
Abstract
Background:
Low flow extracorporeal carbon dioxide removal (ECCO2R) is used to assist in lung protective ventilation. The objective of this study was to compare the characteristics of patients who died in-hospital to those who survived and identify variables pre and during the first 24 h of ECCO2R support independently associated with hospital mortality.
Methods:
This study is a multicenter, multinational, retrospective review of data from the Hemolung Registry between April 2013 and June 2021. The primary outcome was hospital mortality.
Results:
Of the 242 included patients 115 (48%) survived. Prior to ECCO2R initiation and during the first 24 h of ECCO2R therapy, patients who died had a lower PaO2/FiO2 ratio but higher FiO2, respiratory rate (RR), and tidal volumes. Age ((OR: 1.51 (95% CI: 1.06–2.14); p = 0.022), RR (1.92 (1.28–2.87); p = 0.002), and FiO2 (2.33 (1.50–3.62); p < 0.001) were independently associated with increased risk of mortality.
Conclusions:
Age, respiratory rate, and FiO2 during the first 24 h of ECCO2R therapy were independently associated with increased risk of hospital mortality. An ongoing high FiO2 (>0.7) and respiratory rate ⩾25 during the first 24 h is independently associated with higher risk of hospital mortality.
Keywords
Background
Extracorporeal carbon dioxide removal is considered as an intervention to support patients with acute hypercapnic respiratory failure in patients with ARDS or acute exacerbations of chronic lung conditions such as COPD.1–3 Several case studies have shown significant reduction of CO2 with improvement in pH and a reduction in intensity of mechanical ventilation with the use of the low flow venovenous (VV) ECCO2R devices. These studies have prompted randomized controlled trials to investigate ECCO2R for reducing the lung injury and improving survival in patients with ARDS and to avoid intubation and reduce the duration of mechanical ventilation in COPD.4–7 The results of these studies did not show ECCO2R to improve clinical outcomes including mortality or the duration of mechanical ventilation, with suggestion of possible harm with the use of ECCO2R. The randomized controlled studies, although well conducted, had methodological and case selection issues which could have impacted the results.8,9 The inconclusive results of these trials suggest that there continues to be a need for better case selection and timing of instituting ECCO2R. Furthermore, the concept of treatment failure or inadequate “dose” of ECCO2R to achieve treatment goals and improve clinical outcomes has not been previously investigated. One challenge in identifying ECCO2R cases and the appropriate “dose” is the variability in low flow ECCO2R devices in terms of their membrane surface area, blood flow, the limited ability to measure real-time CO2 removal rate and increase CO2 removal to meaningfully reduce the intensity of mechanical ventilation.10,11
Recent studies have identified pre-ECCO2R characteristics that are associated with survival in an effort to improve ECCO2R case selection.12,13 These studies, however, do not provide information regarding characteristics during ECCO2R support that could provide knowledge of the efficiency of ECCO2R in reducing ventilator lung injury and overall prognostication. There are currently no studies that identify characteristics during ECCO2R support that are associated with increased risk of mortality. Such characteristics are important in implying the inadequacy of ECCO2R support and potential treatment failure. Furthermore these characteristics may help in management of ECCO2R and eventually could improve clinical outcomes. Our aim was to identify pre- and during-ECCO2R characteristics that may be independently associated with mortality that could help in case selection as well as future trial design.
Methods
This multicenter, multinational, retrospective, study included patients treated with a single ECCO2R device (Hemolung® RAS, ALung Technologies, Inc., Pittsburgh, PA, USA) for acute respiratory failure and the data was available in the Hemolung Registry.
Data source
The Hemolung Registry is a voluntary registry maintained by ALung Technologies, Inc. (Pittsburgh, PA, USA) and includes de-identified patient data as well as device safety and performance data. Registry data included demographics, diagnosis, comorbidities, and indications for the use of ECCO2R, therapy course including the mechanical ventilation and ECCO2R settings, complications and the outcome of the patients.
In the United States, the Hemolung was used under Food and Drug Administration (FDA) Investigational Device Exemption or Emergency Use Authorization for COVID 19. Outside of the United States, Hemolung therapies were conducted in compliance with each country’s or region’s necessary approval for use at the discretion of the physician caring for the patient.
As the Hemolung Registry Program collects de-identified standard of care data on patients treated with the Hemolung in a retrospective manner, there is no requirement to collect and report data outside of standard of care. Based on U.S. Federal regulation 45 CFS 46 and associated guidance, no IRB review was necessary (and thus no number was assigned) because it did not fall under the board’s guidelines as human subjects’ research.
Inclusion criteria: Patient data was included in the analysis if the following criteria were all met: Data was part of the Hemolung Registry and patients were diagnosed with acute or chronic respiratory failure.
Exclusion criteria: Patients where baseline data, including pH, P/F ratio, PaCO2, and/or outcome data (survived or died) were not available were excluded.
Outcomes
Primary outcome: In hospital mortality.
Secondary outcomes:
Reduction in mechanical ventilation intensity as assessed by respiratory rate, tidal volumes, and peak inspiratory pressure during the first 24 h of ECCO2R therapy between survivors and non survivors.
Safety markers and complications which occurred throughout the entirety of ECCO2R therapy between survivors and non survivors.
Statistical analysis
No sample size calculation was performed and all patients fulfilling the inclusion criteria were included. Continuous variables are presented as median (quartile 25th–quartile 75th) and compared using Wilcoxon rank-sum test, and categorical variables are presented as absolute numbers and percentages and compared using Fisher exact test.
