
Abstract
Hemolysis represents a severe, potentially life-threatening complication of extracorporeal circulation and percutaneous transvalvular microaxial flow pumps. Endogenous carbon monoxide (CO) production, measured via point-of-care (POC) CO-metry, has been investigated as a potential early marker of hemolysis in patients supported by extracorporeal membrane oxygenation (ECMO). We report two cases of hemolysis during percutaneous transvalvular microaxial flow pump therapy associated with significantly elevated carboxyhemoglobin (CO-Hb) levels. Consequently, we hypothesize that CO-Hb serves as a readily available bedside parameter for the early detection of hemolysis in this patient population.
Introduction
Endogenous CO is produced by the enzyme heme oxygenase as a stress response. 1 The affinity of hemoglobin for CO is 210 times higher than for oxygen (O2), leading to a rapid increase in CO-Hb levels even in the presence of slightly elevated environmental CO levels. 2 Typically, endogenous CO production results in CO-Hb levels of less than 1%. 3 In patients diagnosed with hemolytic anemia, an increase in CO-Hb levels is frequently observed. A threshold of 2% has shown a sensitivity of 85% for the presence of hemolytic anemia. 4 In addition to various diseases associated with hemolysis, different types of artificial organ support can contribute to elevated hemolytic activity. Several studies have suggested the potential use of CO-Hb to detect hemolysis in ECMO patients.5–7 Whether CO-Hb can be utilized in mechanical support devices other than ECMO remains uncertain. Percutaneous transvalvular microaxial flow pumps are designed for short-term support of left or right ventricular function in patients with cardiogenic shock. Hemolysis is one of the most frequent complications associated with these pumps, occurring at a frequency similar to ECMO (ranging from 5% to 18%).8,9 Here, we present two patients who developed hemolysis during percutaneous transvalvular microaxial flow pump therapy. In both cases, point-of-care (POC) blood gas analysis showed elevated CO-Hb levels, prompting the hypothesis that POC CO-Hb could serve as a bedside parameter for the early detection of hemolysis in this patient population.
Case series
Case 1
A 66-year-old woman presented with cardiogenic shock due to acute ST-segment elevation myocardial infarction (STEMI). Due to severe hemodynamic instability, a percutaneous transvalvular microaxial flow pump was inserted via the left common femoral artery. Following successful recanalization of the proximal left anterior descending artery, the patient was transferred to our intensive care unit (ICU) for further management of cardiogenic shock, including flow pump support, inotropes, and vasopressors. Due to persistent heart failure symptoms and a severely reduced left ventricular ejection fraction (LVEF) of approximately 20%, pump flow was titrated between 3.0 and 3.4 L/min. On the third day, the patient developed signs of hemolysis: serum bilirubin and lactate dehydrogenase (LDH) levels rose while haptoglobin levels declined. Concurrently, CO-Hb levels from regular POC blood gas analyses increased to above 3%. By the fifth day, the patient’s condition stabilized (LVEF ~35%), allowing for the cessation of vasoactive substances. The flow pump was explanted without complications, and CO-Hb levels normalized to 1.4%–1.9% within a few hours post-explantation (Graph 1).
