
Abstract
High-pressure excursions (HPE) during cardiopulmonary bypass (CPB) are rare but potentially life-threatening events linked to coagulation activation, inflammation. Known risk factors include male sex, large body surface area (BSA), elevated hematocrit (Htc), prior stroke and urgent surgery. Recommended management follows a stepwise approach involving haemodilution, heparin and antithrombin (AT), albumin or epoprostenol depending on Htc and pressure thresholds. We report a 69-year-old man undergoing urgent complex cardiac surgery who developed rising pre-oxygenator pressures 10 min after CPB initiation. Despite initial haemodilution and AT, pressures improved only partially. Administration of 100 mL of 20% albumin led to rapid normalization of pre-oxygenator and delta pressures, allowing safe continuation of CPB. The postoperative course was uneventful. Subsequent review of the oxygenator transmembrane resistance (R) showed a progressive decline following the administration of AT and albumin. This case suggests that AT, administered alongside albumin, may reduce blood viscosity and improve oxygenator performance. Further research is needed to clarify mechanisms and standardize management of HPE during CPB.
Keywords
Introduction
High-pressure excursions (HPE) during cardiopulmonary bypass (CPB) are uncommon yet critical events that may impair oxygenation and require an emergency replacement of oxygenator. 1 The HPE underlying mechanisms during CPB are hypothesized to be the triggering of the inflammatory response, the coagulation cascade and platelet–leukocyte aggregation.2,3 Incidence of HPE ranges between 0.4% and 2.3% in various studies. 4 The risk factors most frequently associated with HPE include male sex, large body surface area (BSA), hematocrit (Htc) levels above 28% during CPB, a history of previous stroke and urgent or emergency surgery. 4 The treatment protocol to manage transient increases in oxygenator inlet pressure follows a stepwise approach. Initial measures include administration of heparin, with additional AT if the activated clotting time (ACT) is <480 s. If pre-oxygenator pressure remains >500 mmHg with Htc >28%, haemodilution with crystalloids and albumin is recommended; instead, if pre-oxygenator pressure exceeds 500 mmHg with Htc <28%, administration of epoprostenol is indicated. 4
Case report
Written informed consent was obtained from the patient for publication of this case report. A 69-year-old man had been planned to undergo urgent combined coronary artery bypass grafting and a biological aortic valve replacement. A preoperative evaluation showed that the patient has hypertension, is an active smoker with no symptoms of heart failure and has chronic coronary artery disease. His BSA was 2.3 m2, and haemoglobin and coagulation parameters were within normal range: WBC 10.70 × 109/L, RBC 4.59 × 1012/L, haemoglobin (Hb) 14.5 g/dL, Htc 43.3%, platelets count (Plt) 232 × 109/L, INR 1.0, aPTT 37.3 s, fibrinogen 449 mg/dL, antithrombin 106%. General anesthesia was induced with midazolam 6 mg, sufentanil 40 µg and rocuronium 80 mg. Afterward totally intravenous anesthesia with propofol and remifentanil was administered and monitored using processed electroencephalography. An initial loading dose of tranexamic acid (10 mg/kg) was administered prior to the start of surgery, followed by a continuous infusion of 2 mg/kg/h in accordance with the local standard protocol. The patients received 2 g of cefazolin as antibiotic prophylaxis. After median sternotomy, systemic heparinization was achieved with 350 IU/kg of unfractionated heparin to obtain a target ACT of ⩾480 s.
As the initial ACT measured with Hemocron® signature elite (Accriva, San Diego, CA, USA) was marginally sub-therapeutic (460 s), an additional bolus of unfractionated heparin (5000 IU) was given prior to initiating CPB. Thereafter, ACT remained above 480 s throughout the CPB run as reported in Supplemental Table 1. Subsequently, normothermic (36 °C) CPB was initiated using a standard roller-pump heart–lung machine Stöckert S5 (LivaNova®, London, UK) equipped with an Inspire 8 F oxygenator (LivaNova®, London, UK), Maquet Heater Cooler Unit 40 (Getinge®, Göteborg, Sweden) and a Medex LogiCal pressure monitoring system (Smith Medical, Plymouth, MN, USA). All disposables were coated with the P.h.i.s.i.o. coating (LivaNova). Target blood flow was set at 5.5 L/min (2.4 L/min/m2). Five minutes after the initiation of CPB, Custodiol® (NC, USA) cardioplegia was administered over an 8-min period and drained from the coronary sinus using an external suction system rather than into the CPB reservoir.
