
Abstract
Aim:
Assessing the incidence of immediate postoperative complications and 90-day mortality in high-risk patients who have undergone radical cystectomy; evaluating the correlation between preoperative conditions and surgery outcomes.
Materials and methods:
This is a monocentric retrospective observational study in which data of 65 patients have been analyzed.
High-risk criteria:
(a) Age ≥75 years, (b) obesity, (c) age-adjusted Charlson Comorbidity Index ≥8, (d) anemic status, and (e) pT ≥3. More than 50% of patients had two or more “high-risk” indicators. Postoperative complications were assessed through Clavien–Dindo classification.
Results:
Average age of patients was 70.4 years, average age-adjusted Charlson Comorbidity Index was 5.8, and average body mass index was 27.5. In 28% of patients, no complications arose, while in 46% grades I–II complications according to Clavien–Dindo occurred, in 23% grades III–IV complications occurred, and in 3% of the patients, death arose in the immediate postoperative period (grade V). Overall, 90-day mortality rate after surgery was 12.3%. The age ≥75 years and an age-adjusted Charlson Comorbidity Index score ≥8 have shown to be risk factors for the onset of severe complications (odds ratio = 3.54, p = 0.028 and odds ratio = 4.7, p = 0.026), while preoperative anemic status was a risk factor for complications in general (odds ratio = 4.1, p = 0.015). No analyzed parameter was a predictor of 90-day mortality (p > 0.05).
Conclusion:
Immediate postoperative complications and 90-day mortality in radical cystectomy in high-risk patients remain significant, but still in line with the data in the literature on comparable populations. Some of the preoperative parameters were able to predict the outcomes of the intervention with regard to the onset of complications but not to the 90-day mortality.
Introduction
Radical cystectomy (RC) is a major urological operation that involves the removal of bladder, prostate and seminal vesicles in men and of the bladder, uterus, adnexa uteri and anterior wall of the vagina in the women (anterior pelvic exenteration); it also involves the execution of lymphadenectomy. RC is the therapeutic gold standard for muscle-invasive bladder cancer, which accounts for approximately 20%–30% of the total number of diagnosed bladder cancers. Bladder cancer occurs more frequently in males aged over 50 years. However, the population affected by this pathology is extremely heterogeneous in both clinical history and tumor characteristics. The prognosis of the patient undergoing RC is very variable. It depends on many factors including age and clinical conditions of the patient and the stage of the tumor. Thanks to progresses in the surgical and anesthesiologic fields, today it is possible to operate with this type of intervention also “high risk” considered subjects.
Aim of the study and limits
To define the following in high-risk patients with bladder cancer subjected to RC:
- The “high-risk” indicative criteria;
- The incidence and severity of complications emerging in the immediate postoperative period (hospitalization);
- Total 90-day mortality after surgical intervention;
- The correlation between the outcomes of surgery in terms of postoperative complications and 90-day mortality with specific preoperative conditions of patients.
The limits of the study are as follows:
- The number of analyzed patients is not big.
- The inability to trace back to the total clinical and instrumental data of the patients studied, as this is a retrospective study based on the analysis of the data obtained from the evaluation of medical and outpatient records.
- The inability to determine undoubtedly the causal link among the onset of complications in postoperative period, 90-day mortality, and RC surgery.
Materials and methods
This is a monocentric retrospective observational study in which medical records and outpatient reports have been analyzed in order to obtain the clinical data of 65 high-risk patients with bladder cancer and subjected to RC between 2011 and 2016, identified after consulting the COU register of Urology of the Palermo University Hospital “Paolo Giaccone.”
The study focuses on evaluating the outcomes of RC in “more complex” and/or “fragile” patients, that is, those with unfavorable conditions that could make convalescence more difficult and the outcome worse, compared to those who have a better performance status. The classification criteria by which patients undergoing RC were considered to be “high risk” were chosen because for each one of them different and often several studies exist in the literature, which investigate and demonstrate the role as a predictor for the onset of postoperative complications and/or mortality after RC. High-risk patients were defined as having one or more of the following characteristics:
Age ≥75 years;
Obesity;
Age-adjusted Charlson Comorbidity Index (ACCI) ≥8;
Preoperative anemic status (Hb < 13 g/dL in male and Hb < 12 g/dL in female);
pT ≥3.