A mixed-effects multivariable logistic regression model was used to identify factors potentially associated with in-hospital mortality. Site was entered as a random effect to account for the clustering effect, all variables were pre-selected based on clinical relevance, available evidence, and were entered in the model without any statistical selection. All results were presented with 95% confidence intervals (95% CI), and there was no imputation for missing data for the main analyses. As a sensitivity analysis, the model was replicated after multiple imputation by chained equations (MICE).
All analyses were performed considering a two-sided hypothesis test, with a significance level of 0.05. Analyses were performed using R v.4.3.3.
Results
Of the total of 278 patients in the registry during the study period, 242 patients were eligible to be included in the analysis (Supplementary Figure 1). The excluded patients (n = 36) did not have baseline and/or outcome data. Of the 242 included patients 115 (48%) survived. The survival was 42.2% with COVID ARDS, 56% with ARDS, and 64% with COPD patients. The percentage of data that was missing in the included patients is presented in Supplementary Table 1. The clinical characteristics and demographic data are presented in Table 1. As shown in Table 1, ARDS was the most common (30%) indication for the use of ECCO2R. Patients who survived were younger than those who died and most had chronic obstructive pulmonary disease as the admission diagnosis. A comparison of type of the ICU and country are shown in Supplementary Table 2.
Comparison of baseline characteristics between survivors and non survivors.
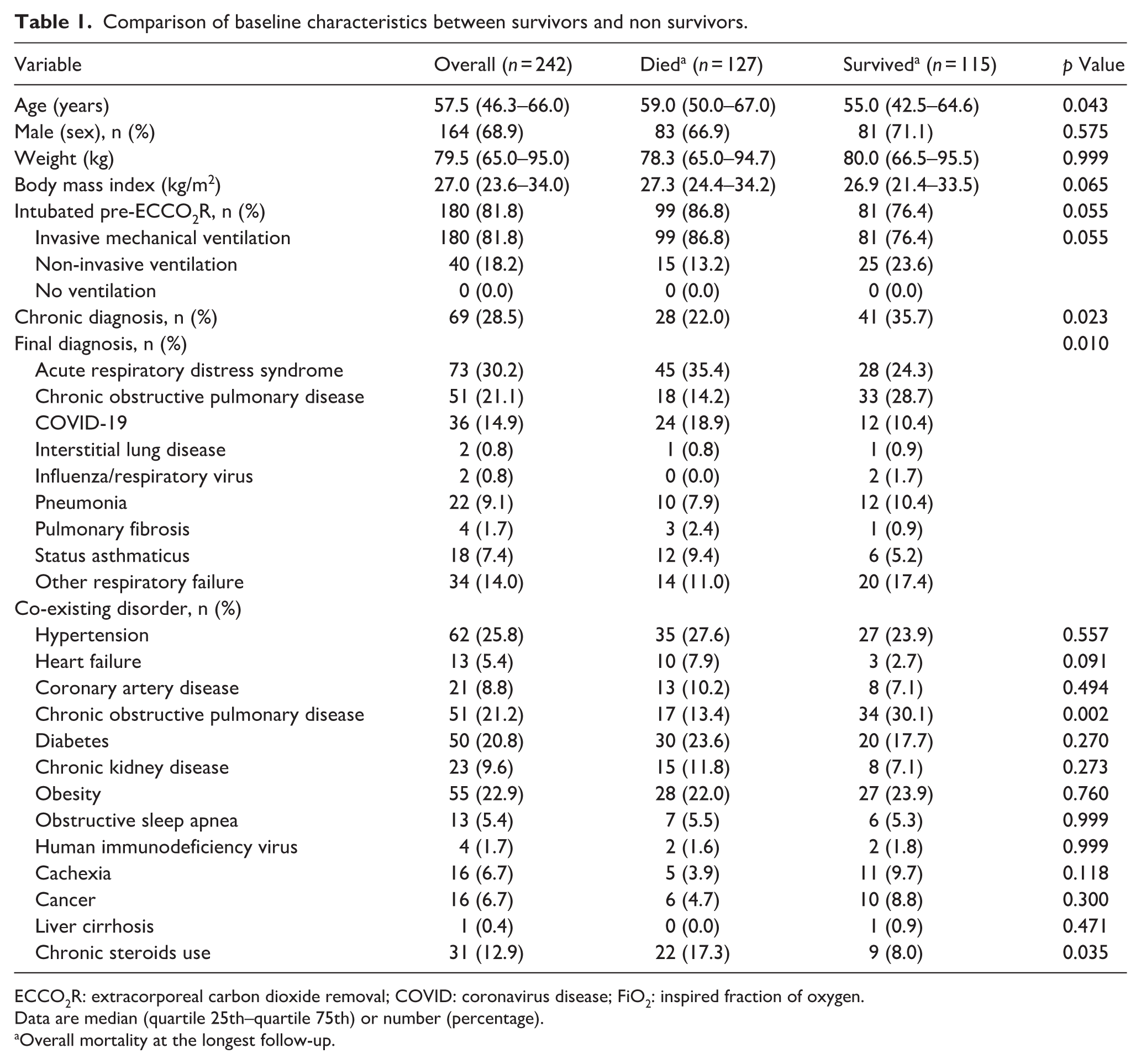
ECCO2R: extracorporeal carbon dioxide removal; COVID: coronavirus disease; FiO2: inspired fraction of oxygen.
Data are median (quartile 25th–quartile 75th) or number (percentage).
Overall mortality at the longest follow-up.
