
Abstract
Objective:
To examine the associations between neonatal–maternal characteristics and mechanical ventilation duration in critically ill neonates, and to explore differences between respiratory distress syndrome (RDS) and non-RDS subgroups.
Methods:
This retrospective study included 319 neonates who required mechanical ventilation in the neonatal intensive care unit of our hospital between 1 January 2022 and 31 December 2024. Data on neonatal demographics, Apgar scores, initial arterial blood gas parameters and maternal characteristics, including age, delivery mode and comorbidities, were collected. The primary outcome was total ventilation duration. Correlation and subgroup analyses were performed.
Results:
The median duration of total mechanical ventilation (invasive + non-invasive) was 133.0 (interquartile range (IQR): 146.0) h. All neonates received invasive mechanical ventilation with a median duration of 48.0 (IQR: 58.0) h, and 83.7% subsequently required non-invasive ventilation support. Ventilation duration was negatively correlated with gestational age (r = −0.503, p < 0.001) and birth weight (r = −0.473, p < 0.001) and positively correlated with blood pH (r = 0.142, p = 0.011), using PS (r = 0.439, p < 0.001) and bicarbonate (r = 0.141, p = 0.012). No significant associations were found with Apgar scores, lactate or maternal age. Compared with non-RDS neonates, those with RDS had significantly longer ventilation durations (135.0 (IQR: 147.0) vs 73.5 (IQR: 100.8) h, p < 0.001), as well as lower gestational age and birth weight, altered blood gas parameters and a higher rate of caesarean deliveries (all p < 0.05). Maternal comorbidity rates did not differ significantly between the groups (p > 0.05). The results of multivariate regression analysis showed that the independent factors affecting mechanical ventilation time were gestational age, pulmonary surfactant, birth weight, blood pH, HCO3− and mode of delivery.
Conclusions:
Neonatal factors, especially gestational age and birth weight, critically impact ventilation duration in critically ill neonates. Tailored respiratory management addressing diagnosis and key perinatal factors (gestational age, birth weight) may improve outcomes.
Keywords
Introduction
Mechanical ventilation is an essential life-support modality in the neonatal intensive care unit (NICU), particularly for critically ill neonates with respiratory failure. 1 Although mechanical ventilation can be lifesaving, prolonged ventilatory support is associated with increased risks of adverse outcomes, including ventilator-associated pneumonia, bronchopulmonary dysplasia (BPD) and long-term neurodevelopmental impairments. Therefore, elucidating the factors that influence the duration of mechanical ventilation is critical for optimising clinical management, improving neonatal outcomes and ensuring efficient utilisation of healthcare resources. Despite advances in neonatal respiratory care, the global incidence of prolonged mechanical ventilation (⩾72 h) in critically ill neonates remains 30%–40%, with preterm infants (gestational age <34 weeks) accounting for over 70% of cases.1,2 Prolonged ventilation not only increases healthcare costs (by an estimated 15,000 dollar/neonate in high-income settings 2 ) but also doubles the risk of BPD – a leading cause of long-term respiratory morbidity in survivors. 3 These data underscore the urgency of identifying modifiable factors that influence ventilation duration.
Previous studies have identified key neonatal determinants of ventilation duration, including gestational age, birth weight and primary respiratory diagnoses such as respiratory distress syndrome (RDS). 4 However, most investigations have not comprehensively incorporated both neonatal clinical parameters and maternal risk factors that may affect neonatal respiratory function and ventilation needs. 5 Moreover, it remains unclear whether these associations differ according to specific respiratory pathologies, for example, between RDS and non-RDS conditions. While prior studies have linked gestational age and birth weight to longer ventilation, 6 most have focussed on either neonatal factors alone or specific subgroups (e.g. very-low-birth-weight infants (<1500 g)), with limited attention to how maternal comorbidities (e.g. gestational diabetes, hypertensive disorders) interact with neonatal characteristics to affect ventilatory needs.7,8 Additionally, few studies have directly compared predictors of ventilation duration between neonates with RDS and those without – a distinction critical for tailoring management as RDS often requires surfactant therapy, whereas non-RDS conditions (e.g. meconium aspiration syndrome) may demand targeted infection control. 9
In this context, the present study systematically assesses the relationships between a broad spectrum of neonatal characteristics, including blood gas indices and clinical scores, as well as maternal high-risk factors related to mechanical ventilation duration in critically ill neonates. Subgroup analyses stratified by RDS status were performed to explore potential variations in predictors according to respiratory aetiology. By identifying independent factors associated with prolonged ventilation, this study aspires to provide evidence supporting individualised risk stratification.
Methods and materials
Study design and population
This retrospective study was conducted in the NICU of Beijing Chaoyang District Maternal and Child Health Care Hospital. Eligible participants met the following inclusion criteria: (1) gestational age ⩾28 weeks; (2) admission to the NICU within 24 h after birth; (3) requirement for mechanical ventilation (invasive and/or non-invasive) during hospitalisation and (4) availability of complete clinical data, including demographic characteristics, initial arterial blood gas results and maternal medical history.