The extent of patients’ comorbidity prior to surgery was measured by the ACCI score. Postoperative complications have been sought through the study of clinical records of patients who have undergone surgery, and therefore refer to the period of patient hospitalization; in fact, complications that emerged after the patient’s discharge were not reported for incompleteness of data. Postoperative complications have been defined and classified according to the Clavien–Dindo classification,1,2 as suggested by international guidelines. 3
Ninety-day mortality from surgery was evaluated by consulting patient outpatient registers by contacting the urologists who had operated and followed the patients and/or contacting the patient’s domicile.
Results
After consulting the register and selecting patients through evaluation of the “high-risk classification” criteria, 65 patients undergoing RC for bladder cancer in the period 2011–2016 were selected. More than 50% of patients had two or more of the “high-risk” criteria. The principal patient characteristics are shown in Table 1.
Principal patient characteristics.
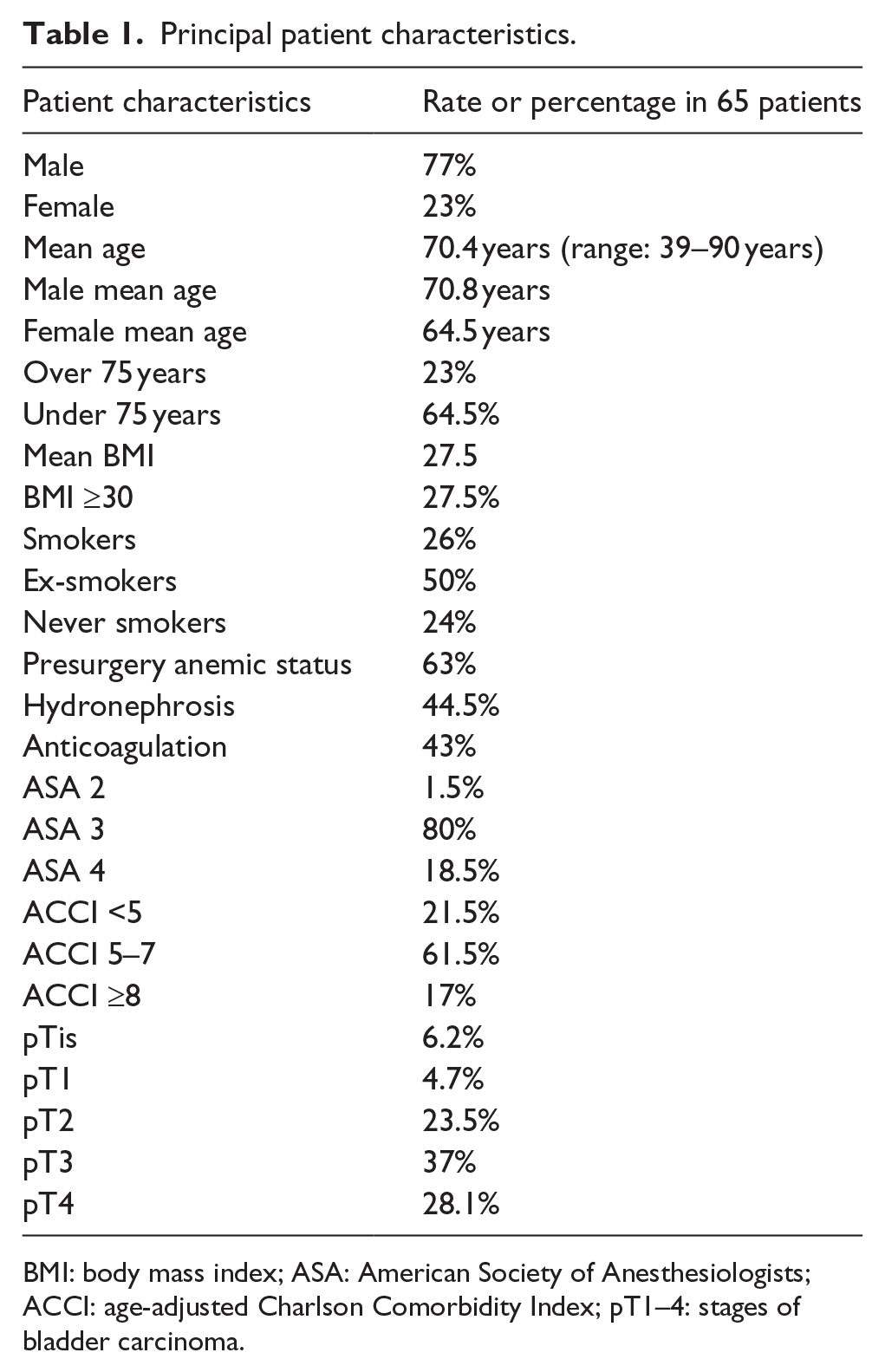
BMI: body mass index; ASA: American Society of Anesthesiologists; ACCI: age-adjusted Charlson Comorbidity Index; pT1–4: stages of bladder carcinoma.