Overall, the mortality was 52%. The comparison of baseline characteristics of patients who survived to those who died at the time of initiation of ECCO2R are shown in Table 2. The PaO2/FiO2 ratio was lower and the FiO2, respiratory rate, positive end expiratory pressure, and peak inspiratory pressures were higher in those patients who died. The baseline pH and PaCO2 levels were comparable between both groups (Table 2). The duration of ventilation prior to initiation of ECCO2R, tidal volumes (adjusted for predicted body weight), and the duration of ECCO2R are comparable between both groups.
Characteristics at ECCO2R initiation.
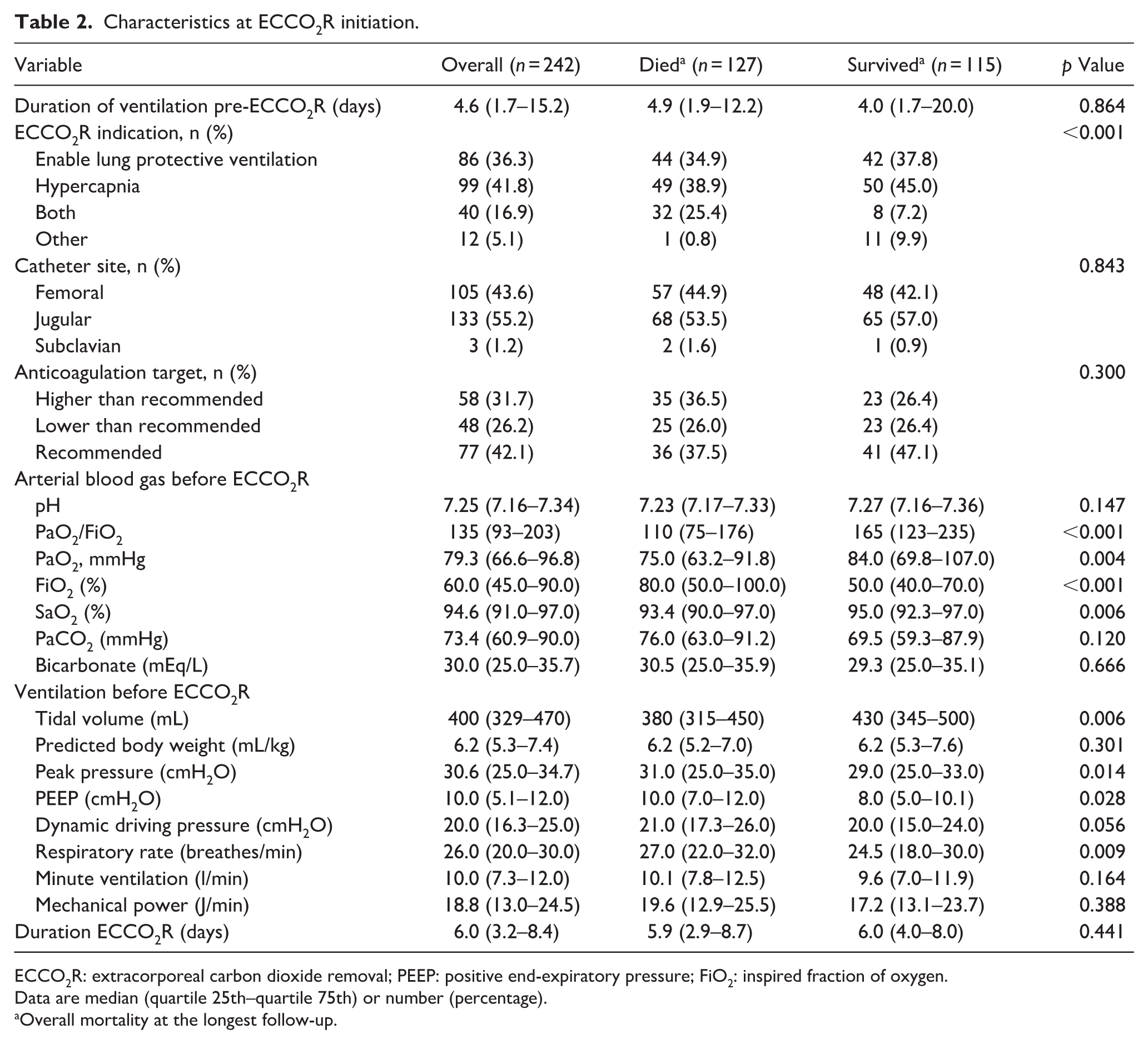
ECCO2R: extracorporeal carbon dioxide removal; PEEP: positive end-expiratory pressure; FiO2: inspired fraction of oxygen.
Data are median (quartile 25th–quartile 75th) or number (percentage).
Overall mortality at the longest follow-up.
Table 3 shows a comparison of the characteristics during the first 24 h of ECCO2R therapy for patients who died and survived. Overall, patients who survived had a higher pH with lower respiratory rate, mechanical power, minute ventilation, and FiO2 requirement during the first 24 h of ECCO2R therapy (Figures 1 and 2). In particular, the respiratory rate and the minute ventilation remained higher at 24 h of initiation of ECCO2R in those patients who died as compared to those who survived (Supplementary Table 3 and Figures 1 and 2). The median ECCO2R blood flow and CO2 removal were comparable between patients who died to those who survived (Table 3 and Supplementary Figure 2). There was no difference in complications attributable to ECCO2R or the need for blood products (Supplementary Table 4) between the survivors and non survivors. The length of ICU stay was higher in patients who survived. Multivariable analysis showed age, median respiratory rate and FiO2 during the first 24 h of ECCO2R therapy to be independently associated with increased risk of mortality (Table 4). These associations persisted after multiple imputations for missing values. The final model also had good discrimination with an area under the curve of 0.798 (95% CI: 0.734–0.862; Supplementary Figure 3).