Exclusion criteria included (1) major congenital anomalies (e.g. congenital diaphragmatic hernia, severe congenital heart disease); (2) known or suspected chromosomal abnormalities (e.g. trisomy 21 or 18); (3) diagnosed genetic or metabolic syndromes significantly affecting respiratory function and (4) incomplete medical records or missing key variables affecting data validity. The screening process of research participants is shown in Figure 1.

Study subject screening process.
The study protocol was approved by the ethics committee of our hospital. Given the retrospective design and use of de-identified data, the requirement for informed consent was waived in accordance with the Declaration of Helsinki and applicable local ethical regulations.
Data collection
Throughout the study period, all procedures involving intubation, extubation and weaning from non-invasive ventilation were performed in accordance with standardised clinical protocols established in our NICU, which align with international guidelines for neonatal respiratory support. 10
Comprehensive clinical data were systematically extracted from electronic medical records using a predefined data collection form to minimise extraction bias. Neonatal variables included demographic information (sex, gestational age, birth weight), Apgar scores at 1, 5 and 10 min, time of symptom onset and primary diagnosis categorised as either RDS or non-RDS conditions. The non-RDS group included diagnoses such as pneumonia, meconium aspiration syndrome and pulmonary haemorrhage. Additional neonatal data encompassed the total duration of mechanical ventilation (including both invasive and non-invasive modes), comorbidities, length of NICU stay (in days) and hospitalisation costs (in RMB).
Initial arterial blood gas parameters prior to the initiation of mechanical ventilation were recorded, including blood pH, partial pressure of oxygen (PaO2), partial pressure of carbon dioxide (PaCO2), base excess (BE), bicarbonate (HCO3−) and lactate levels. These indicators were deemed essential for evaluating the neonates’ respiratory and metabolic status.
Maternal clinical data were also collected, including maternal age, mode of delivery (vaginal or caesarean) and documented maternal comorbidities. The following maternal comorbidities were defined based on clinical diagnostic criteria: gestational diabetes mellitus (GDM) per World Health Organisation 2013 guidelines 11 ; hypertensive disorders complicating pregnancy (HDCP), including gestational hypertension, preeclampsia and chronic hypertension with superimposed preeclampsia (per American College of Obstetricians and Gynaecologists 2020 criteria) 12 ; and thyroid dysfunction (subclinical/overt hypothyroidism, hyperthyroidism) confirmed by serum thyroid function tests.
Neonatal complications were diagnosed per neonatal clinical practice guidelines as follows: intracranial haemorrhage (via cranial ultrasound); pneumonia (confirmed by chest X-ray findings consistent with infection (e.g. infiltrates, consolidation) plus supportive laboratory evidence (e.g. leukocytosis, elevated C-reactive protein (CRP))); coagulation disorders (abnormal prothrombin time/activated partial thromboplastin time) and sepsis (positive blood culture + clinical signs of infection), with severity graded per the Neonatal Sepsis Assessment Tool.
Outcomes
The primary outcome of interest was the total duration of mechanical ventilation, defined as the sum of hours on invasive mechanical ventilation (via endotracheal intubation) and subsequent non-invasive ventilation support (e.g. nasal continuous positive airway pressure (CPAP), nasal intermittent positive pressure ventilation). For neonates who required multiple episodes of ventilation (e.g. weaned off and then placed back on support), the durations of all episodes were summed to calculate the total duration. This measure served as a surrogate marker for severity of respiratory illness and resource utilisation.
Secondary outcomes were focussed on identifying clinical and maternal factors associated with prolonged total mechanical ventilation duration. These included neonatal demographic and clinical parameters (e.g. gestational age, birth weight, Apgar scores), initial arterial blood gas indicators (e.g. blood pH, HCO3−) and maternal risk factors (e.g. age, delivery mode, comorbidities). Moreover, subgroup analyses were performed comparing neonates with RDS and those with non-RDS respiratory conditions to explore potential aetiological differences in total mechanical ventilation requirements, as well as differences in the duration of invasive mechanical ventilation alone between the two subgroups.
Statistical analysis
Data were analysed using SPSS version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were tested for normality and are presented as means with standard deviations (SD) or medians with interquartile ranges (IQR), as appropriate. Categorical variables are reported as frequencies and percentages. Univariate analyses were conducted using independent t-tests or Mann–Whitney U tests for continuous variables, as appropriate, with chi-square tests used for categorical variables. Associations between ventilation duration and continuous variables were assessed using Spearman/Pearson correlation coefficients. Multiple linear regression analysis was conducted with mechanical ventilation time as the dependent variable, and categorical variables and indicators with statistical differences in correlation analysis as independent variables. All statistical tests were two-sided, and a p < 0.05 was considered statistically significant.
