
Abstract
Objective:
To report the results of a survey supported by the Italian Andrological Association (ASS.A.I.), aimed at documenting sexual disorders in a large population of patients who visited general practitioners for general health problems.
Methods:
Between April and October 2016, 15,000 questionnaires were distributed to general practitioners throughout Italy and made available to all the people who visited the doctor’s offices. The data were collated separately for age ranges, 15–30, 31–50 and 51–65 years, respectively.
Results:
A final sample of 5441 questionnaires was evaluable (4000 men and 1441 women). Sexual disorders were reported by 1795 out of 5441 (33.0%) patients. Among the male population, phimosis, varicocele, prostate and testicular disorders were the most common conditions interfering with sexuality, being reported by 42.0%, 37.0%, 39.0% and 31.0% of the sample, respectively. Furthermore, erectile dysfunction, sexually transmitted diseases, infertility, premature ejaculation and penile curvature were reported by 27.7%, 27.0%, 17.0%, 14.4% and 7.8% of the male sample, respectively. Among the female population, low sexual satisfaction was the more common complaint, reported by 65.0% of the sample. Sexually transmitted diseases, low libido, dyspareunia, infertility and arousal disorder were reported by 32.0%, 29.0%, 24.0%, 24.0% and 19.7% of the female sample, respectively.
Conclusion:
Our data show sexual disorders among 33.0% of people visiting doctors’ offices. The majority of these sexual disorders increased with age among both male and female subjects. Despite the limitations of our study, we consider that these data confirm the importance of sexual function evaluation during a physician’s daily clinical practice.
Keywords
Introduction
The World Health Organization (WHO) defines sexual health as a continuum of physical, psychological and socio-cultural well-being associated with sexuality. 1 In this setting, sexual disorders produce feelings of distress that have a profound impact on the individual’s perception of the sexual quality of life. 2 Studies on the prevalence of sexual disorders typically address specific categories of sexual dysfunction and patient disease groups, for example, sexual dysfunction associated with diabetes, cardiovascular disease, obesity, cancer, cancer chemotherapy or other medications and depression. However, sexual dysfunction can arise from a wide range of organic or psychosocial causes, and information regarding the sexual health of the general population has tended to be overlooked. 3 Furthermore, family physicians are often reluctant to initiate discussions about sexual concerns with their patients. 4
To help address the limited data on the effects of sexual disorders in the general population, the Italian Andrological Association (ASS.A.I.) undertook a survey which aimed to estimate the incidence and type of sexual disorders in a large population of patients of different ages who visited the offices of general practitioners and family doctors for general health problems. The aim of this article is to report the results of this survey.
Methods
Between April and October 2016, a total of 15,000 questionnaires were distributed to general practitioners throughout all Italian regions by the ASS.A.I. Andrologists. The questionnaire forms were anonymous and made available to all the people who visited the doctors’ offices, including accompanying persons.
The survey consisted of two parts. The first part recorded demographical data, such as age and sex, along with the patient’s medical history. Specific inquiries about risk factors for sexual disorders, such as a chronic disease, the presence of an overweight condition and regular consumption or abuse of alcohol, nicotine and other substances. As data were reported by the patients, they were descriptive rather than quantitative. The second part comprised a questionnaire consisting of 12 questions focusing on male and female sexual disorders.
