
Abstract
Introduction:
Artificial pancreas systems represent an important technological advancement in the management of type 1 diabetes mellitus (T1DM). These systems provide automated insulin delivery and have the potential to improve glycemic control and cardiometabolic outcomes. In this study, we aimed to evaluate the effects of artificial pancreas systems on glycemic control, lipid parameters, and proteinuria in patients with T1DM in a real-world clinical setting.
Methods:
This retrospective study included 32 patients with T1DM who transitioned to artificial pancreas therapy. Glycemic parameters including HbA1c, fasting blood glucose (FBG), and postprandial blood glucose (PBG) were compared before pump initiation and at 3 months, 6 months, and 1 year after treatment. Lipid parameters and spot urine proteinuria levels were evaluated before pump therapy and at 1-year follow-up. Repeated measures ANOVA and paired t-tests were used for continuous variables, while Cochran’s Q and McNemar tests were used for categorical variables.
Results:
A significant reduction in HbA1c levels was observed over time, decreasing from 8.74 ± 1.21% before pump initiation to 7.92 ± 0.98% at 3 months, 7.61 ± 0.87% at 6 months, and 7.48 ± 0.83% at 1 year (p < 0.001). Fasting and postprandial glucose levels also significantly declined during follow-up (p < 0.001). LDL cholesterol and total cholesterol levels decreased significantly at 1 year (p = 0.029 and p = 0.006, respectively), while HDL cholesterol increased significantly (p = 0.022). The reduction in triglyceride levels was not statistically significant (p = 0.069). Proteinuria levels decreased from 84.6 ± 42.3 mg/g before pump therapy to 61.8 ± 35.7 mg/g at 1 year (p = 0.011). The proportion of patients achieving HbA1c target increased from 18.8% before pump therapy to 62.5% at 1 year (p < 0.001).
Conclusion:
Artificial pancreas therapy significantly improves glycemic control and increases the proportion of patients achieving HbA1c targets in individuals with T1DM. In addition, favorable effects on lipid profile and proteinuria suggest potential cardiometabolic benefits of artificial pancreas systems.
Keywords
Introduction
Type 1 diabetes mellitus (T1DM) is a chronic autoimmune disease characterized by insulin deficiency and persistent hyperglycemia. Despite advances in insulin therapy, maintaining optimal glycemic control remains challenging for many patients. Poor glycemic control is associated with the development of microvascular and macrovascular complications, including nephropathy, retinopathy, and cardiovascular disease.
Artificial pancreas systems, also known as closed-loop insulin delivery systems, combine continuous glucose monitoring with automated insulin delivery algorithms1,2,3. These systems represent a major technological advancement in diabetes management and are designed to improve glycemic control while reducing the burden of self-management4,5,6.
Recent studies have demonstrated that artificial pancreas systems improve time in range and reduce HbA1c levels in patients with T1DM7,8. However, real-world data evaluating their effects on broader cardiometabolic parameters remain limited. In particular, their potential effects on lipid profiles and renal markers such as proteinuria have not been extensively investigated.
Therefore, the aim of this study was to evaluate the real-world clinical and metabolic outcomes of artificial pancreas systems in patients with T1DM, focusing on glycemic control, cardiometabolic parameters, and proteinuria.