RC with traditional “open” technique was performed in all patients and urinary derivations carried out were: ureterocutaneostomy in 49%, ureteroileocutaneostomy according to Bricker in 32.5% of cases, orthotopic neobladder in 17% of cases (in eight patients with technique according to Studer and in three patients VIP 2), and no urinary derivation was produced in one patient because of terminal IRC in dialysis treatment. Histologically, almost all of the neoplasias were transitional cell carcinomas, in four cases they were squamous carcinoma, in four cases neuroendocrine tumors to small cells, and in one case bladder adenocarcinoma. The percentage of complications that occurred after RC is shown in Figure 1. The need for urinary derivation washings for mucus and/or clots that hinder urine outflow and blood transfusion due to postoperative anemia were the most common complications. Blood transfusion was necessary in 24 patients (37.5%).
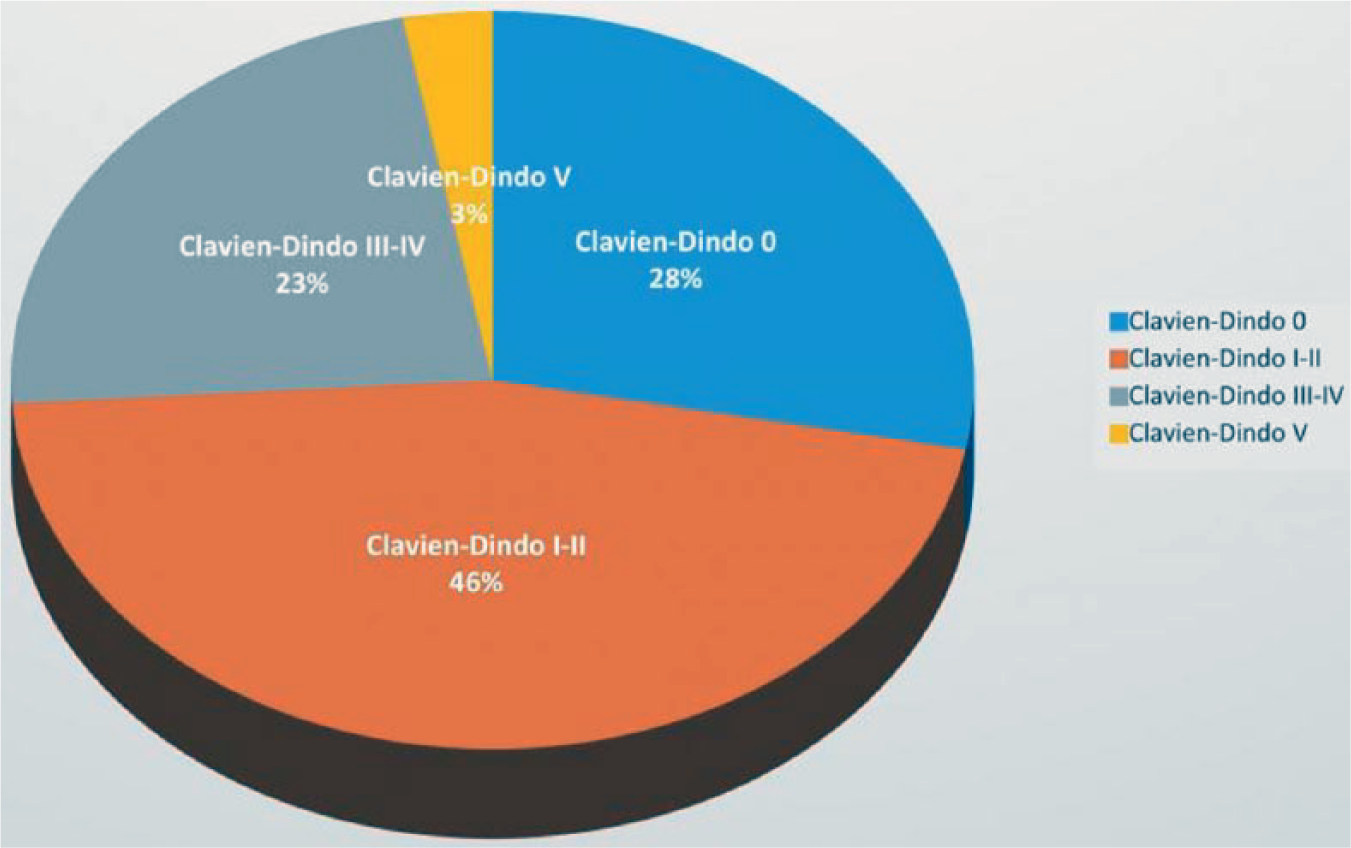
Percentage of postoperative complications.