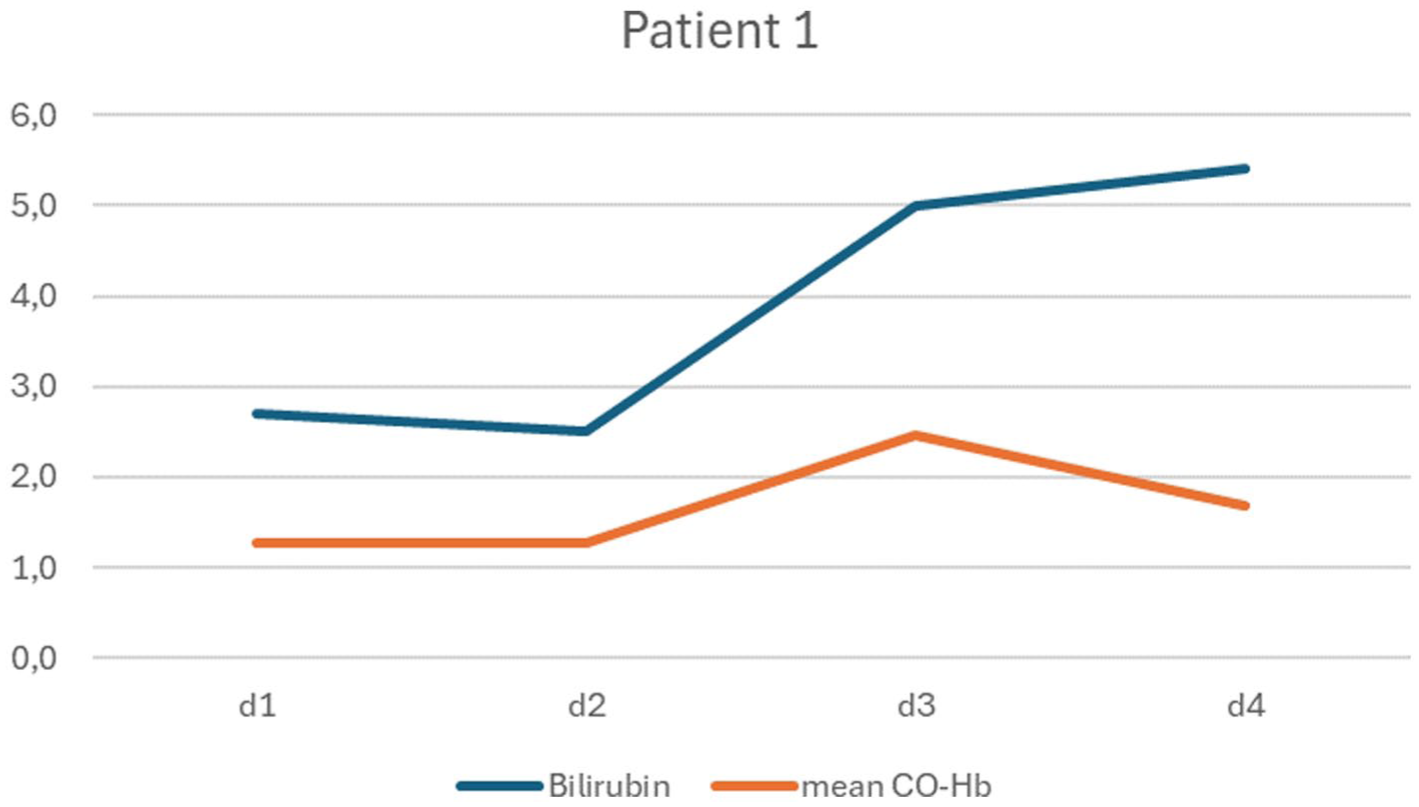
Mean CO-Hb (%) and total Bilirubin (mg/dL) levels over the course of 4 days, first case.
Case 2
A 65-year-old male presented to the emergency department with an acute STEMI. He underwent immediate percutaneous coronary intervention for a thrombotic occlusion of the left main coronary artery. Despite successful recanalization, the patient suffered a cardiac arrest with pulseless electrical activity. Following 5 min of cardiopulmonary resuscitation, echocardiography revealed severe stunning of the left ventricle (LVEF ~10%). A percutaneous transvalvular microaxial flow pump was implanted via the right common femoral artery. On the second day, laboratory results (elevated bilirubin and LDH, low haptoglobin) confirmed hemolysis. To maintain organ perfusion, pump flow was kept above 3.2 L/min. Concurrently, POC analysis showed a significant elevation of CO-Hb to 2.5%. The patient’s cardiac function improved by day three (LVEF ~30%), and the device was successfully explanted on day four. Following explantation, CO-Hb and other hemolytic markers declined steadily (Graph 2).