Characteristics during the first 24 h of ECCO2R.
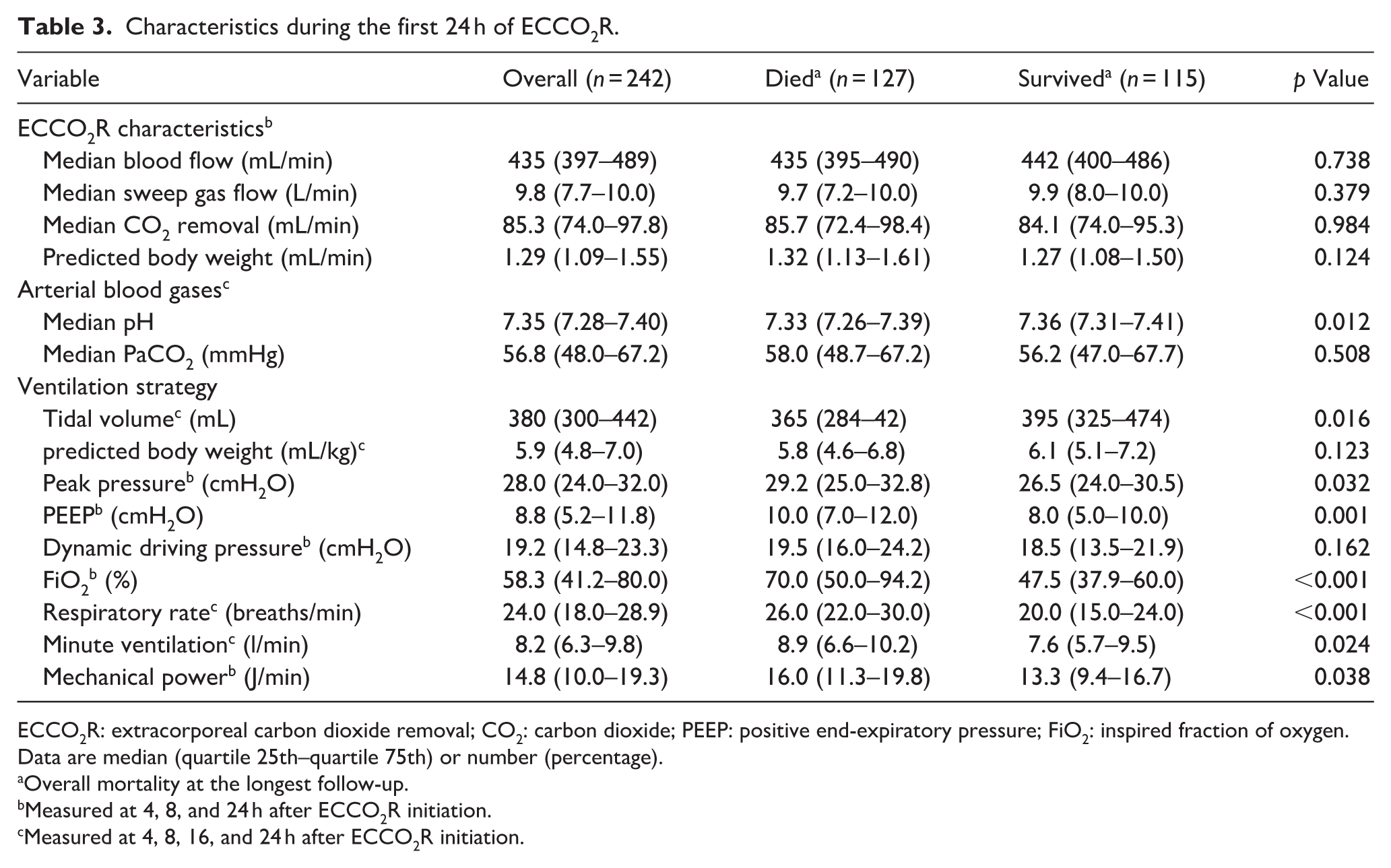
ECCO2R: extracorporeal carbon dioxide removal; CO2: carbon dioxide; PEEP: positive end-expiratory pressure; FiO2: inspired fraction of oxygen.
Data are median (quartile 25th–quartile 75th) or number (percentage).
Overall mortality at the longest follow-up.
Measured at 4, 8, and 24 h after ECCO2R initiation.
Measured at 4, 8, 16, and 24 h after ECCO2R initiation.