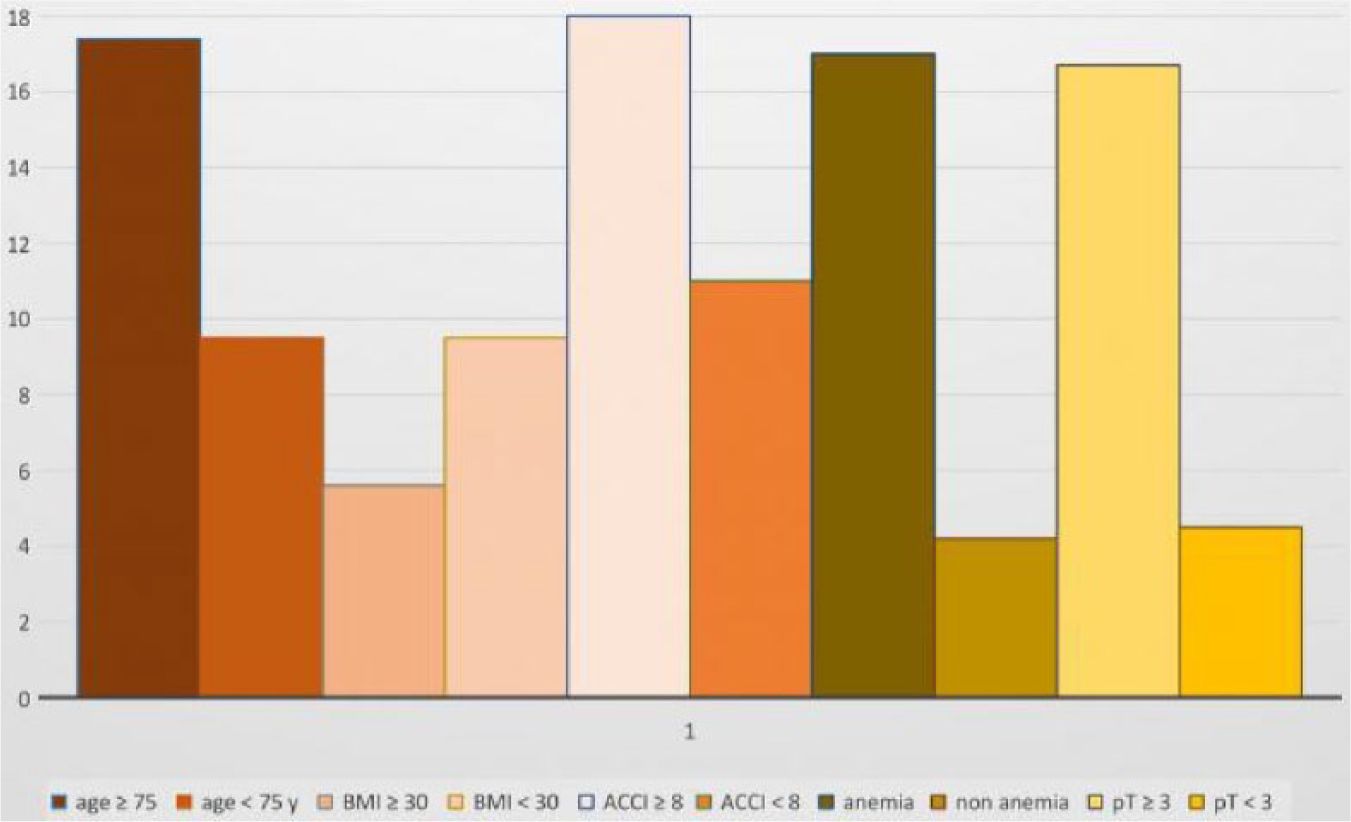
The percentage and correlations between postoperative total and severe complications and presurgery patient characteristics are shown in Figure 2 and Tables 2 and 3, while the percentage and correlations between 90-day mortality and presurgery patient characteristics are shown in Figure 3 and Table 4.