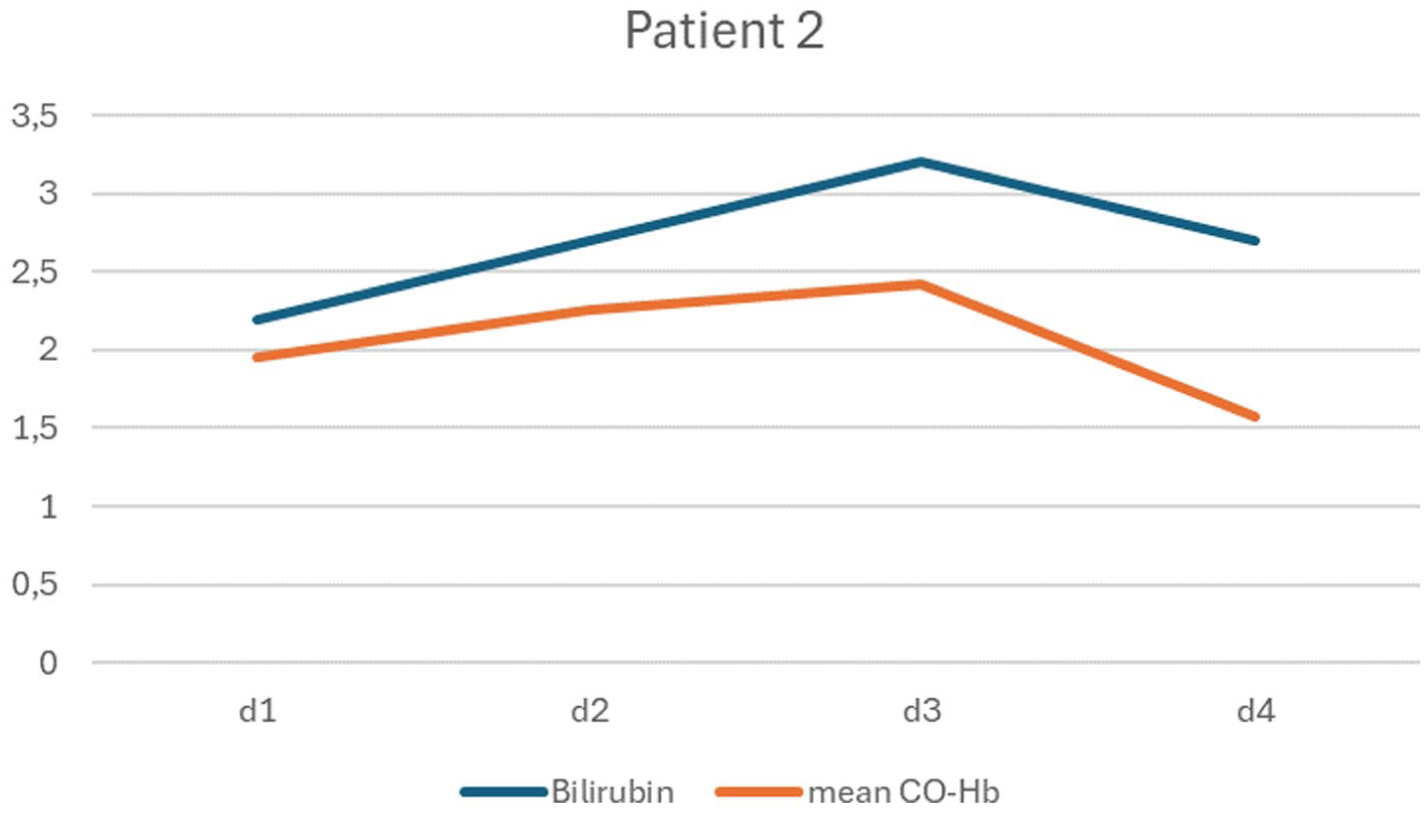
Mean CO-Hb (%) and total Bilirubin (mg/dL) levels over the course of 4 days, second case.
Discussion
While emerging evidence supports the use of CO-Hb as a hemolysis marker in ECMO patients,5–7 data regarding other mechanical circulatory support devices, such as percutaneous transvalvular microaxial flow pumps, remains limited. These two cases suggest a potential correlation between hemolytic activity and CO-Hb levels as measured by POC blood gas analysis. Although plasma-free hemoglobin (pfHb) is the diagnostic gold standard, it is not universally available, and most centers rely on haptoglobin, LDH, and bilirubin, which are typically measured only once daily. In contrast, POC blood gas analyses are conducted multiple times per day in the ICU. Given that hemolysis can progress rapidly and lead to catastrophic outcomes, CO-Hb levels could be an invaluable tool for early bedside detection. In conclusion, our cases highlight the potential of CO-Hb as a readily available, low-cost bedside marker for detecting hemolysis in patients supported by microaxial flow pumps. Further research is warranted to validate CO-Hb as a reliable screening parameter in this clinical setting.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.