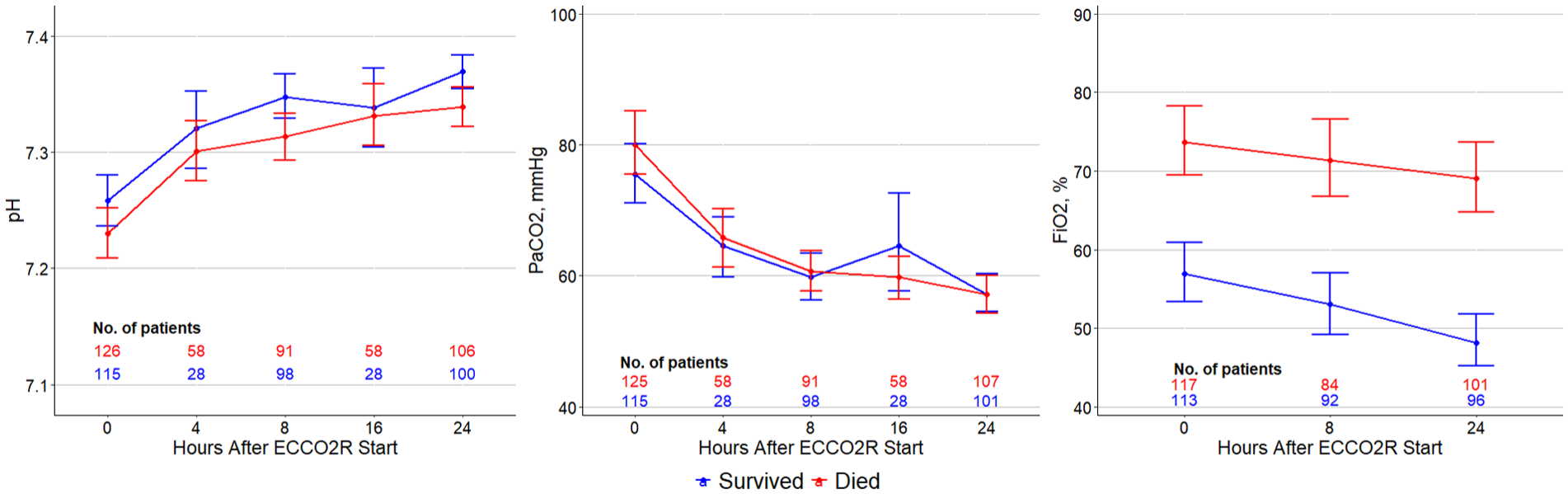
Changes in pH, PaCO2, and FiO2 during the first 24 h between the survivors and non survivors.
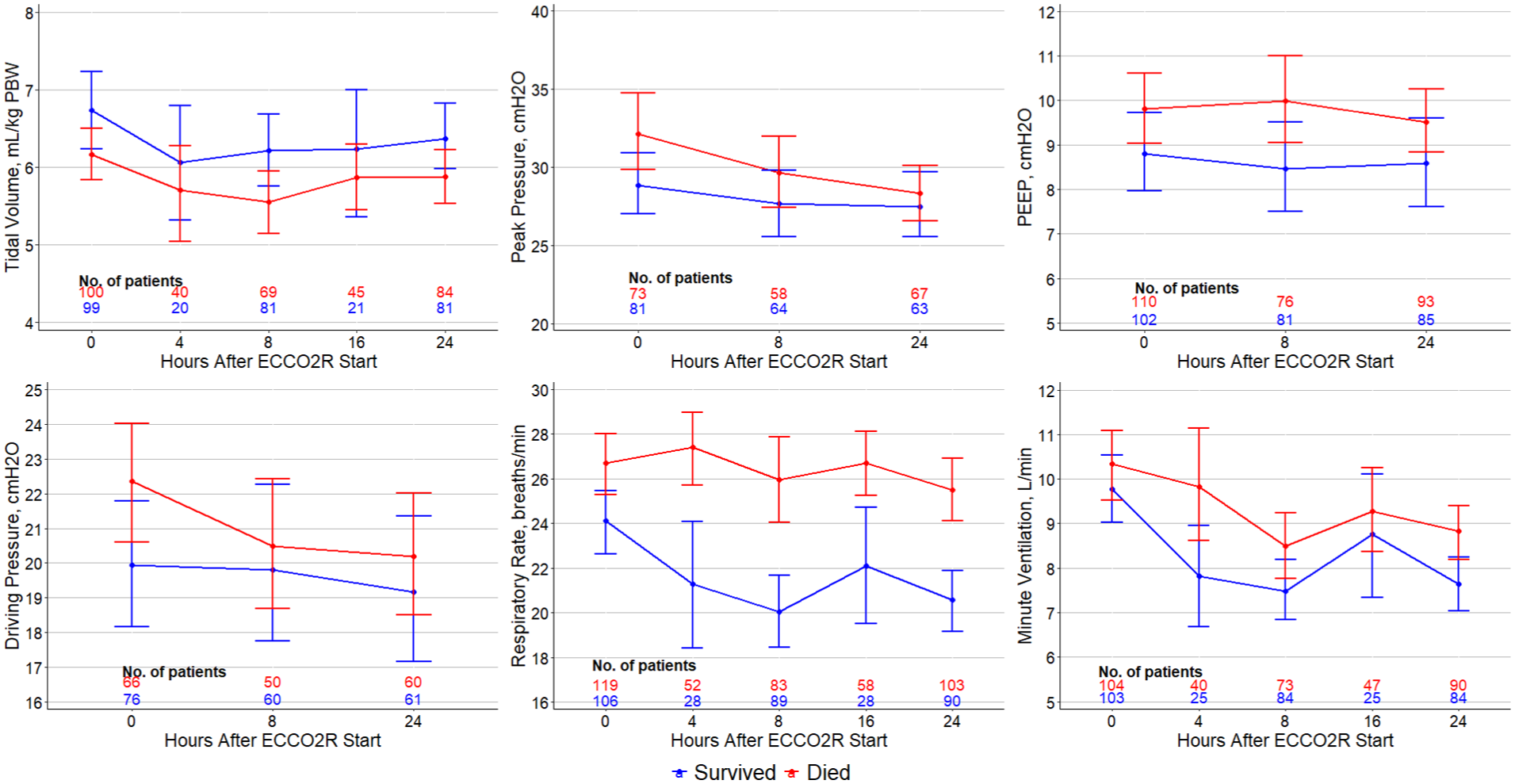
Changes in tidal volume, peak airway pressures, PEEP, driving pressures respiratory rate, and minute ventilation between the survivors and non survivors.
