
Abstract
Introduction:
Emphysematous pyelonephritis is a rare necrotizing infection of the kidney with a poor prognosis. If it occurs in patients with a reduced general condition, this infection is life threatening. Early diagnosis is made by computed tomography. Treatment options are drainage and intensive care or immediate nephrectomy in severe cases.
Case description:
A 73-year-old woman in a poor general condition presented with a fulminant urosepsis. Computed tomography revealed an impressive abscess formation of the right kidney with free air retro and intraperitoneal. The diagnosis of emphysematous pyelonephritis was made. Besides septicemia, she had a multiorgan failure including kidney and liver function deterioration. Nephrectomy was performed immediately. The postoperative course was successful with a complete stabilization of the kidney and liver function and reconvalescence of the patient.
Discussion:
The widespread availability of imaging techniques leads to early diagnosis and a reduction of mortality of renal and periphrenic abscesses and even of emphysematous pyelonephritis. However, severe cases have a poor outcome and require aggressive and immediate therapy. Besides systemic antibiotic therapy and percutaneous and surgical drainage, radical nephrectomy is a viable therapy option and should be performed immediately in patients with several risk factors, poor prognosis, and extensive findings.
Conclusion:
Radical nephrectomy being performed immediately seems to be the optimal management in patients with acute emphysematous nephritis and urosepsis.
Introduction
Emphysematous pyelonephritis (EPN) is an acute severe necrotizing infection of the renal parenchyma and its surrounding tissue and leads to gas production in the renal parenchyma, collecting system, or perirenal tissue. 1 Gram-negative bacteria like Escherichia coli and Klebsiella pneumoniae are commonly isolated pathogens.2–5 EPN has a life-threatening potential and therefore needs special attention. Until the late 1970s, mortality rate was up to 78%. Over the last two decades, a reduction of the mortality rate to 21% could be achieved by improved management techniques. 5 Predisposing factors are diabetes mellitus, drug abuse, neurogenic bladder, alcoholism, and urinary tract abnormalities. Up to 95% of patients with EPN have underlying uncontrolled diabetes mellitus.5–7 Renal insufficiency, old age, and lethargy are associated with a poor prognosis. Computed tomography (CT) is the gold standard for diagnosis. 8 The treatment strategies include medical management alone, medical management and percutaneous drainage, medical management and emergency nephrectomy, and medical management and percutaneous drainage and emergency nephrectomy. 9
In this article, we report a case of a fulminant urosepsis due to EPN in an old-aged woman in a poor general state.
Case description
A 73-year-old female patient from Munich has been transferred to the emergency department of the Ludwig Maximilians University of Munich Campus Großhadern with the final diagnosis of EPN of the right kidney. She initially presented in the clinic Augustinum of Ludwig Maximilians University Munich with back pain and reduction of the health condition and then was transferred to Großhadern as soon as the diagnosis was made.
In the medical history, a ductal pancreatic cancer (pT3, pN0 (0/30), L0, V1, Pb1, G3, R0, ED 12/15) is treated by Whipple surgery and adjuvant chemotherapy. The last infusion took place on 11 July 2016. In a CT for staging conducted in July 2016, there was no evidence of disease.
In 2007, breast cancer (pT1, pN0 (0/19), Mx, R0, Gx, ERO, PRO, Her2/neu neg.) was treated by neoadjuvant chemotherapy and breast-conserving surgery as well as irradiation therapy.
A number of cardiovascular risk factors existed such as coronary heart disease with status post percutaneous transluminal coronary angioplasty (PTCA) and stenting in 2014, diabetes mellitus, and arterial hypertension.
The patient was transferred to the emergency room by ambulance. She was accompanied by her daughter. The anamnesis had to rely on the daughter as the patient was no longer orientated. The reason for the ambulance call was a reduction of the health condition as well as back pain that occurred within 1 week. Since 2 days, the patient had not eaten and no fluid intake. She had no fever.