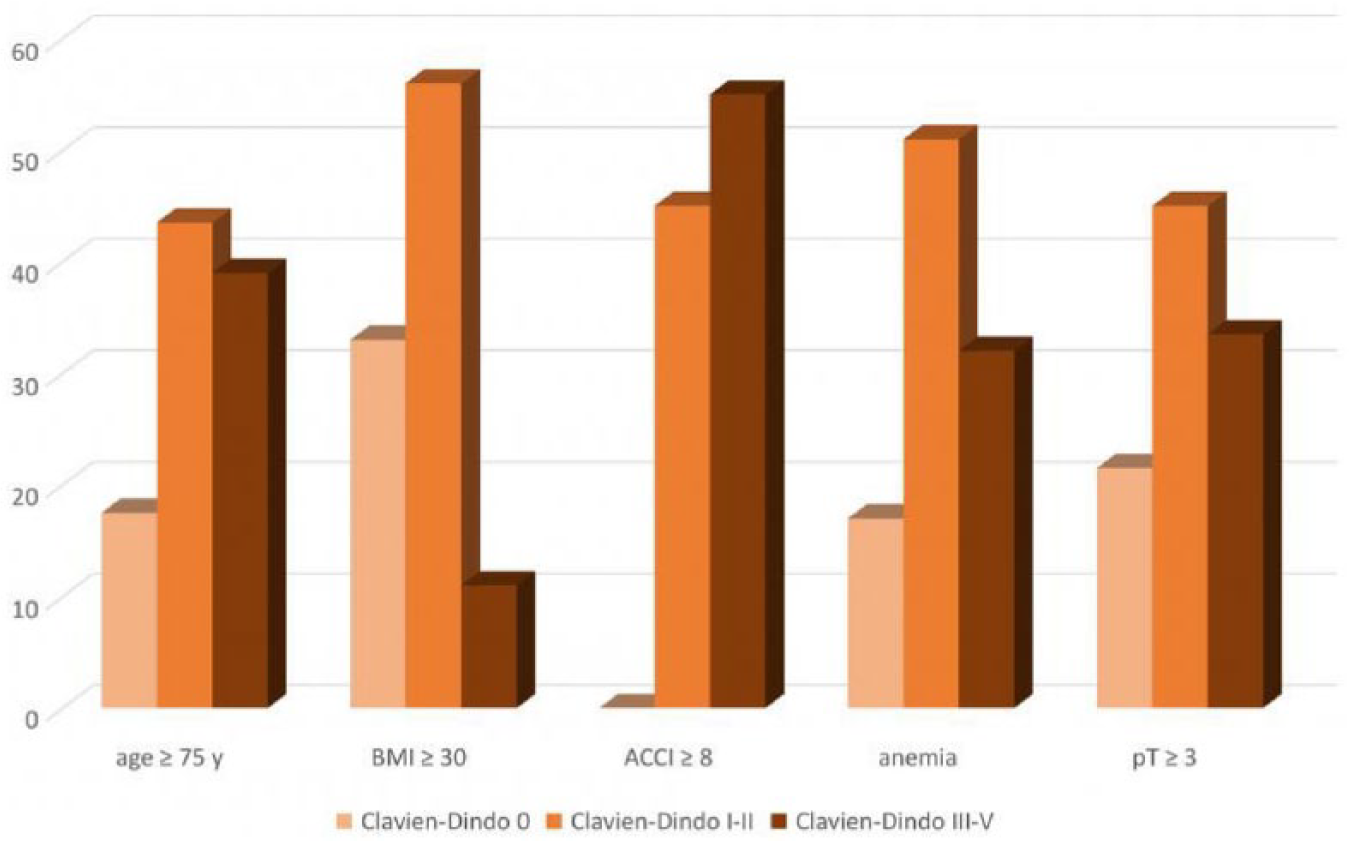
Percentage of complications as a function of presurgery state.
Correlations between postoperative total complications and presurgery state.