Approximately 20 min following the onset of CPB, the perfusionist noted a disproportional rise of pre-oxygenator pressure in comparison with pump flow and temperature. The pre-oxygenator pressure was nearing 400 mmHg at that period and 25 min later, the pre-oxygenator pressure reached 500 mmHg, the trigger point for intervention. The patient had at that time an Htc of 32%, thus haemodilution with crystalloids was initiated. This intervention was not successful, and therefore the perfusionist alerted the anesthesiologist, who ordered to drain 1 L of blood from the venous reservoir and continue crystalloid haemodilution to an HTC of 28%. In addition to haemodilution, 500 IU of AT was administered, although ACT was >480 s. Approximately 10 min later, the pre-oxygenator pressure had fallen below 500 mmHg, but full calculated CPB flow could not be achieved. Thus, a 100 mL bolus of 20% human serum albumin was provided. Ten minutes after that, the cross-clamp was removed and pre-oxygenator pressures were restored to normal.
The aspirated blood was reinfused and further reperfusion and weaning from CPB proceeded uneventful. There was adequate surgical haemostasis with mild diffuse bleeding that cleared off spontaneously. Intraoperative diuresis was maintained. There were no foci of neurologic deficit on awakening. There was no acute kidney injury (AKI) after operation. The patient required one packed red blood cell transfusion during the hospitalization. On postoperative day 16, the patient was discharged after the bilateral pleural effusions had resolved and progressive mobilization had been achieved.
Discussion
HPE during CPB despite adequate anticoagulation represents an uncommon but potentially hazardous event due to the risk of oxygenator failure and the catastrophic nature of an emergent oxygenator change-out. 3 This case illustrates the presentation and management of an HPE event in a modern coated oxygenator,2,5 consistent in several aspects with the patterns described by Hjärpe et al. 4 The patient had several characteristics that were associated with an increased risk of HPE, including a large BSA, a higher Htc level during CPB and a complex combined procedure. The slow increase in oxygenator pressures (Supplemental Figure 2) shortly after the onset of aortic cross-clamping is characteristic of type II HPE, 4 where platelet activation, leukocyte adhesion and shear-mediated aggregation appear to contribute to rapid elevations in transmembrane pressure. At the time of this event, institutional protocols for managing HPE were undergoing revision at our centre. For this reason, management of HPE proceeded via empirical escalation. Initial interventions targeted aggressive haemodilution; ~1 L of whole blood was sequestered from the venous reservoir and replaced with crystalloid. Following a suboptimal response – and despite maintaining therapeutic ACT – functional AT deficiency was suspected. Consequently, 500 IU of AT was administered to augment heparin sensitivity, consistent with ERAS society recommendations. 6 Exogenous albumin was subsequently administered as a rescue adjunct to optimize plasma oncotic pressure and rheological flow, as it is not a constituent of our standard circuit priming.
The reduction in oxygenator transmembrane pressures achieved with these maneuvers eliminated the need for epoprostenol, which was reserved as a tertiary rescue measure in light of its slightly elevated bleeding risk7,8 and the need for an emergent oxygenator exchange.