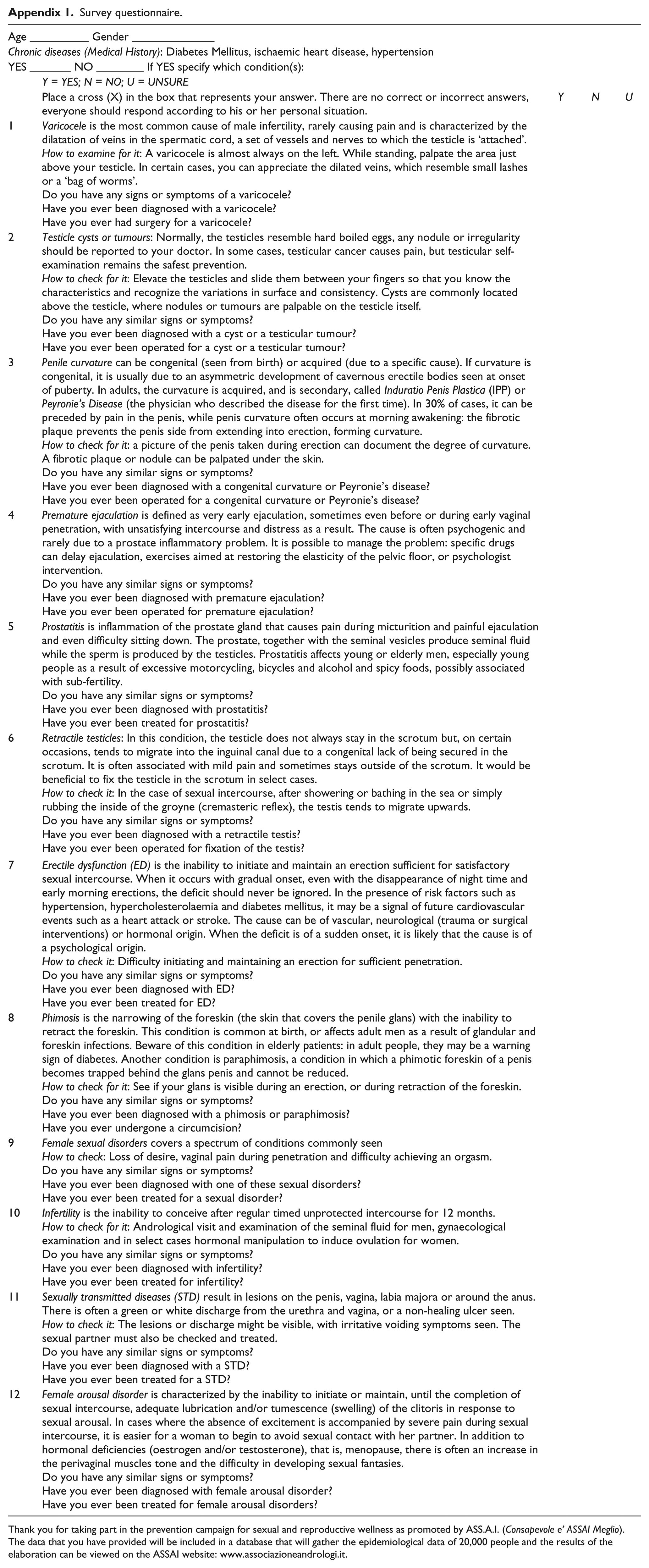
Sexual disorders considered in the survey were varicocele, tumours or cysts of the testicles, penile curvature, premature ejaculation, prostatitis, retractile testicles, erectile dysfunction, phimosis, female sexual disorders (loss of desire, vaginal pain during penetration and difficulty achieving an orgasm), infertility, sexually transmitted diseases and female arousal disorder.
If participants reported had been diagnosed with or had received treatment for one of the sexual disorders included in the survey, they were invited to complete the questionnaire. A copy of the questionnaire is included in Appendix 1. The data were collated separately for three different age ranges, 15–30, 31–50 and 51–65 years, respectively. As no statistical analysis was conducted, the results are descriptive.
As participation was optional and all patients eligible for inclusion in the survey were attending the offices of their general practitioner or family doctors for general health problems, only data of a type available to the physician during a routine patient consultation were collected. Patient consent to participate was implicit in the completion and return of a questionnaire.
Results
Overall, of the 15,000 questionnaires distributed, questionnaires were filled in and returned by, and accompanying demographical data collected for, a total of 6190 participants, with a response rate of 41.2%. A total of 749 questionnaires were considered incomplete and were excluded from the evaluation, leaving a final sample of 5441 (36.2%) questionnaires evaluable for results; 4000 (26.6%) from male and 1441 (9.6%) from female patients, respectively.