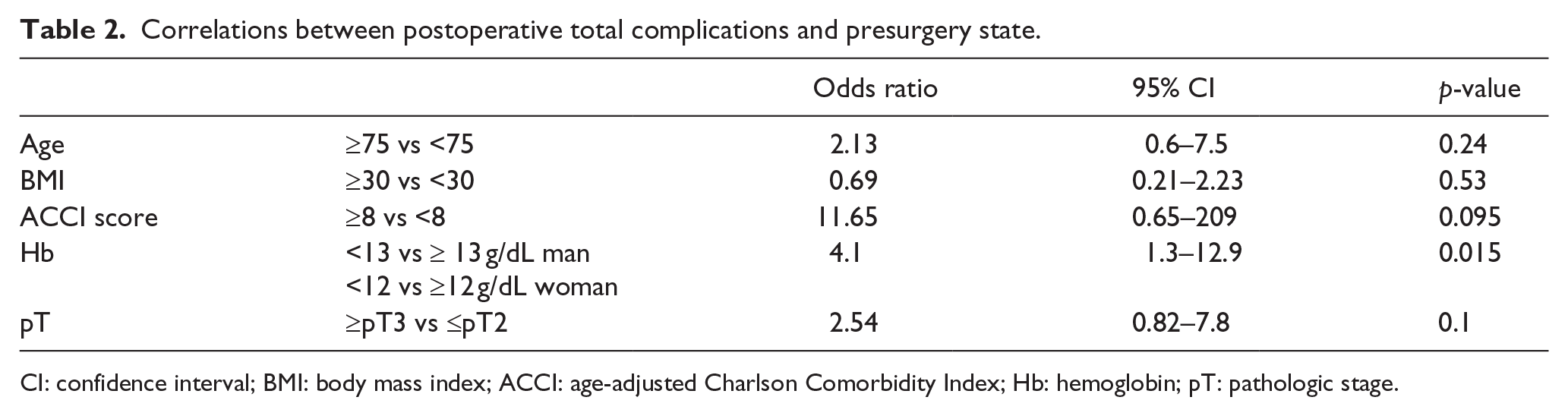
CI: confidence interval; BMI: body mass index; ACCI: age-adjusted Charlson Comorbidity Index; Hb: hemoglobin; pT: pathologic stage.
Correlations between postoperative severe complications (grades III–V) and presurgery state.
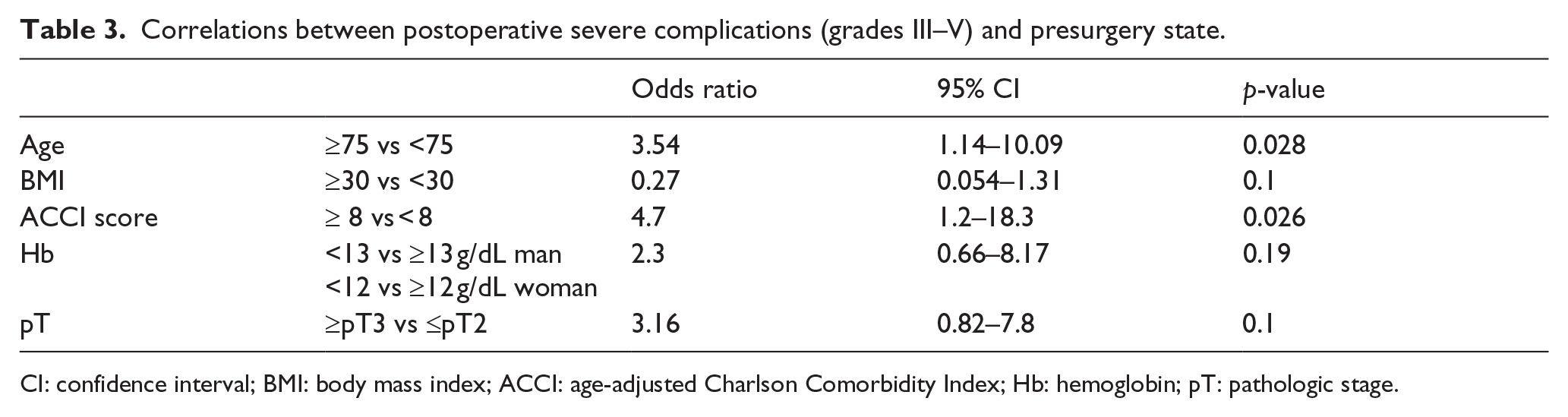
CI: confidence interval; BMI: body mass index; ACCI: age-adjusted Charlson Comorbidity Index; Hb: hemoglobin; pT: pathologic stage.
Ninety-day mortality as a function of presurgery state.
Correlations between 90-day mortality and presurgery state.