Results
Neonatal characteristics and maternal risk factors
A total of 319 neonates were enrolled, including 183 boys (57.4%) and 136 girls (42.6%). The median gestational age was 35.3 (IQR: 5.0) weeks, and the median birth weight was 2.39 (IQR: 1.41) kg. The median Apgar scores at 1, 5 and 10 min were 9.0 (IQR: 2.0), 10.0 (IQR: 0.0) and 10.0 (IQR: 0.0), respectively. The median time of symptom onset was 15.0 (IQR: 20.0) min. The median duration of NICU stay was 14.0 (IQR: 16.0) days, and the median hospitalisation cost was 41,772.2 (IQR: 34,764.8) RMB. One neonatal death was recorded during hospitalisation. Table 1 presents details on neonatal demographics, maternal comorbidities and NICU stay.
Baseline characteristics of the study cohort and comparison between RDS and non-RDS neonates.
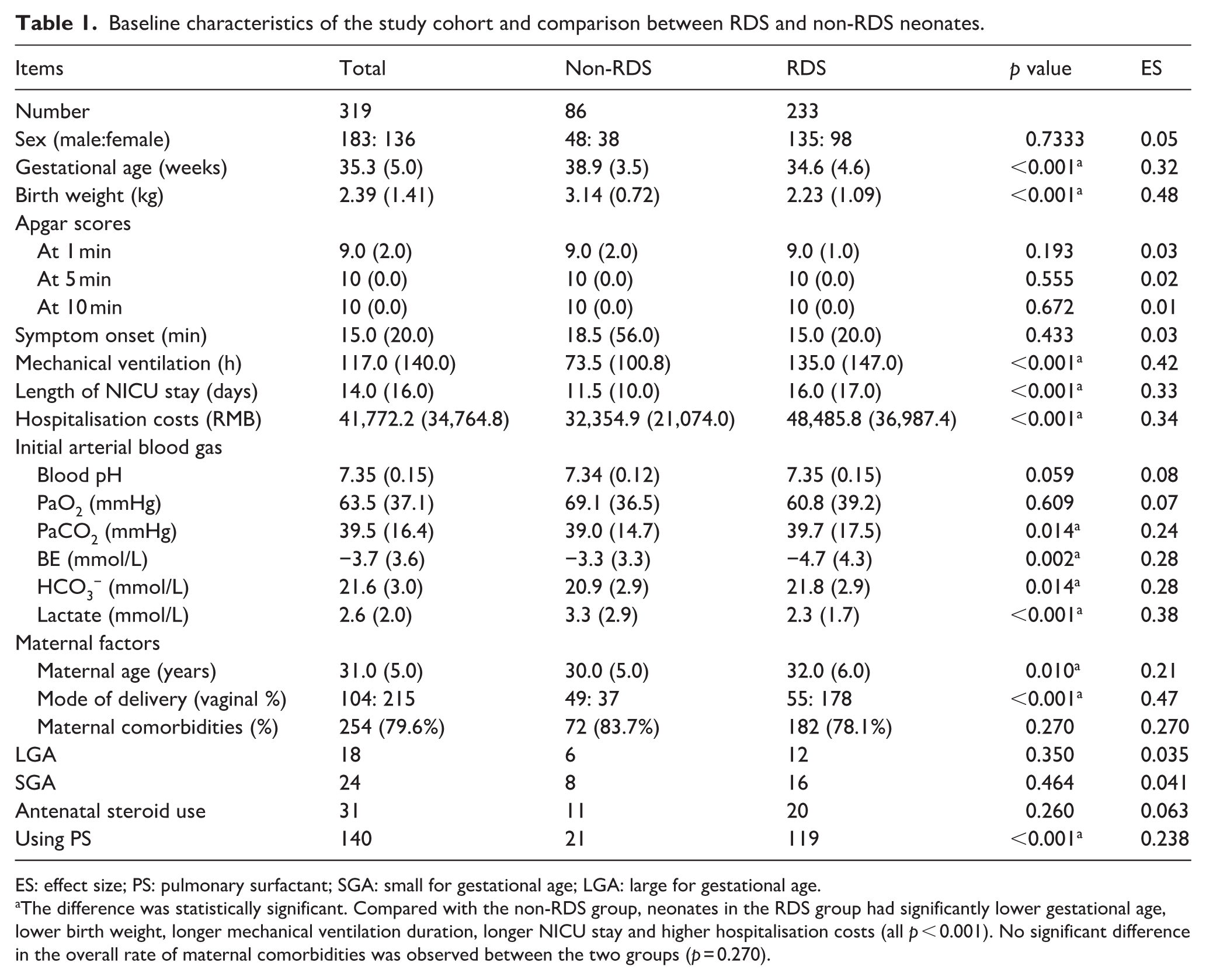
ES: effect size; PS: pulmonary surfactant; SGA: small for gestational age; LGA: large for gestational age.
The difference was statistically significant. Compared with the non-RDS group, neonates in the RDS group had significantly lower gestational age, lower birth weight, longer mechanical ventilation duration, longer NICU stay and higher hospitalisation costs (all p < 0.001). No significant difference in the overall rate of maternal comorbidities was observed between the two groups (p = 0.270).