Multivariable model showing the independent association of clinical variables to hospital mortality.
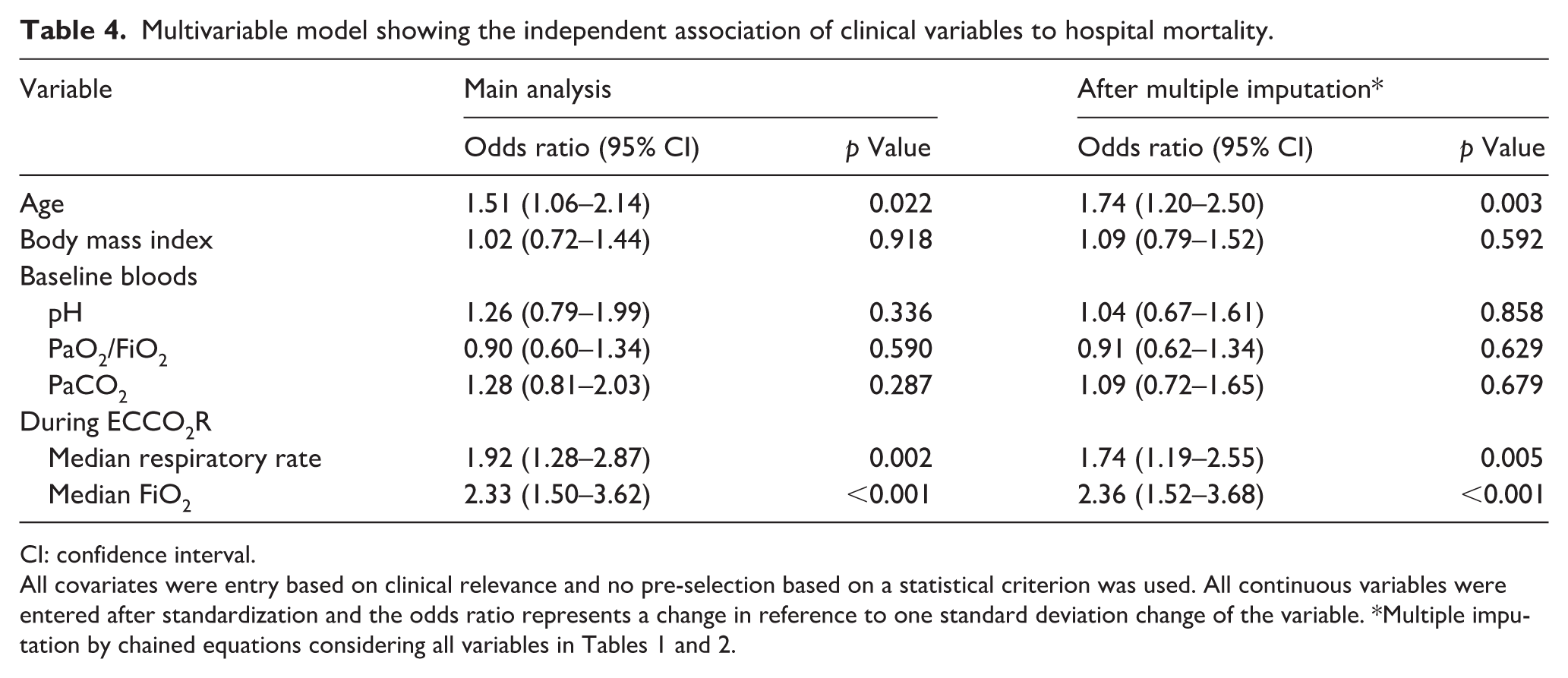
CI: confidence interval.
All covariates were entry based on clinical relevance and no pre-selection based on a statistical criterion was used. All continuous variables were entered after standardization and the odds ratio represents a change in reference to one standard deviation change of the variable. *Multiple imputation by chained equations considering all variables in Tables 1 and 2.
ARDS subgroup analysis
There were 158 patients with ARDS, of which 93 and 64 patients had COVID and non COVID ARDS, respectively. Patients who had COVID related ARDS had a higher mortality than non COVID ARDS (70.2% vs 29.8%; p = 0.001; Supplementary Table 5). The characteristics of patients with ARDS who died as compared to survivors showed that patients who died were older and had lower PaO2/FiO2 (Supplementary Tables 5 and 6). Patients who died also had higher respiratory rates, peak inspiratory pressures, and FiO2 requirements during the first 24 h of ECCO2R (Supplementary Table 7). Multivariable analysis showed respiratory rate during the first 24 h (OR: 2.92 (95% CI: 1.47–5.77); p = 0.002) to be independently associated with increased risk of hospital mortality (Supplementary Table 8).
COPD subgroup analysis
Fifty-nine patients had COPD with a hospital mortality of 35%. Comparison of characteristics of patients who died to those who survived with a diagnosis of COPD showed that patients who died were older, but did not differ significantly with other baseline (Supplementary Table 9). Patients who died had a significantly higher CO2 (median PaCO2: 83 vs 66 mmHg; p = 0.009), though not pH at baseline and a lower pH (median pH: 7.36 vs 7.4; p = 0.038) during the first 24 h of ECCOR initiation (Supplementary Tables 10 and 11). Multivariable analysis (after imputations) showed age (OR: 2.90 (95% CI: 1.01–8.33); p = 0.047) and median FiO2 during the first 24 h of ECCO2R (OR: 3.65 (1.10–12.13); p = 0.035) to be independently associated with increased risk of hospital mortality (Supplementary Table 12).