Risk factors
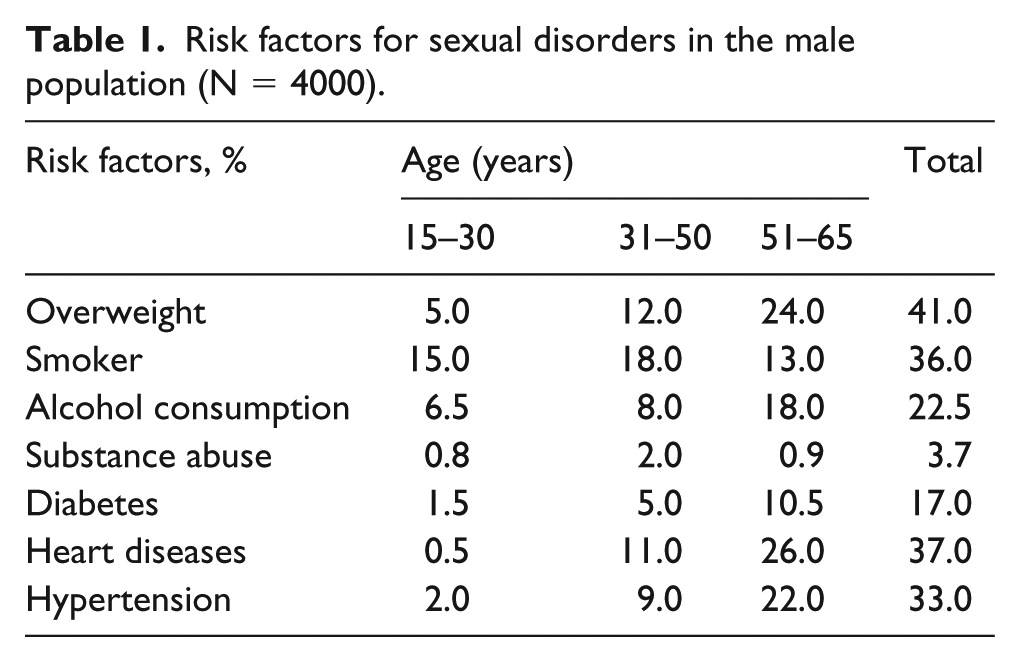
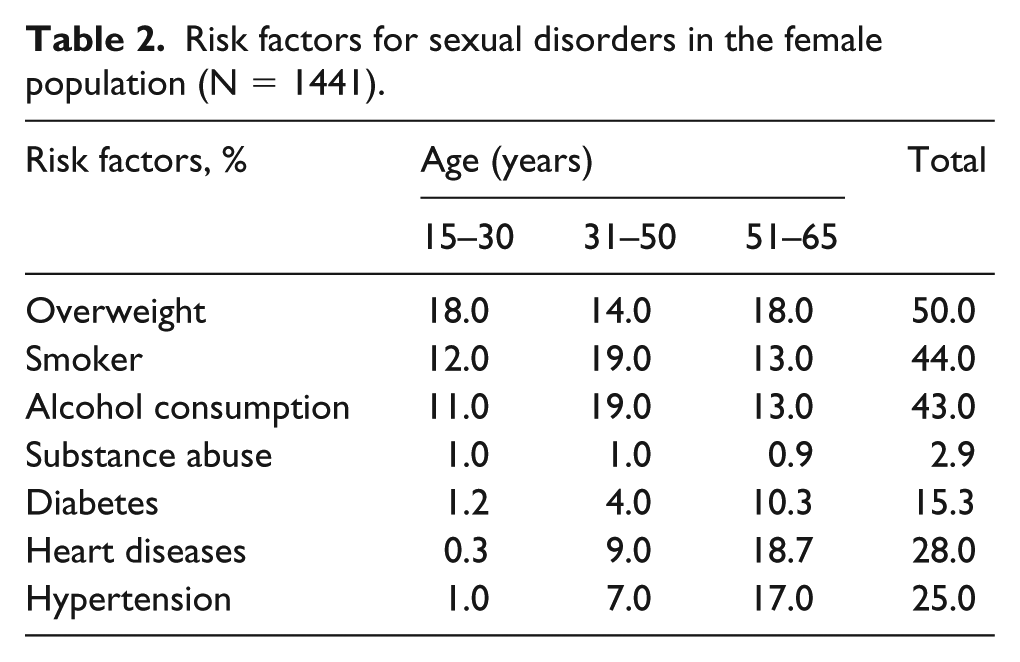
The results regarding risk factors for sexual disorders in male and female populations are summarized in Tables 1 and 2, respectively. Chronic diseases reported included diabetes mellitus, ischaemic heart disease and hypertension. Overweight status, smoking habit, alcohol consumption, heart diseases and hypertension were the most widely reported risk factors, with some variations for age and gender. Although the results are descriptive as no statistical analysis was performed, the rates reported for overweight status and alcohol consumption were slightly higher in younger women as compared to younger men, while the same parameters were slightly higher among older men compared to women.
Risk factors for sexual disorders in the male population (N = 4000).
Risk factors for sexual disorders in the female population (N = 1441).