Materials and methods
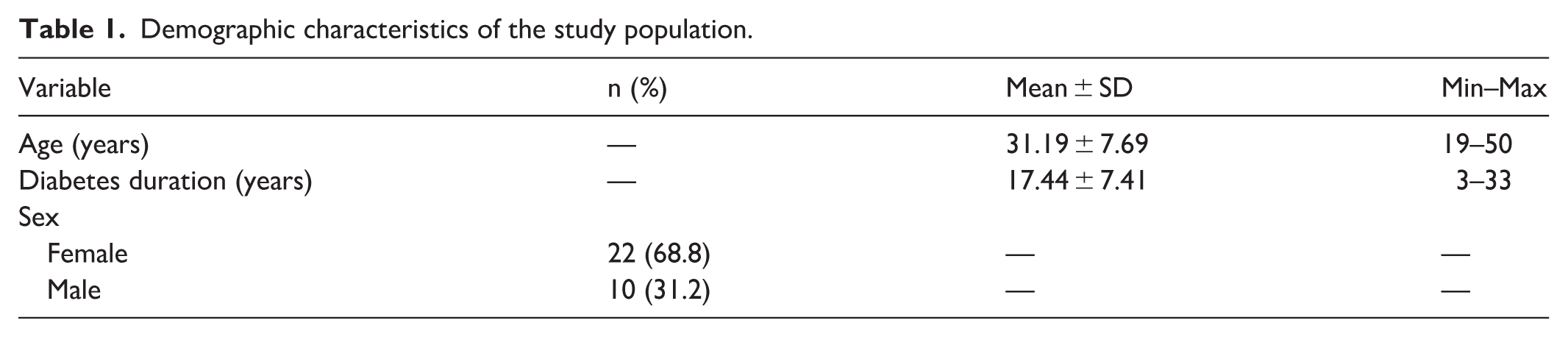
This retrospective study included patients with T1DM who initiated artificial pancreas therapy at our center. A total of 32 patients were included in the analysis. The mean age of the patients was 31.19 ± 7.69 years (range 19–50), and the mean duration of diabetes was 17.44 ± 7.41 years. Of the participants, 22 (68.8%) were female and 10 (31.2%) were male. Clinical and laboratory data were retrospectively obtained from patient records (Table 1).
Demographic characteristics of the study population.
Glycemic parameters including HbA1c, fasting blood glucose (FBG), and postprandial blood glucose (PBG) were recorded before pump initiation and at 3 months, 6 months, and 1 year after therapy. Lipid parameters (LDL cholesterol, HDL cholesterol, triglycerides, and total cholesterol) and spot urine proteinuria levels were evaluated before pump therapy and at the 1-year follow-up. The proportion of patients achieving HbA1c target levels was also evaluated during follow-up.
Statistical analyses were performed using IBM SPSS software. Continuous variables were expressed as mean ± standard deviation, while categorical variables were presented as numbers and percentages. Repeated measures ANOVA and paired t-tests were used for comparisons of continuous variables across time points. Cochran’s Q and McNemar tests were used to evaluate changes in categorical variables. A p-value <0.05 was considered statistically significant.
Results
A significant reduction in HbA1c levels was observed during follow-up. The mean HbA1c decreased from 8.74 ± 1.21% before pump initiation to 7.92 ± 0.98% at 3 months, 7.61 ± 0.87% at 6 months, and 7.48 ± 0.83% at 1 year (p < 0.001). Similarly, fasting blood glucose levels decreased from 186.3 ± 52.4 mg/dL before pump therapy to 149.9 ± 35.6 mg/dL at 1 year (p < 0.001). Postprandial glucose levels also significantly decreased from 228.7 ± 61.5 mg/dL to 181.5 ± 41.2 mg/dL during follow-up (p < 0.001) (Table 2).
Comparison of metabolic parameters before and after artificial pancreas therapy.