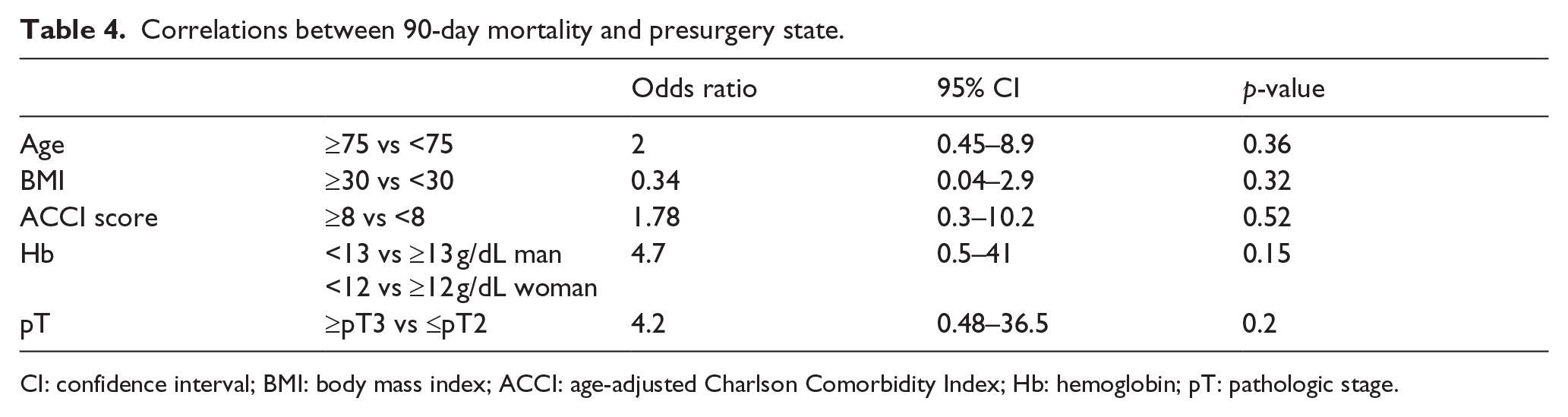
CI: confidence interval; BMI: body mass index; ACCI: age-adjusted Charlson Comorbidity Index; Hb: hemoglobin; pT: pathologic stage.
In our experience, anemic preoperative status is a statistically significant predictor of the onset of complications in general (odds ratio = 4.1 with confidence interval (CI) = 1.3–12.9 and p = 0.015).
In our experience, the age ≥75 and ACCI ≥8 are statistically significant predictors of the onset of severe complications (grades III–V; odds ratio = 3.54 with CI = 1.14–10.09 and p = 0.028 and odds ratio = 4.7 with CI = 1.2–18.3 and p = 0.026).
The total 90-day mortality rate after the surgical intervention was 12.3%. In our experience, age, body mass index (BMI), ACCI, anemic status, and tumor extension are not statistically significant predictors of 90-day mortality from RC.
Discussion
RC is an extremely challenging surgical procedure and it is certainly burdened by considerable morbidity and mortality in the premature or late postoperative period. Patients with RC treatment indications are often complex patients with multiple comorbidities that may make the surgical approach uncertain. However, the need for surgical excision of tumor mass is necessary when the neoplasia has not yet given metastasis at a distance, but it is not conservatively treatable to improve the patient’s prognosis.4,5 In this clinical picture, it is therefore important to understand the outcomes of RC surgery in terms of complications and mortality in high-risk patients to ultimately assess the relationship between risk and benefit for the patient. Our study has the advantage of presenting a standardized assessment of patient comorbidity (via ACCI score) and postoperative complications (by Clavien–Dindo classification) and a recent observation period (2011–2016). The number of patients analyzed is, however, limited to 65 people given the monocentric nature of the study and the classification criteria by which patients are considered to be “high risk” are arbitrary. As this work is a retrospective study, it presents the disadvantage of having a risk of greater statistical bias. The choice we have made to evaluate complications in the limited period of postoperative hospitalization and not 90 days is related to the fact that in the latter case, data collection would be fragmentary. Our choice was to analyze the outcomes of surgery according to each of the “disadvantaged conditions” that led to classifying the patient as “high-risk” patient independently from the others. Thus, the approach is to a single-variant analysis of the data obtained.