The 73-year-old patient presented in a reduced general condition and in an extremely poor nutritional and dehydrated status. She showed a positive shock index with a heart rate of 130/min and a blood pressure of 90/50 mmHg. The weight was 50 kg, temperature 37.6 C, and the breathing rate 30/min. The abdomen was soft, the borborygmus sparely. The blood test indicated a septic constellation with a leukocyte count of 38 g/L, a C-reactive protein (CRP) of 22.0 mg/dL, and disseminated coagulation factors. The creatinine level of 4 mg/dL indicated an acute kidney failure, and elevated liver enzymes (bilirubin of 2.8 mg/dL) might signify for a multiorgan dysfunction. Blood gas analysis showed a metabolic acidosis (pH 7.19, bicarbonate 10), and lactate was 11 mmol/L.
CT showed an impressive image with an abscession of the whole right kidney with free air retro and intraperitoneal (Figure 1). In sum, it showed the picture of an EPN.
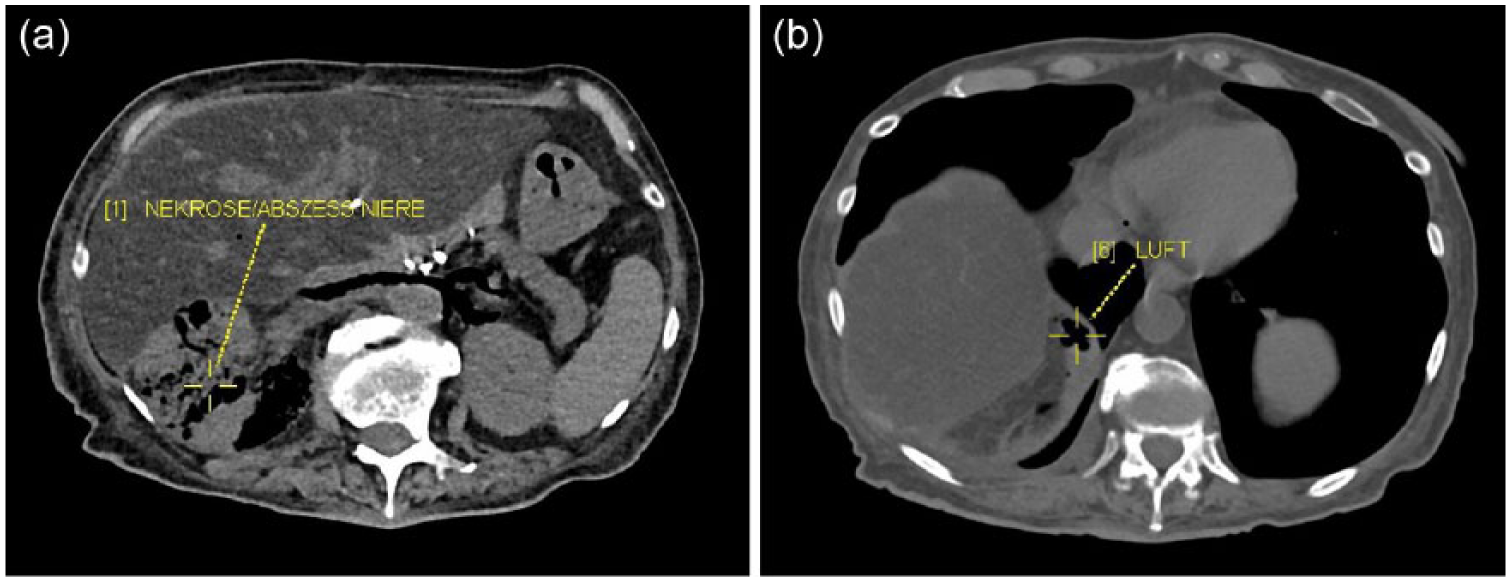
Computed tomography shows an abscess of the whole right kidney (a) with free air retro and intraperitoneal (b).
The patient was transferred to the Department of Urology in Ludwig Maximilians University of Großhadern for further therapy.
The patient underwent a radical nephrectomy of the right kidney immediately. Figure 2 shows an image of the kidney as it presented intraoperatively. On the surface, little yellow spots were visible. Swabs of the kidney were taken, and a pathological examination of the organ was initiated.