Among all neonates, 233 (73.0%) were primarily diagnosed with RDS, whereas 86 (27.0%) had non-RDS conditions. Diagnoses in the non-RDS group included pneumonia (54 cases, 62.8%), meconium aspiration syndrome (16 cases, 18.6%), pulmonary haemorrhage (six cases, 7.0%), birth asphyxia (four cases, 4.7%), sepsis (two cases, 2.3%), prematurity (two cases, 2.3%), transient tachypnoea of the newborn (one case, 1.2%) and purulent meningitis (one case, 1.2%).
The median maternal age was 31.0 (5.0) years. Vaginal delivery was recorded in 104 cases (32.6%), and caesarean section in 215 cases (67.4%). The most common maternal comorbidity was GDM (89 cases, 27.9%), followed by HDCP (70 cases, 21.9%) and thyroid dysfunction (40 cases, 12.5%). Other maternal conditions included uterine scarring (31 cases, 9.7%), genital tract infections such as group B streptococcus and trichomonas (20 cases, 6.3%), premature rupture of membranes (17 cases, 5.3%), placental abnormalities (17 cases, 5.3%), threatened preterm labour (14 cases, 4.4%), uterine malformations (14 cases, 4.4%), immunologic or thrombotic disorders (15 cases, 4.7%), twin pregnancy (11 cases, 3.4%), anaemia (13 cases, 4.1%), abnormal foetal presentation (six cases, 1.9%), hepatobiliary disorders (seven cases, 2.2%), urinary tract diseases (six cases, 1.9%) and adverse pregnancy history (six cases, 1.9%).
Mechanical ventilation duration and related factors
The median total duration of mechanical ventilation was 133.0 (IQR: 146.0) h. Among the neonates, 267 (83.7%) received subsequent non-invasive ventilation, with a median duration of 69.0 (IQR: 106.0) h. A total of 28 (8.8%) neonates required repeated endotracheal intubation.
Spearman correlation analysis showed that mechanical ventilation duration was negatively correlated with gestational age (r = −0.503, p < 0.001) and birth weight (r = −0.473, p < 0.001). No significant correlations were observed with Apgar scores at 1 min (r = −0.071, p = 0.206), 5 min (r = −0.0377, p = 0.503) or 10 min (r = −0.079, p = 0.158), or with symptom onset time (r = 0.001, p = 0.992). For initial blood gas parameters, blood pH (r = 0.142, p = 0.011), using PS (r = 0.439, p < 0.001) and HCO3− (r = 0.141, p = 0.012) were