Discussion
Key findings
This multicenter, multinational study that included 242 patients treated with a single ECCO2R device for respiratory failure showed that ARDS was the most common indication for the use of ECCO2R in current clinical practice. The mortality of the overall patient cohort was high (52%), with a 44% mortality in ARDS, 71% in C-ARDS, and 35% in COPD. Multivariable analysis showed increasing age and respiratory rate during the first 24 h of ECCO2R therapy to be independently associated with mortality in ARDS. The mortality in ARDS14,15 and C-ARDS 16 in this study are high but similar to that reported in the wider literature. Patients with COPD who died had a higher CO2 at baseline and a lower pH at 24 h. Multivariable analysis showed age and FiO2 during the first 24 h to be independently associated with mortality in patients with COPD. The mortality in the COPD group is similar to the reported mortality in literature for patients with COPD admitted to the ICU with increasing age and the need for mechanical respiratory support both being independent risk factors for mortality.17,18
Relationship with previous studies
Several studies have shown improvement in physiologic mechanical ventilator parameters, including PaCO2/pH and minute ventilation, with ECCO2R therapy. However, the impact of these physiological improvements, on overall reduction in need for or duration of mechanical ventilation, organ failure free days or mortality remains unclear.19,20
ECCO2R devices that are currently available in clinical practice vary significantly in their efficiency and complication profile.10,21–25 The CO2 removal rate of these devices differs significantly and is based on blood flow and fiber bundle geometry. In the secondary analysis of SUPERNOVA study the “low extraction devices” could only achieve 4 mL/kg PBW target in 55% and 64% of the patients whereas “high CO2 extraction devices” could achieve the 4 mL/kg PBW target in 90% and 92% of the patients at 8 and 24 h post ECCO2R initiation. 24 Importantly, high versus low extraction was defined based on extracorporeal blood flow rate and not on measured CO2 removal rates the devices achieved in the study. It is important to appreciate that higher blood flows have a greater oxygen delivery and given the higher mortality in patients with lower P/F ratio in ARDS, one implication of this study is that higher blood flow devices, or ECMO, should be considered in patients with significant hypoxemia or severe ARDS (P/F ratio <100 mmHg). There is limited data on the efficacy of the low flow, low CO2 extraction devices in achieving the ARDSNet recommended, lung protective ventilation tidal volumes of ⩽6 mL/kg PBW in patients where hypercapnic acidosis restricts tidal volume reduction to <6 mL/kg PBW. 26 However, the implications of such reduction on mortality remains unclear.
In addition to the tidal volumes, 27 the other ventilator parameters that are related to ventilator induced lung injury and the overall outcome include driving pressures and mechanical power.28,29 Respiratory rate is a prognosticator in patients with respiratory failure and is a component of mechanical power.29,30 Our study did not show a difference in driving pressures between survivors and non survivors, but the respiratory rate was higher pre ECCO2R and during the first 24 h on ECCO2R in patients who died. The current ECCO2R consensus on the initiation of ECCO2R is ⩾25 breaths/min in patients with ARDS with no defined rate for patients with COPD. 31 The ECCO2R treatment target based on the consensus is to aim for a respiratory rate of <20 breath/min in both ARDS and COPD patients. 31 Our results further reinforce the consensus targets where respiratory rate was an independent predictor of mortality and patients who died had a respiratory rate of 27 breaths/min at ECCO2R initiation and 25 breaths/min at 24 h of ECCO2R therapy.
Study implications
The results of this study have implications for clinical application of ECCO2R as well as future research.
Case selection and application of ECCO2R: While there are consensus statements on the practice of ECCO2R, there are limited clinical data that could help in case selection as well as practice of ECCO2R. Our study provides further data to assist in case selection and device management. It identified high FiO2 requirement prior to initiation and an ongoing high FiO2 requirement and respiratory rate and minute ventilation at 24 h during ECCO2R may reflect ongoing ventilatory demand, impaired gas exchange, and limited extracorporeal CO2 clearance relative to metabolic requirements, thereby indicating a mismatch between patient needs and the support provided by ECCO2R.
Low flow ECCO2R devices may support reduction in driving pressure and tidal volumes in patients with hypercapnic respiratory acidosis. However the efficacy and applicability of these devices to improve clinical outcomes are likely to be different in ARDS (where hypercapnic acidosis may be associated with hypoxemia) as compared to COPD or asthma patients where hypercapnic acidosis may not be associated with significant hypoxemia. The study by Monet et al. 32 including ARDS patients on low blood flow (less than 500 mL/min) and high blood flow (greater than or equal to 1000 mL/min) ECCO2R showed that ultra-lung protective ventilation with reduction in mechanical power was feasible with higher blood flow rates. Patients who received ultra-lung protective ventilation also had higher 90-day survival rate (63% vs 18%; p = 0.0004). 32
Our study had 92 patients with COVID-19 ARDS and 64 patients with non COVID-19 ARDS. The mortality in COVID-19 ARDS was significantly higher with COVID-19 ARDS (71%) as compared to non COVID-19 ARDS (44%). Studies comparing COVID-19 and non-COVID19 ARDS patients have shown that there were differences in inflammatory biomarkers 33 as well as clinical outcomes including longer duration of mechanical ventilation33,34 and mortality 35 in COVID-19 ARDS. Studies that have used ECCO2R in COVID-19 are limited with low sample size and focused on physiological endpoints such as reduction of PaCO2 with ECCO2R.36,37 Given a higher mortality with COVID-19 ARDS in our study, further research focusing on clinical endpoints is required to evaluate the role of ECCO2R in COVID-19 ARDS.