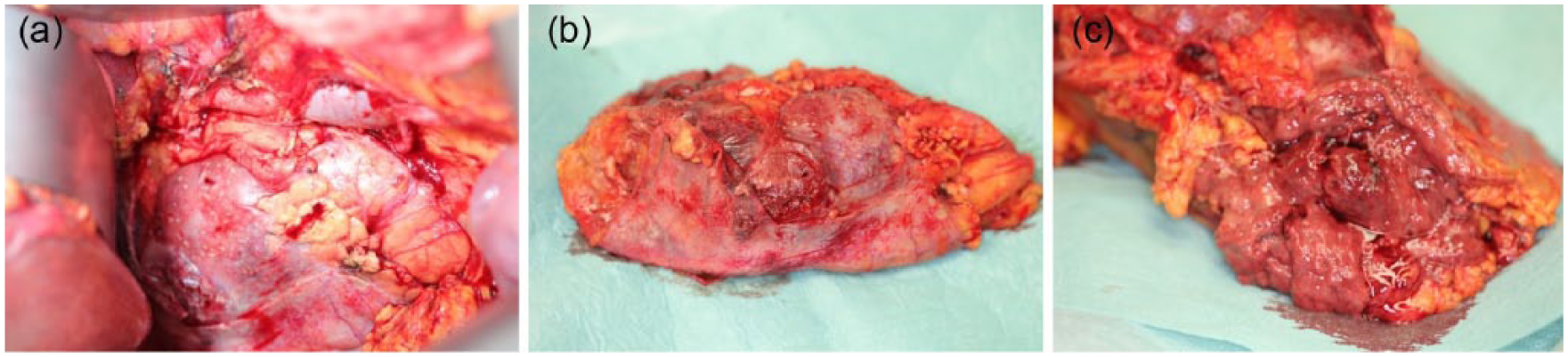
(a–c) Intraoperative appearance of the right kidney: little yellow spots on the surface are visible.
Postoperatively, the patient was treated on the intensive care unit. Calculated antibiotic therapy with piperacillin and combactam led to a reduction of infectious parameters. The kidney and liver function recovered. The coagulation factors stabilized. The microbiological examination of the kidney revealed the growth of E. coli sensitive to the existing antibiotic therapy. The pathological examination resulted in the presence of abscesses with destruction of the parenchyma and bacterial infection as well as spreading of the purulent-abscessed infection into the perirenal fat. There was no evidence of malignancy (see Figure 3).
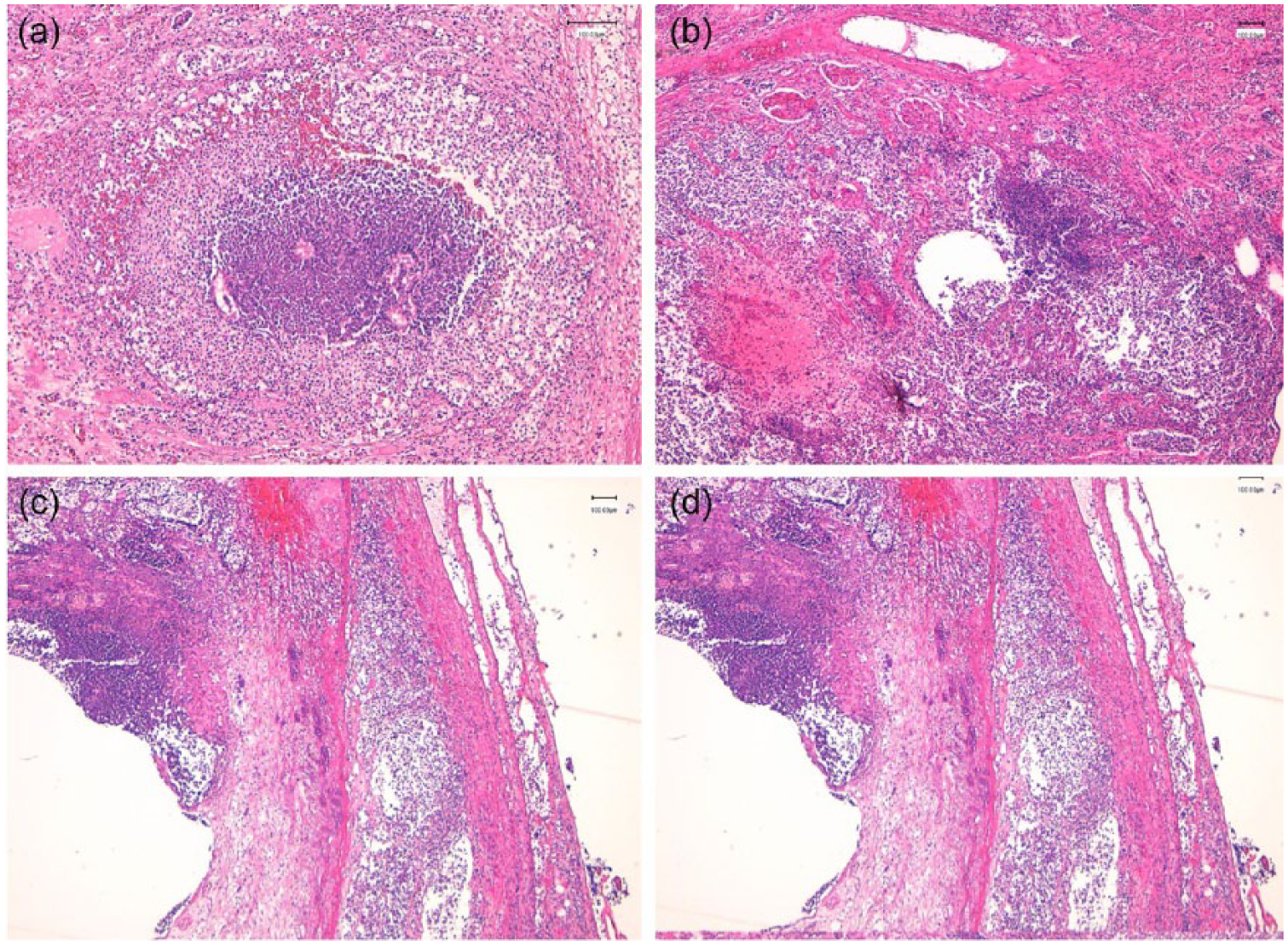
Pathological examination resulted in the presence of abscesses (a, b) with destruction of the parenchyma and bacterial infection as well as spreading of the purulent-abscessed infection into the perirenal fat (c, d).
A further CT showed a fluid formation epidiaphragmal subpleural as well as in the right renal bed. Two drains have been inserted. In the microbiological examination of the fluid, the growth of E. coli was detected corresponding to the microbiological findings of the kidney.
Finally, the patient could be extubated, was stable, and recovered slowly but continuously. She was transferred to a regular urological ward. Further imaging control could exclude further fluid formation, so the drains have been removed. The antibiotic therapy was oralized to Augmentan. Finally, the patient has been discharged in freedom of symptoms.
Discussion
The advances in imaging techniques have lead to earlier diagnosis of EPN. With the widespread use of CT and magnetic resonance imaging (MRI), mortality rate has been reduced, but still is 21%.5,9