positively correlated with ventilation duration; PaCO2 (r = −0.095, p = 0.091), PaO2 (r = −0.033, p = 0.553), BE (r = 0.077, p = 0.169) and lactate level (r = −0.021, p = 0.713) were not significantly correlated. Maternal age (r = 0.052, p = 0.358) was also not significantly associated with ventilation time. For detailed correlation coefficients of all neonatal blood gas parameters and maternal factors (see Table 2 and Figure 2).
Correlations between mechanical ventilation duration and neonatal/maternal factors.
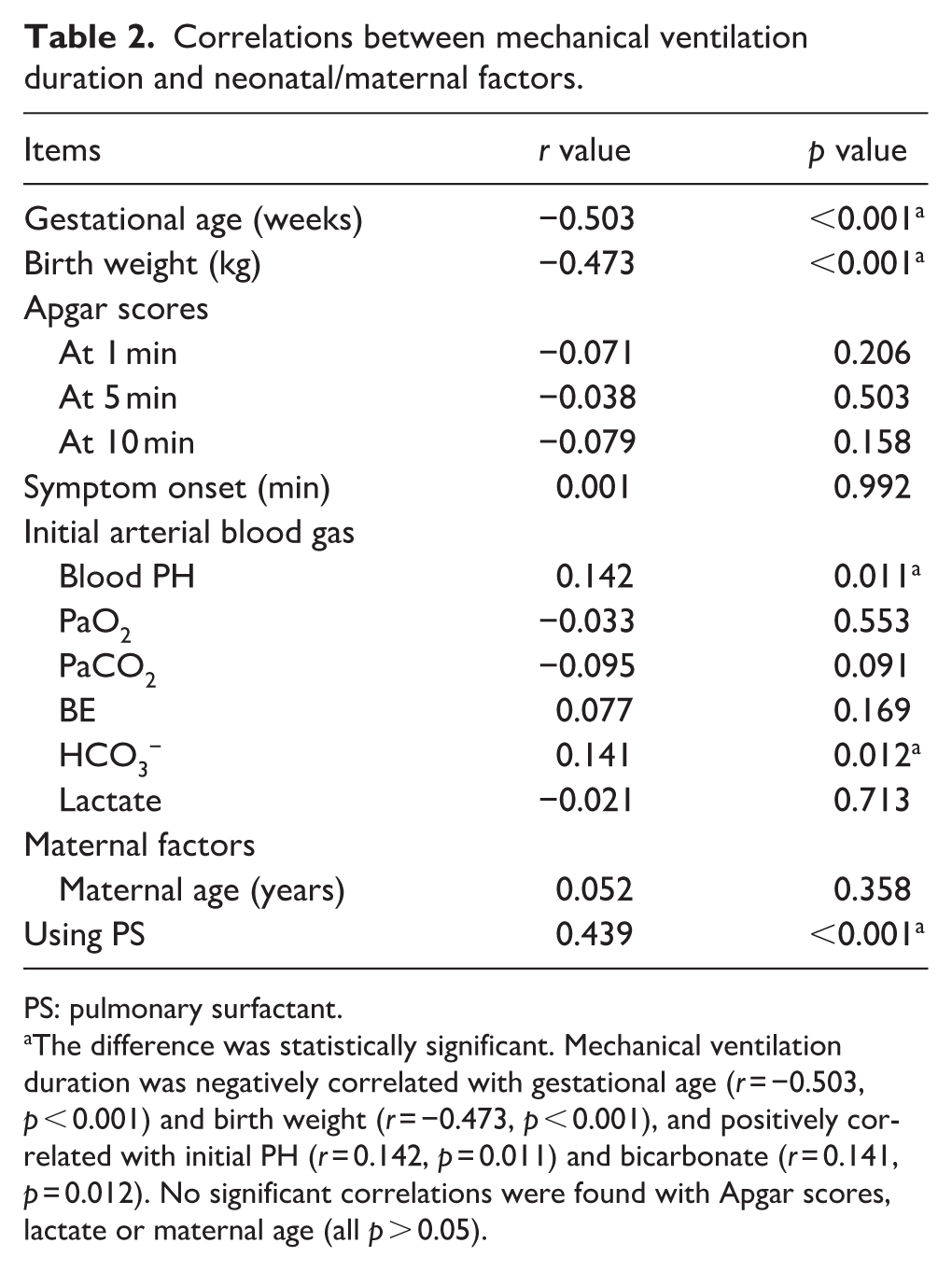
PS: pulmonary surfactant.
The difference was statistically significant. Mechanical ventilation duration was negatively correlated with gestational age (r = −0.503, p < 0.001) and birth weight (r = −0.473, p < 0.001), and positively correlated with initial PH (r = 0.142, p = 0.011) and bicarbonate (r = 0.141, p = 0.012). No significant correlations were found with Apgar scores, lactate or maternal age (all p > 0.05).
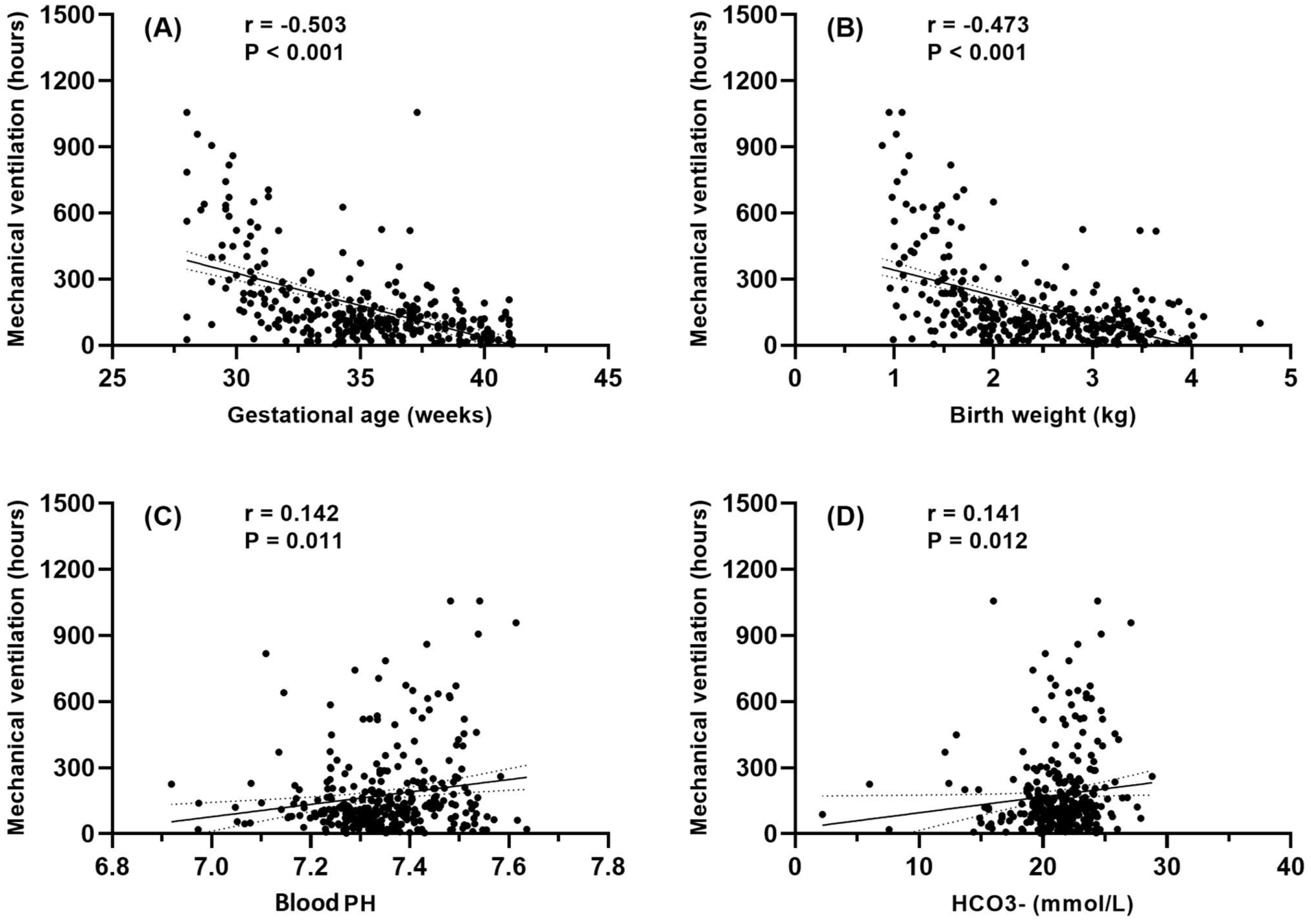
Correlation analyses between mechanical ventilation duration and key perinatal factors: panel (a) shows a strong negative correlation with gestational age (r = −0.503), reflecting the impact of prematurity on prolonged ventilation needs, panel (b) demonstrates a similar negative trend with birth weight (r = −0.473), consistent with the role of foetal growth in respiratory maturity and panels (c, d) reveal modest positive associations with blood pH (r = 0.142) and bicarbonate (r = 0.141), potentially indicating compensatory metabolic alkalosis in chronic respiratory acidosis.
The median ventilation duration was 117.0 (IQR: 131.0) h for male neonates and 118.5 (IQR 154.0) h for female neonates, with no significant difference between the two groups (p = 0.520). Among neonates delivered vaginally, the median ventilation duration was 110.5 (IQR: 171.3) h, compared with 118.5 (IQR: 133.0) h for those delivered by caesarean section (p = 0.790). For neonates without maternal comorbidities, the median ventilation duration was 130.0 (IQR: 100.0) h, compared with 113.8 (IQR: 150.3) h in those with maternal comorbidities (p = 0.512).
Comparison of maternal–neonatal factors between the two groups