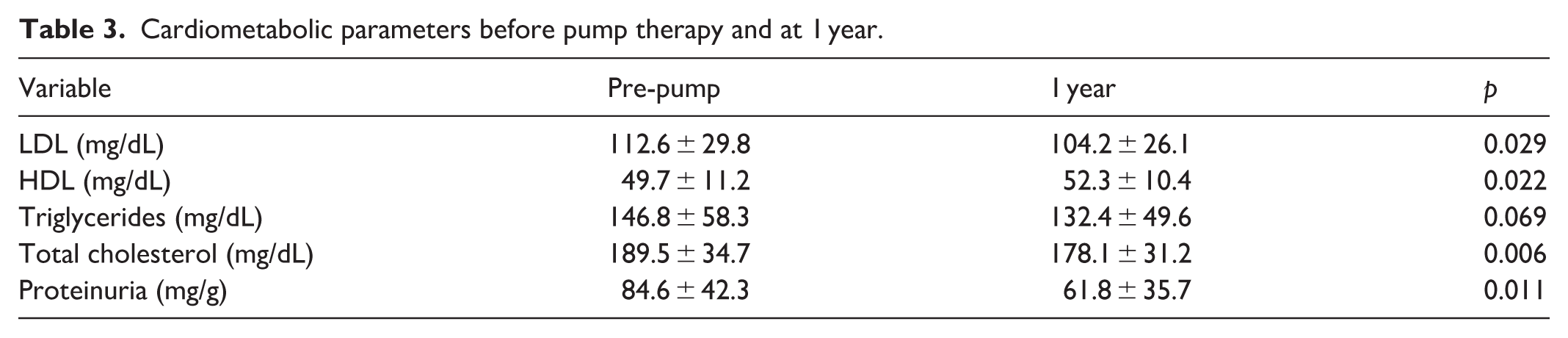
Lipid profile analysis showed a significant decrease in LDL cholesterol from 112.6 ± 29.8 mg/dL to 104.2 ± 26.1 mg/dL at 1 year (p = 0.029). Total cholesterol levels also decreased significantly (p = 0.006). HDL cholesterol levels increased significantly from 49.7 ± 11.2 mg/dL to 52.3 ± 10.4 mg/dL (p = 0.022). Although triglyceride levels decreased from 146.8 ± 58.3 mg/dL to 132.4 ± 49.6 mg/dL, this change was not statistically significant (p = 0.069). Proteinuria levels decreased significantly from 84.6 ± 42.3 mg/g before pump therapy to 61.8 ± 35.7 mg/g at 1 year (p = 0.011) (Table 3).
Cardiometabolic parameters before pump therapy and at 1 year.
The proportion of patients achieving HbA1c targets increased substantially over time (Table 4). While only 6 patients (18.8%) were within target before pump therapy, this proportion increased to 14 patients (43.8%) at 3 months, 18 patients (56.3%) at 6 months, and 20 patients (62.5%) at 1 year. The increase in target achievement was statistically significant (p < 0.001), with post-hoc analysis indicating that the difference between baseline and 1-year follow-up was particularly significant (Figure 1).
Comparison of HbA1c target achievement before and after artificial pancreas therapy.

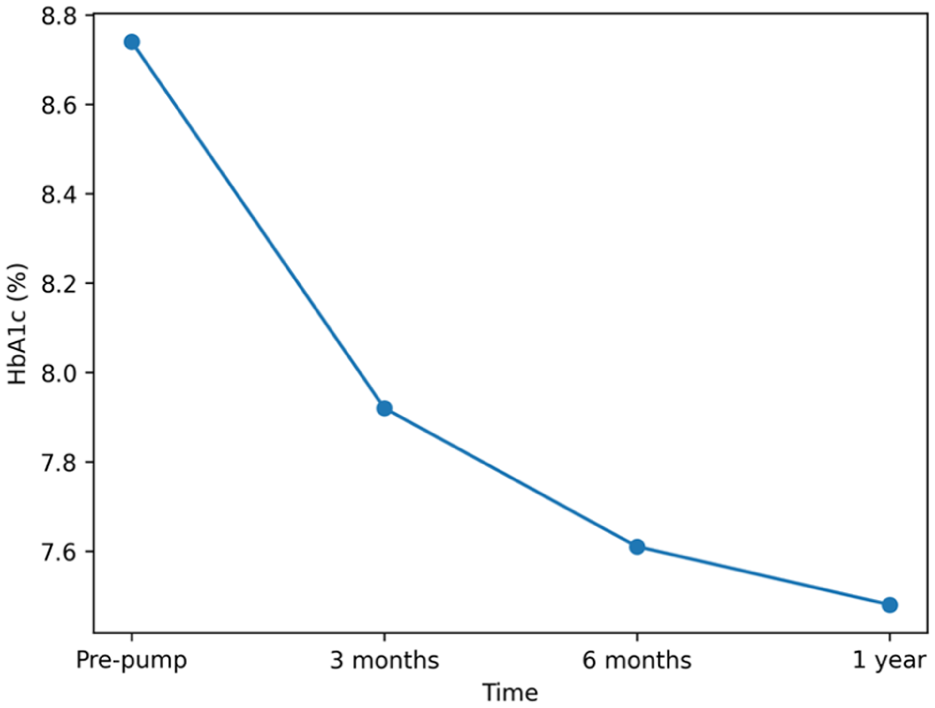
Change in HbA1c levels after initiation of artificial pancreas therapy.
