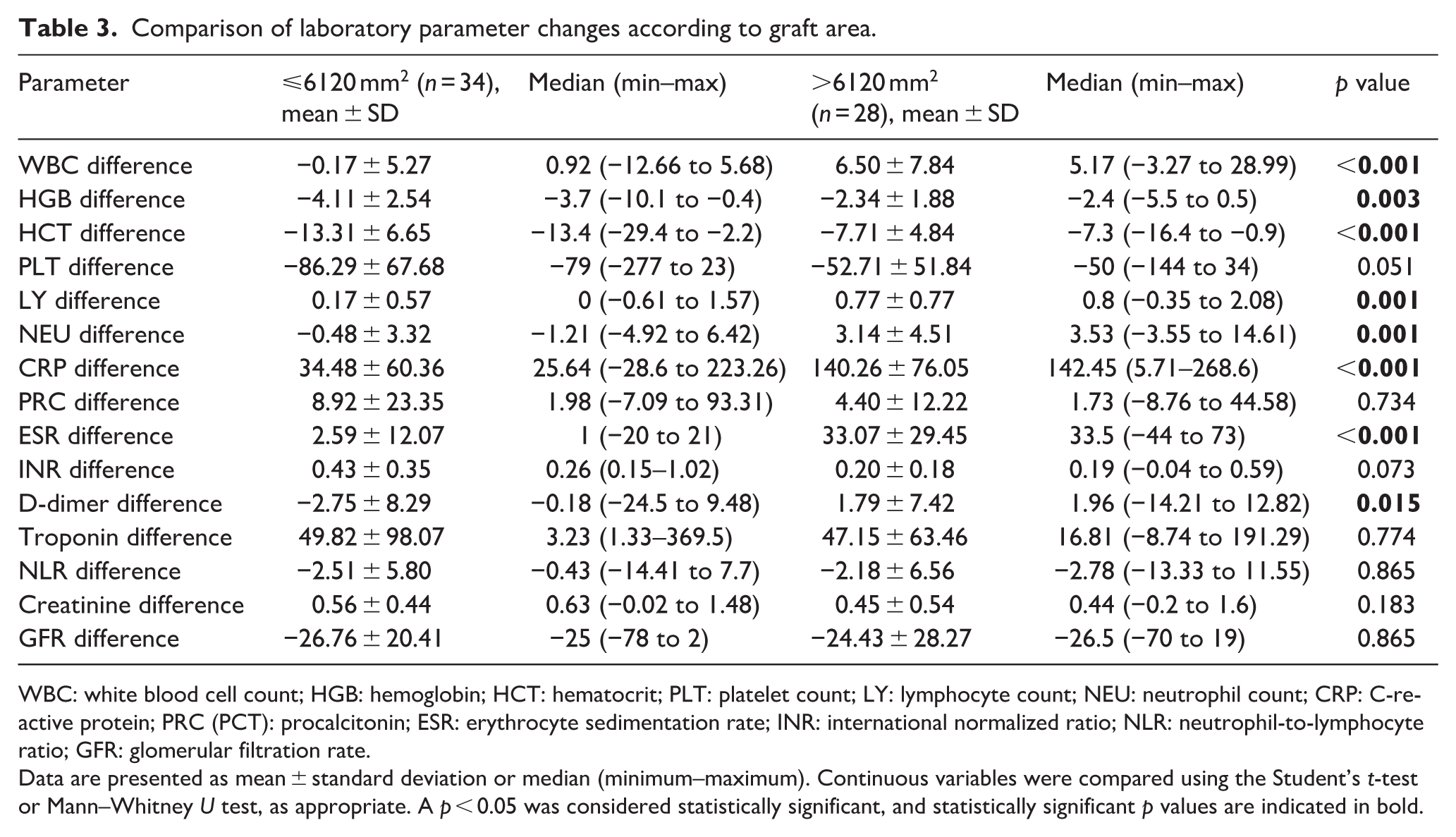
WBC: white blood cell count; HGB: hemoglobin; HCT: hematocrit; PLT: platelet count; LY: lymphocyte count; NEU: neutrophil count; CRP: C-reactive protein; PRC (PCT): procalcitonin; ESR: erythrocyte sedimentation rate; INR: international normalized ratio; NLR: neutrophil-to-lymphocyte ratio; GFR: glomerular filtration rate.
Data are presented as mean ± standard deviation or median (minimum–maximum). Continuous variables were compared using the Student’s t-test or Mann–Whitney U test, as appropriate. A p < 0.05 was considered statistically significant, and statistically significant p values are indicated in bold.