Compared with the non-RDS group, neonates in the RDS group had significantly longer mechanical ventilation duration (135.0 (IQR: 147.0) vs 73.5 (IQR: 100.8) h, p < 0.001). Compared with neonates in the non-RDS group, those with RDS had significantly lower gestational age (34.6 (IQR: 4.6) vs 38.9 (IQR: 3.5) weeks, p < 0.001) and lower birth weight (2.23 (IQR: 1.09) vs 3.14 (IQR: 0.72) kg, p < 0.001). The RDS group also exhibited longer NICU stay (16.0 (IQR: 17.0) vs 11.5 (IQR: 10.0) days, p < 0.001) and higher hospitalisation costs (48,485.8 (IQR: 36,987.4) vs 32,354.9 (IQR: 21,074.0) RMB, p < 0.001). There was no significant difference in Apgar scores at 1 min between the RDS group and the non-RDS group; both groups had a median Apgar score of 9.0 (IQR: 2.0) at 1 min (p = 0.193).The time of symptom onset was comparable between groups (15.0 (IQR: 20.0) vs 18.5 (IQR: 56.0) min, p = 0.433).
Regarding initial arterial blood gas parameters, the RDS group showed higher PaCO2 levels (39.7 (IQR: 17.5) vs 39.0 (IQR: 14.7) mmHg, p = 0.014), lower BE (−4.7 (IQR: 4.3) vs −3.3 (IQR: 3.3) mmol/L, p = 0.002), lower HCO3− concentration (21.8 (IQR: 2.9) vs 20.9 (IQR: 2.9) mmol/L, p = 0.014) and lower lactate levels (2.3 (IQR: 1.7) vs 3.3 (IQR: 2.9) mmol/L, p < 0.001). The difference in blood pH between groups was not statistically significant (7.35 (IQR: 0.15) vs 7.34 (IQR: 0.12), p = 0.059), as was the case with the PaO2 level (60.8 (IQR: 39.2) vs 69.1 (IQR: 36.5) mmHg, p = 0.609).
Maternal age was higher in the RDS group (32.0 (IQR: 6.0) vs 30.0 (IQR: 5.0) years, p = 0.010), and caesarean deliveries were more frequent (178 vs 37 cases, p < 0.001). There was no significant difference in the overall rate of maternal comorbidities between the two groups (78.1% vs 83.7%, p = 0.270). For detailed comparisons of neonatal blood gas parameters and complications between the two groups (refer to Table 1). The results of multivariate regression analysis showed that the independent factors affecting mechanical ventilation time were gestational age, pulmonary surfactant, birth weight, blood pH, HCO3− and mode of delivery (see Table 3 for details).
Multiple linear regression results of mechanical ventilation time.