Discussion
Our study demonstrates that artificial pancreas systems significantly improve glycemic control in patients with type 1 diabetes in a real-world clinical setting. The progressive reduction in HbA1c observed during follow-up is consistent with findings from randomized trials evaluating closed-loop insulin delivery systems 9 .
Previous large clinical trials have shown that artificial pancreas systems significantly reduce HbA1c and increase time spent within the target glucose range compared with conventional insulin therapy. For example, Brown et al. demonstrated significant improvements in glycemic control with closed-loop systems during a 6-month randomized trial. Similarly, Bergenstal et al. reported improved glycemic outcomes with hybrid closed-loop therapy in patients with type 1 diabetes1,2.
Beyond improvements in glycemic control, our study also demonstrated favorable changes in cardiometabolic parameters. The observed reduction in LDL cholesterol and total cholesterol levels, along with the increase in HDL cholesterol, may reflect the metabolic benefits associated with improved glycemic regulation. Previous studies have shown that improved glucose control is associated with reductions in cardiovascular risk factors in patients with diabetes10,11.
Another important finding of our study was the significant reduction in proteinuria levels during follow-up. Diabetic nephropathy remains one of the most important microvascular complications of type 1 diabetes, and persistent hyperglycemia plays a central role in its pathogenesis. Improved glycemic control achieved with artificial pancreas systems may contribute to renal protection by reducing glomerular hyperfiltration and metabolic stress7,10,12.
Additionally, the proportion of patients achieving HbA1c targets increased substantially during follow-up, highlighting the clinical effectiveness of artificial pancreas therapy in routine clinical practice13,14.
Strengths of the study
Several strengths should be noted in our study. First, this study provides real-world clinical data on artificial pancreas therapy in patients with type 1 diabetes, reflecting outcomes observed in routine clinical practice rather than controlled trial environments. Second, the study evaluated multiple cardiometabolic parameters, including lipid profile and proteinuria, in addition to glycemic control. These outcomes are less frequently reported in artificial pancreas studies and provide a broader understanding of the metabolic impact of automated insulin delivery systems. Third, the study included longitudinal follow-up up to 1 year, allowing the evaluation of sustained metabolic effects after initiation of artificial pancreas therapy.
Limitations of the study
This study has several limitations that should be considered when interpreting the results. First, the study was conducted in a single center with a relatively small sample size, which may limit the generalizability of the findings. Second, the retrospective design may introduce potential selection bias and limits the ability to establish causal relationships. Third, the study lacked a control group using conventional insulin therapy, which would have allowed a more direct comparison of treatment effects. Finally, although improvements in proteinuria and lipid parameters were observed, the follow-up duration was limited to 1 year, and longer-term studies are needed to evaluate the sustained renal and cardiovascular effects of artificial pancreas therapy.
Clinical implications
Artificial pancreas systems may provide benefits beyond glycemic control, potentially improving cardiometabolic risk factors and early markers of diabetic nephropathy. These findings support the broader clinical use of automated insulin delivery systems in the management of patients with type 1 diabetes.
Conclusion
Artificial pancreas systems significantly improve glycemic control in patients with type 1 diabetes and markedly increase the proportion of patients achieving HbA1c targets. Beyond improvements in glycemic parameters, the favorable changes observed in lipid profile and the significant reduction in proteinuria suggest that artificial pancreas therapy may confer beneficial cardiometabolic and renal effects. Considering that proteinuria typically increases with longer diabetes duration due to the progression of diabetic nephropathy, the reduction observed in our cohort highlights the potential role of improved glycemic regulation in modifying early markers of diabetic complications. These findings emphasize that artificial pancreas systems may provide benefits extending beyond glucose control and support their growing role in routine clinical practice for improving metabolic outcomes in patients with type 1 diabetes. Larger prospective studies with longer follow-up are warranted to confirm the long-term cardiometabolic and renal benefits of artificial pancreas therapy.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.