In the current literature, only few cases of serious EPN are described. Kawano et al. reported of three cases of serious renal infection. One of them died from EPN, despite nephrectomy performed on the day of diagnosis. Exitus letalis occurred 2 months later. Symptoms were present since 13 days until diagnosis was made.
Abdul-Halim et al. 10 compared management strategies of severe EPN in seven patients from 1996 to 2004. Nephrectomy was performed in three patients, delayed nephrectomy in two patients, incision and drainage in one patient, and immediate percutaneous drainage in one patient. Patients who had incision and drainage or percutaneous drainage presented recurrent periphrenic abscesses requiring surgical intervention and leading to longer hospital stay. Patients after immediate nephrectomy recovered more quickly and had no complications postoperatively.
In our case, a patient presented with several risk factors: old age, poor health condition with a history of cancer and current chemotherapy, diabetes mellitus, marasmus, and renal failure. Imaging showed EPN. Multiorgan dysfunction has been present. Considering all these factors and the final outcome, the aggressive treatment by immediate nephrectomy seemed to be the right treatment option.
To our knowledge, no case has been reported which describes that kind of clinical severity and that impressive extent of EPN found radiographically and intraoperatively.
Conclusion
Immediate radical nephrectomy is a viable treatment option in EPN, leading to a septic condition. Thus, the indication for nephrectomy should be made generously as otherwise the mortality rate is high.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.