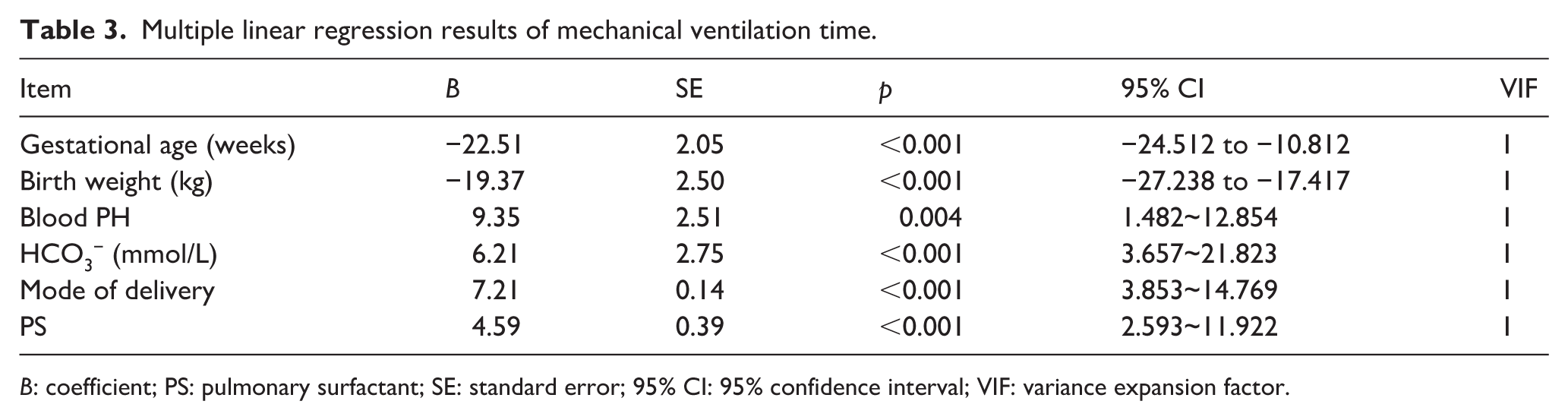
B: coefficient; PS: pulmonary surfactant; SE: standard error; 95% CI: 95% confidence interval; VIF: variance expansion factor.
Discussion
Consistent with contemporary literature emphasising that non-invasive ventilation (e.g. nasal CPAP) is less harmful and may improve long-term pulmonary outcomes in preterm infants (⩾32–34 weeks postmenstrual age), 13 we redefined our primary outcome as invasive mechanical ventilation duration (rather than total ventilation) to avoid equating non-invasive and invasive support. This distinction enhances clinical relevance, as invasive ventilation is the main driver of adverse outcomes (e.g. BPD) and a priority for optimisation. Our focus on invasive duration also addresses a key gap in prior studies that often grouped ventilation modes, providing more actionable insights for reducing invasive support exposure in critically ill neonates.
Mechanical ventilation is a critical intervention for managing critically ill neonates in the NICU. While it is lifesaving, prolonged mechanical ventilation is associated with increased risk of complications, such as BPD, hospital-acquired infections and adverse neurodevelopmental outcomes. Primarily caused by surfactant deficiency in preterm infants, RDS is a common and severe respiratory condition that often necessitates extended ventilatory support.4,5,14 In this retrospective study of 319 mechanically ventilated neonates, we examined both neonatal and maternal factors influencing ventilation duration and compared clinical differences between neonates with RDS and those with other respiratory conditions, providing important insights for tailored respiratory care.
This study identified lower gestational age and birth weight as the most significant predictors of prolonged mechanical ventilation in neonates, consistent with previous reports that demonstrated an increased risk of severe RDS in preterm neonates and highlighted low birth weight as a key risk factor for RDS.6,7,15,16 Our finding that gestational age (r = −0.503) and birth weight (r = −0.473) are the strongest correlates of ventilation duration aligns with a large multicentre study by Sauthier et al., 2 which reported similar negative associations (r = −0.48 for gestational age, r = −0.45 for birth weight) in 1200 ventilated neonates. However, our subanalysis extends this work by showing that neonates with RDS require around 83% longer ventilation (median: 135.0 h) than those without RDS (median: 73.5 h) – a larger gap than previously reported (50%–60% in Shin et al. 6 ). This difference may reflect our cohort’s higher proportion of preterm RDS neonates (68% of RDS cases had gestational age <34 weeks), highlighting the need for antenatal corticosteroids to reduce RDS severity and shorten ventilation.5,9 These associations reflect the physiological immaturity of the preterm lung, where inadequate surfactant production, underdeveloped alveolar structures and insufficient respiratory muscle strength contribute to impaired gas exchange and increased work of breathing, resulting in prolonged ventilatory support. It should be noted that surfactant replacement therapy, a cornerstone in the management of RDS, was not explicitly recorded in our dataset regarding its timing, dosage or frequency of administration. Although we observed a higher rate of caesarean sections in the RDS group, this association is likely confounded by the underlying indications for this procedure, such as maternal hypertensive disorders, foetal distress or preterm labour. Since RDS is intrinsically a disorder of prematurity, the primary driver of prolonged ventilation is likely the immature lung structure and surfactant deficiency characteristic of preterm birth, rather than the mode of delivery itself.17,18 Subgroup analysis further showed that neonates with RDS had significantly lower gestational ages, lower birth weights and higher arterial carbon dioxide levels compared with those with non-RDS conditions, reinforcing the pathophysiological basis of RDS as a disease of prematurity.4,19 These findings emphasise the clinical value of antenatal corticosteroids and timely postnatal surfactant therapy in improving pulmonary outcomes for preterm infants.