Role of haemodilution
Haemodilution represents the first-line intervention in most HPE management protocols because lowering Htc reduces blood viscosity and platelet margination. 9 Hjärpe et al. showed that Htc during CPB was independently associated with HPE risk, with each percentage increase raising odds by 20%. 4 Nonetheless, in our case, haemodilution did not consistently mitigate HPE or the transmembrane oxygenator resistance noted on subsequent review (Figure 1), presumably because the pathophysiologic process leading to HPE was initiated early during CPB 10 and was not amenable to reversal by haemodilution. 11 It remains unclear whether the induction of haemodilution is a prerequisite for the effectiveness of other pharmacologic interventions or whether, in highly urgent situations, it may instead delay the timely administration of targeted therapies against HPE.
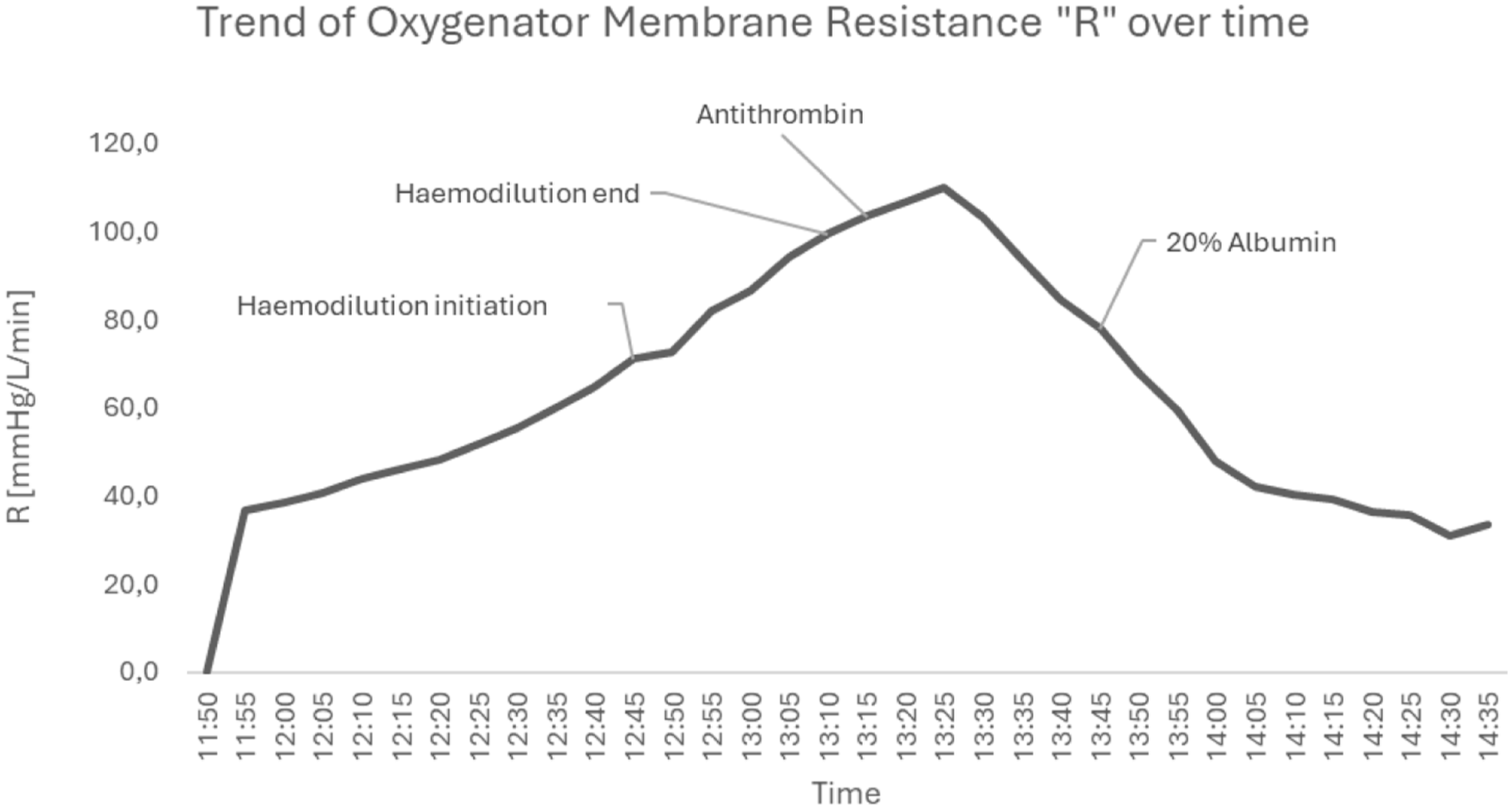
Oxygenator membrane resistance (R) plotted over time, demonstrating a parallel transmembrane oxygenator pressures and resistance rise decreasing after antithrombin and 20% albumin administration.