There are numerous studies in the literature that investigate the incidence, nature, severity, and predictive factors of postoperative complications in RC as well as 90-day mortality of surgical interventions; these studies are characterized by often quite different results among them, probably due to the remarkable heterogeneity in the clinical and socioeconomic characteristics of patients. Moreover, different classifications of postoperative complications have been used frequently in the various studies, so that it is often difficult to compare the different results among them. Postoperative complications in our case have arisen in 72% of patients, about half of which were mild and moderate complications (grades I–II) and, therefore, characterized by easy clinical management. Total 90-day mortality after surgery instead was 12.3%. These results deviate from those of some major RC studies, such as those of Shabsigh et al., 6 who conducted a study over 1142 patients undergoing RC that had a rate of complications that arose during hospitalization to about 42%, while in the study conducted by Schiavina et al., 7 they reported a 90-day complication rate of 51.7% on a total of 404 patients operated (34.4% grades I–II and 17.3% grades III–V according to Clavien–Dindo) with a total 3-month mortality of 4.5%. Furthermore, in a recent review by Krajewski et al., 8 postoperative complications have been reported in 30% of patients. The closest results to ours are those obtained from Djaladat et al., 9 where the rate of 90-day complications from the RC in 169 patients was 78.1% (minor complications in 53.9% of patients at greater than 24.3%). In the study conducted by Hautmann et al., 10 mortality was recorded at 30 and 90 days from the intervention by 3.2% and 5.2%, respectively. However, in these studies, a standardized system such as that of Clavien–Dindo has not been used to report complications, and the population of patients studied did not focus exclusively on “high-risk” patients, and therefore probably were more predisposed to a worse prognosis. Among the factors that are most considered in the stratification of the risk of surgery are certainly the age of the patient and his comorbidities.
In our case, the age and ACCI scores ≥8 proved to be statistically significant prediction factors for the onset of severe post-RC complications. A work that investigated postoperative complications and 90-day mortality following RC in elderly patients (>75 years) is that carried out by Berger et al., 11 who report a global rate of complications during hospitalization of 58.6% (32% grades I–II and 26.6% grades III–V according to Clavien–Dindo) and a 90-day overall mortality of 9%. Our mortality outcomes are in line with those obtained by Schiffmann et al. 12 in a study in which mortality was investigated in 5207 patients over 65 years undergoing RC, which was overall 10.6% 90 days after surgery. The study shows that mortality increases considerably with age (reaching 14.8% in patients over 80 years of age) and patient comorbidity (90-day mortality in patients with a comorbidity index of Charlson more than 3 arrives at 15.9%). The study concludes that the recorded mortality is significantly higher than previously reported in other work and that advanced age, a high consumer price index (CPI), low socioeconomic status, and celibacy/spinsterhood are independent predictors of 90-day mortality from intervention. In contrast, the study of Clark et al., 13 in 1054 patients undergoing RC stratified in four age groups, shows that the age of the patient does not affect the global rate of complications that is overlapping in the different groups.
In our study, the condition of obesity (BMI >30) did not prove to be a predictive factor for postoperative complications nor 90-day mortality from RC intervention, contrary to Berger et al., 11 who demonstrate a statistically significant correlation with the onset of postoperative complications and to Dabi et al., 14 who in their work state that obesity is an independent predictor of specific tumor mortality and recurrence of disease in patients with bladder carcinoma treated with RC. A total of 63% of the patients analyzed in our case had a preoperative anemia condition that proved to be a predictor of postoperative complications, but not of 90-day mortality. Recently, there has been increasing interest in the role of anemic status as a prognostic factor in surgical outcomes. Xia and Guzzo 15 carried out a meta-analysis on 17 scientific papers to assess the impact of anemia on the outcomes of RC; this work demonstrates that preoperative anemic status in RC is statistically associated with a worse prognosis than non-anemic patients undergoing the same surgery as regards overall mortality and specific tumor and recurrence of the disease. However, this work does not investigate correlation with the onset of postoperative complications. Studies by Stain et al. 16 and Madersbacher et al. 17 are important works in which there is an important correlation between tumor extension (pT parameter) and prognosis after RC. In our case there was not the same correlation statistics.
Conclusion
In light of our experience, it can be argued that the use of a standardized postoperative complication classification system is necessary to avoid excessive variability in their recording between one study and another, and thus it allows better comparison between works on the same topic carried out by different research groups. The incidence of immediate postoperative complications and 90-day mortality in RC in high-risk patients remains significant and moderately higher than that of the total population of patients undergoing this surgery. Although the results we obtained are superimposable to those of studies in the literature on comparable populations for preoperative conditions, it should be emphasized, however, that much of the complications are mild to moderate, and therefore easily managed clinically in a conservative manner and with good prognosis.
Some of the preoperative parameters considered and classified as high-risk criteria have been shown to predict the outcomes of the intervention with regard to the onset of complications but not to the 90-day mortality.
Although it is certainly necessary to work with a larger patient population than the one we have studied, it is advisable that RC will also be performed in patients who are considered to be at high risk as the rate of negative outcomes does not differ much from the general reported in the literature, and therefore the relationship between the risk and the benefit of surgical intervention remains in favor of the second. Therefore, it is necessary to elaborate a RC stratification system suitable for this specific category of patients in the perspective of a personalized medicine and in the field of urological surgery.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.