A noteworthy finding was the modest positive correlation between initial blood gas parameters (blood pH and HCO3−) and ventilation duration. While elevated blood pH and HCO3− might typically indicate clinical stability, in this context, they likely reflect compensatory metabolic alkalosis secondary to chronic respiratory acidosis in neonates with prolonged subacute respiratory compromise. Elevated HCO3− suggests renal compensation for sustained CO2 retention, whereas a preserved blood pH may represent a homeostatic adjustment rather than adequate ventilation. This aligns with studies demonstrating that neonates with chronic respiratory conditions often develop metabolic compensation to mitigate acidosis, potentially prolonging ventilatory needs. 20 Survivor bias may also contribute, as neonates with severe acidosis might have shorter ventilation times due to rapid deterioration or mortality. These findings underscore the complexity of interpreting isolated blood gas values and highlight the need for dynamic, longitudinal assessments in ventilated neonates. 21
Regarding maternal factors, we did not observe significant independent associations between maternal age, gestational diabetes, hypertensive disorders of pregnancy or mode of delivery and the duration of mechanical ventilation.17,18,22,23 However, the absence of statistical significance does not imply a lack of clinical relevance. Maternal comorbidities may influence neonatal respiratory outcomes through indirect pathways, such as contributing to prematurity, foetal growth restriction or placental insufficiency. Moreover, the high baseline prevalence of maternal complications in both groups within our cohort may have attenuated any measurable differences. It is also important to note that key antenatal interventions, such as the use of corticosteroids or magnesium sulphate, were not captured in our dataset and may have moderated the observed relationships.
This retrospective single-centre study was conducted using de-identified data from our NICU, where standardised data collection and consistent neonatal respiratory management protocols ensured high-quality data for analysing factors associated with mechanical ventilation duration. However, several limitations of this study should be acknowledged. First, as a retrospective study, the analysis is inherently subject to potential selection bias and unmeasured confounding factors. Furthermore, the single-centre design restricts broad generalisability. Second, despite adjusting for key neonatal and maternal factors, our analysis did not account for several clinically relevant confounders, including surfactant administration timing/dosage, inspired oxygen fraction, infection markers (e.g. CRP, procalcitonin), ventilator modes (e.g. SIMV vs HFOV), ventilation mode, maternal infections and sedation protocols. A key limitation is the absence of data on critical antenatal interventions, such as corticosteroid administration for foetal lung maturation or magnesium sulphate for neuroprotection. Future prospective studies should systematically collect antenatal treatment data to clarify their modifying effects. Additionally, ventilation duration may be influenced by institutional protocols, limiting generalisability. Finally, due to limitations such as research funding, this study did not conduct a survival analysis or perform a stratified analysis of non-invasive ventilation duration. Further research could explore these aspects.
Conclusion
In conclusion, neonatal characteristics, particularly gestational age, birth weight and respiratory diagnosis, remain the most important determinants of mechanical ventilation duration in critically ill neonates. Maternal factors may exert a more indirect influence, primarily through their effects on foetal development and birth outcomes rather than directly impacting postnatal respiratory needs. Future research should focus on validating these findings in larger multicentre cohorts and on developing predictive models that incorporate both maternal and neonatal variables to guide early and individualised respiratory management strategies.
Footnotes
Acknowledgements
The authors would like to thank the medical and nursing staff of the NICU for their support in data collection and clinical care related to this study.
Author contributions
Conception and design of the research: Yueqiao Gao, Jiuye Guo and Zulin Lu. Acquisition of data: Lifang Zhao. Analysis and interpretation of the data: Ying Liu. Statistical analysis: Wei Fu. Obtaining financing: none. Writing of the manuscript: Zulin Lu and Lifang Zhao. Critical revision of the manuscript for intellectual content: Yueqiao Gao and Jiuye Guo. All authors reviewed and approved of the final manuscript.
Data availability statement
The original clinical data used in this study are available from the corresponding author upon reasonable request. Requests should include a detailed research proposal and proof of ethical approval from the requester’s affiliated institution to ensure compliance with patient privacy protection regulations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This study was conducted in accordance with the Declaration of Helsinki and approved by the Research Ethics Committee of Beijing Chaoyang District Maternal and Child Health Care Hospital (approval number: CYFY-EC2022-001). Given the retrospective design and use of de-identified data, the requirement for informed consent was waived in accordance with the Declaration of Helsinki and applicable local ethical regulations.
Consent for publication
Not applicable.