Role of antithrombin
The underlying mechanism of HPE is still uncertain, although involvement of platelets has been suggested.2,4,11,12 Antithrombin is crucial for achieving adequate heparin activity 13 and its supplementation is indicated for heparin resistance. 14 Even when ACT is therapeutic, functional AT deficiency during CPB 15 may allow ongoing thrombin generation and platelet/fibrin activity, mechanisms implicated in HPE pathogenesis. The Hjärpe protocol suggests considering AT supplementation as part of the evaluation and correction of coagulation disturbances when HPE progresses despite therapeutic ACT. 4 However, AT is not without risk. Supraphysiologic antithrombin levels (200%–500% activity), not expected with the dose administered in this case, have been associated with an increased risk of bleeding 16 and acute kidney injury (AKI), 17 although a causal relationship with AKI has not been demonstrated.
Role of albumin
Albumin, when added to the priming solution, was historically considered protective against HPE 12 by improving oncotic balance, reducing erythrocyte aggregation and platelet count drop, 18 and through its hydrophilic and anti-inflammatory properties.19,20 Overall, the available evidence on albumin-coated oxygenators and extracorporeal circuits remains limited and heterogeneous.10,20 Other studies report small technical or laboratory benefits; however, these results are not consistent, and clinically important benefits have not been proved. 21 Moreover, there have been warnings of hyperoncotic albumin (20%), iso-oncotic albumin (4%–5%), especially the potential links with AKI, bleeding, red blood cell transfusion and infections22-25. Therefore, despite the fact that albumin is still a component in HPE haemodilution strategies, its usage needs to be balanced with its risks and expenses, 26 particularly in patients who already have renal impairment.
Conclusion
This case highlights that the timely observation of the pressure increase in the oxygenators during CPB, coupled with a prompt and concerted response, is critical to preventing the development of oxygenator failure. The use of AT in this patient, despite therapeutic ACT values, followed by a small bolus of 20% albumin, was temporarily correlated with a further decrease in transmembrane pressures and resistance, allowing for the continuation of CPB and a subsequent uneventful perioperative course. The synergistic anticoagulant, platelet-modulating and anti-inflammatory properties of AT and albumin may mitigate HPE within the oxygenator; however, these interactions remain poorly characterized. Further investigation is warranted to elucidate the underlying mechanisms and facilitate the development of standardized, evidence-based protocols for HPE management during CPB.
Supplemental Material
sj-docx-1-jao-10.1177_03913988261450135 – Supplemental material for Antithrombin and 20% albumin as treatment of oxygenator high pressures excursion during cardiopulmonary bypass in cardiac surgery: A case report
Supplemental material, sj-docx-1-jao-10.1177_03913988261450135 for Antithrombin and 20% albumin as treatment of oxygenator high pressures excursion during cardiopulmonary bypass in cardiac surgery: A case report by Raffaele Mandarano, Silvia Pedevilla, Flavia Annese, Luca Pessetti, Enrico Squiccimarro, Stefano Romagnoli and Sergio Bevilacqua in The International Journal of Artificial Organs
Footnotes
Acknowledgements
The authors thank the patient who participated in this study. The authors thank all the perfusionists working at the Careggi University Hospital in Florence, Italy.
Author contributions
RM, SP, FA, SB and SR: writing – original draft, writing – review and editing. RM: conceptualization, data curation, project administration, writing – review and editing. RM, ES, LP, SB and SR: formal analysis, software, supervision.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.