These findings suggest that larger graft areas may be associated with a more pronounced postoperative inflammatory response, as reflected in greater changes in leukocyte subtypes and inflammatory markers, while the greater decreases in hemoglobin and hematocrit values observed in patients with smaller graft areas may indicate different perioperative physiological or hemodilution effects. Together, these patterns highlight the potential impact of graft size on postoperative systemic response and may have important implications for perioperative monitoring and risk stratification.
Discussion
The main topic of this study was the relationship between aortic graft area and postoperative laboratory values and clinical findings.
In this study, a more pronounced inflammatory profile was observed in patients with larger graft areas, as evidenced by a higher frequency of postoperative fever and greater changes in leukocyte subtypes, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR), and D-dimer levels. Postoperative fever is a common occurrence after cardiac surgery and is explained by a sterile inflammatory response associated with surgical trauma and cardiopulmonary bypass rather than infection, especially in the early postoperative period; this highlights the role of inflammation in the postoperative clinical course. 8 Due to the significant heterogeneity in patient selection and study methodologies, 9 it is difficult to directly compare the findings of some studies with previous studies examining the development of postoperative fever. However, the relatively broad exclusion criteria in the present study and the inclusion of a patient group without mortality or major complications in the analysis ensured that the results were obtained from a more realistic population reflecting clinical practice and increased the value of the study.
The frequency of aortic valve replacement was significantly higher in patients with larger graft areas, and the change in CRP levels was more pronounced in the group with graft area >6120 mm2. The literature reports that high postoperative CRP levels may be associated with a more negative improvement in cardiac function after valve replacement. 10 However, in the present study, despite increased inflammatory response indicators, no statistically significant difference indicating a worse improvement in cardiac function was found. This suggests that although a systemic inflammatory response is evident, its clinical expression may differ from the typical postoperative inflammatory syndrome described in the literature.
In recent years, it has become increasingly widely accepted that inflammatory markers play a critical role in the pathogenesis and progression of atrial fibrillation (AF). 11 In our present study, although statistically significant differences were found between the groups in terms of some inflammatory biomarkers, no significant difference was observed between the groups in terms of the development of postoperative atrial fibrillation. This finding suggests that multiple pathophysiological mechanisms, in addition to the inflammatory process, play a role in the development of AF.
Elevated levels of CRP and other inflammatory markers after cardiac surgery have been repeatedly documented and associated with adverse clinical outcomes, suggesting that systemic inflammation contributes to postoperative morbidity. 12 Although the elevations in CRP and other inflammatory markers were significant in the patient group in the current study, the patient groups consisted of patients without major morbidity and mortality.
Fever and elevated CRP levels can also be seen in cases of non-infectious aortitis. 13 However, this condition is usually associated with systemic inflammatory diseases such as Takayasu arteritis, giant cell arteritis, rheumatoid arthritis, systemic lupus erythematosus, Behçet’s disease, or immunoglobulin G4-associated disease, and usually presents with clinical manifestations extending beyond the aorta. 14 Definitive diagnosis of non-infectious aortitis usually requires histopathological evaluation of surgical specimens. 15 In this study, although fever and elevated CRP levels were observed in some patients, no concomitant systemic inflammatory disorder suggestive of non-infectious aortitis was detected, and no repeated surgical intervention was performed for pathological confirmation. Therefore, non-infectious aortitis was not considered a possible explanation for the inflammatory findings in our cohort.
Finally, previous studies have reported that up to 74% of patients develop non-infectious inflammatory signs after aortic graft replacement surgery, most commonly presenting with fever, fatigue, elevated CRP levels, and periprosthetic fluid accumulation. 16 In the present study, patients—particularly those with larger graft areas—showed significantly higher rates of fever and elevation of CRP and other inflammatory markers; however, no evidence of periprosthetic effusion was detected. This suggests that, although a systemic inflammatory response is evident, its clinical expression may differ from the typical postoperative inflammatory syndrome described in the literature.
Limitations
This study has several limitations. Firstly, the retrospective design of the study restricts the evaluation of causal relationships, and more comprehensive, prospectively planned studies are needed to confirm the findings. Furthermore, since postoperative laboratory parameters can be affected by many non-surgical factors, this may complicate the interpretation of the results. In addition, the fact that the study was conducted in a single center and included a relatively limited number of patients reduces generalizability. Further studies with longer follow-up periods, in multiple centers, and with larger sample sizes are needed.
Conclusion
These findings are consistent with the existing literature indicating that systemic inflammation plays a central role in the postoperative pathophysiology following cardiac surgery, and highlight the potential clinical significance of integrating graft-size-dependent inflammatory responses into perioperative risk stratification and patient management strategies. However, prospective, well-designed studies are needed to more clearly elucidate the causal aspect of this relationship and to evaluate whether specific interventions targeting postoperative inflammation can improve clinical outcomes.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.