In COPD patients requiring intensive care, there is a significant increase in mortality associated with increasing age, increasing severity of illness and development of respiratory failure requiring mechanical ventilatory support.17,18 Given the lack of demonstrated benefit of ECCO2R in studies involving patients with COPD to date, further work is required to define a patient population who may benefit from ECCO2R as well as to optimize its application with regard to blood flow rates and CO2 removal for preventing the need for mechanical ventilation as well as reduction in the duration of mechanical ventilation and mortality.
Strengths and limitations
Strengths
Our study has several strengths. It provides real-world application of ECCO2R and characterizes the type of patients who are currently managed with ECCO2R. Our data has both physiological outcomes as well as patient centered outcomes, providing significant clinical insights to the case selection. It is the first study that provides insights into the dynamic time dependent clinical variables (such as FiO2 and respiratory rate) during the first 24 h of ECCO2R therapy that could suggest the inadequacy of ECCO2R support. The results of this study can assist in routine clinical practice as well as in future clinical trials.
Limitations
Our study has several limitations due to the retrospective nature of this study. Given the observational nature of this study, some variables had a high rate of missing data (Supplementary Table 1). The data available on blood gases and ventilator requirements were limited to the first 24 h of ECCO2R support. Our study included three diagnostic groups. While this reflects real-world ECCO2R use, it may obscure condition-specific associations in the primary analysis. Subgroup analyses were limited by small sample sizes and should be interpreted cautiously. Accordingly, these findings represent overall signals within a mixed population and highlight the need for larger, diagnosis-specific studies. Nevertheless, our results provide contextual and hypothesis-generating insights into the use of ECCO2R in real-world practice. We have used the longest survival data that was available to hospital discharge, however detailed initiation criteria for ECCO2R, severity of illness scores, such as APACHE III, SOFA, or SAPS, use of tracheostomy and outcome data such as ICU‑free days, and ventilator‑free days were not available.
We did not have data on the use of other adjunctive supportive therapies including prone position ventilation, corticosteroids, neuromuscular blockade, inhaled nitric oxide, or predefined criteria for escalation to ECMO when the support of ECCO2R was insufficient. Only patients submitted to the registry with complete baseline blood gas and outcome data were included, which may have introduced selection bias. In addition, the availability or lack of availability of ECMO particularly during the COVID‑19 pandemic may have influenced decisions regarding ECCO2R initiation and contributed to further selection bias.
Conclusion
The mortality in patients receiving ECCO2R was high but in keeping with the literature across all three groups. Age, respiratory rate and FiO2 during the first 24 h of ECCO2R therapy are independently associated with increased risk of mortality. An ongoing high FiO2 (>0.7) and respiratory rate ⩾25 breaths/min suggest a more severe underlying disease process or a limited response to therapy. These parameters, may help identify patients at higher risk of poor outcomes. However, given the observational design, cohort heterogeneity, and lack of prospective validation, these findings should be considered hypothesis generating. Further prospective studies need to be undertaken to define a population of patients who may benefit most from ECCO2R.
Supplemental Material
sj-docx-1-jao-10.1177_03913988261461123 – Supplemental material for Association of clinical characteristics to mortality in acute respiratory failure patients treated with ECCO2R
Supplemental material, sj-docx-1-jao-10.1177_03913988261461123 for Association of clinical characteristics to mortality in acute respiratory failure patients treated with ECCO2R by Ravindranath Tiruvoipati, Alexandra May, Ary Serpa Neto, Bindu Akkanti, Kha Dinh, Nicholas A Barrett and Steven A Conrad in The International Journal of Artificial Organs
Footnotes
Acknowledgements
Not applicable.
List of abbreviations
ARDS acute respiratory distress syndrome
COPD chronic obstructive pulmonary disease
ECCO2R extracorporeal carbon dioxide removal
ECMO extracorporeal membrane oxygenation
FDA Food and Drug Administration
ICU intensive care unit
IMV invasive mechanical ventilation
IQR interquartile range
MICE multiple imputation by chained equations
PaCO2 partial pressure of carbon dioxide in arterial blood
PaO2 partial pressure of oxygen in arterial blood
SAPS Simplified Acute Physiology Score
SOFA Sequential Organ Failure Assessment
Author contributions
RT: conceptualization, methodology, assisting in analysis, original draft writing, review and editing. AM: data curation, methodology, assisting in analysis, review and editing. ASN: data analysis, revision and editing. BA: methodology, draft review, revision and editing. KD: methodology, draft review, revision and editing. NAB: methodology, draft review, revision and editing. SAC: methodology, draft review, revision and editing. All authors read and approved the final manuscript.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Ravindranath Tiruvoipati was an invited speaker at several Baxter/Vantive sponsored meetings and have received speaking fee. He also received investigator initiated research grants provided by Baxter Healthcare Pty. Ltd. and Fisher and Fisher and Paykel HealthCare Limited. Alexandra May was an employee of ALung Technologies, Inc. Bindu Akkanti and Steven A Conrad received consulting fees from ALung Technologies, Inc. Nicholas A Barrett received institutional research funding from ALung Technologies, Inc. Ary Serpa Neto and Kha Dinh have no conflicts to declare.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The Hemolung Registry Program collects de-identified standard of care data on patients treated with the Hemolung in a retrospective manner, there is no requirement to collect and report data outside of standard of care. Based on U.S. Federal regulation 45 CFS 46 and associated guidance, no IRB review was necessary (and thus no number was assigned) because it did not fall under the board’s guidelines as human subjects’ research.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.