Sexual disorders
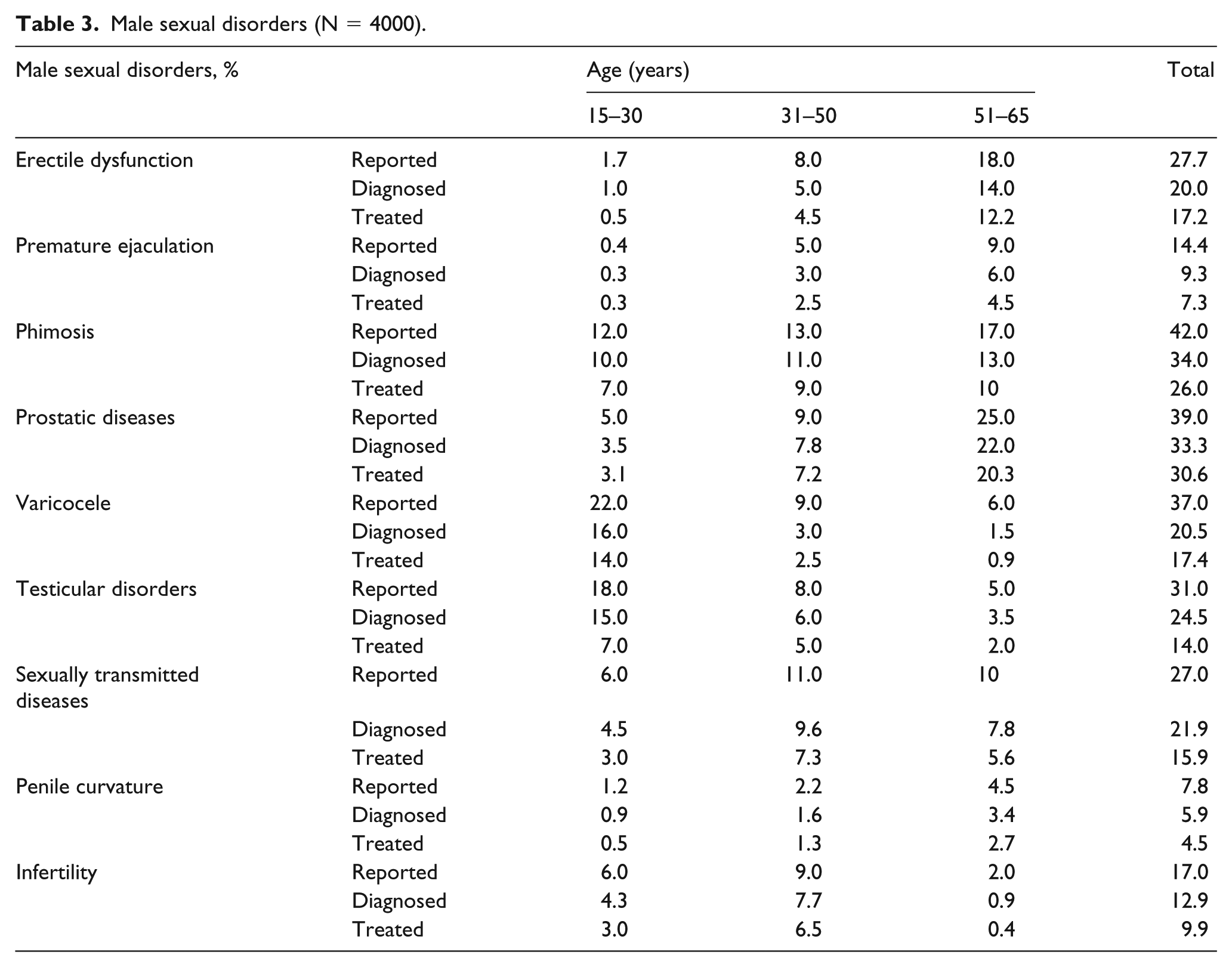
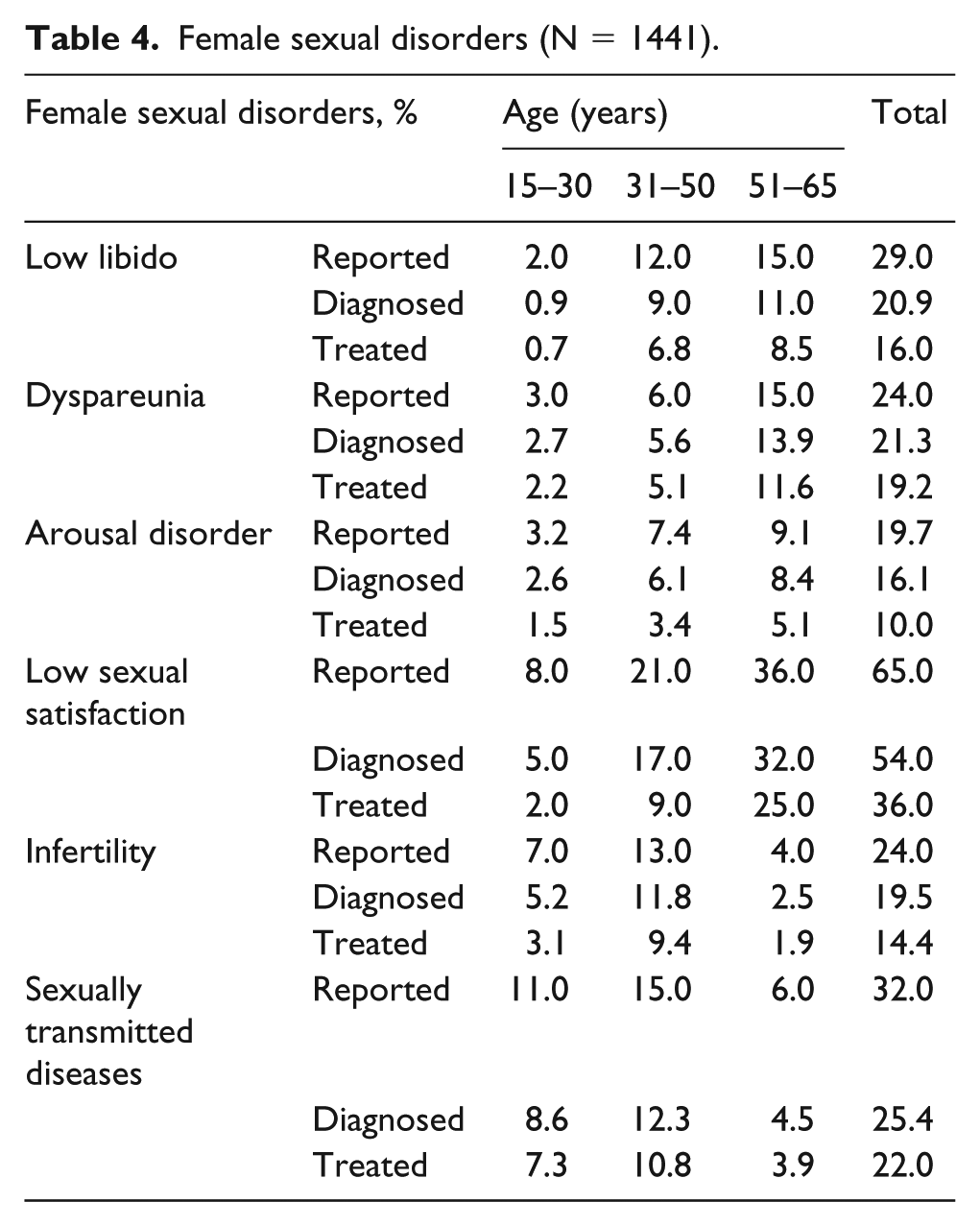
Overall, sexual disorders were reported by 1795 out of 5441 (33.0%) patients. The percentage of reported, diagnosed and treated sexual disorders among the different age categories for male and female samples is reported in Tables 3 and 4, respectively.
Male sexual disorders (N = 4000).
Female sexual disorders (N = 1441).
Phimosis, varicocele, prostate and testicular disorders were the most common conditions interfering with male sexuality, being reported by 42.0%, 37.0%, 39.0% and 31.0% of the male sample, respectively. In addition, erectile dysfunction, sexually transmitted diseases, infertility, premature ejaculation and penile curvature were reported by 27.7%, 27.0%, 17.0%, 14.4% and 7.8% of the male sample across all the age ranges, respectively.
Among the female population, low sexual satisfaction was the more common complaint, which increased with age and was reported overall by 65.0% of the sample. Low libido, dyspareunia and arousal disorder showed a parallel distribution, being reported by 29.0%, 24.0% and 19.7%, respectively. Infertility and sexually transmitted diseases were reported by 24.0% and 32.0% of the female population, respectively.
Discussion
The results of our survey provide a ‘snapshot’ of the range and incidence of sexual disorders among a representative population of patients visiting the offices of general practitioners and family doctors for general health problems.
Our preliminary evaluation of the risk factors for sexual disorders likely to be encountered in general medical practice was mainly reflected in the survey results, which showed significant rates of overweight status, smoking habit, alcohol consumption, heart diseases, diabetes and hypertension among participants. Despite some differences between the two groups, the distribution of these risk factors among our sample population was essentially similar.
Sexual disorders were documented in 33.0% of our sample population. That is, the data showed that one out of three persons who visited the doctor’s office reported being affected by some type of sexual disorder. This is similar to data reported in two other papers available in the literature, which showed sexual difficulties in 20%–40% of adult patients,3,5 confirming the importance of considering sexual disorders in the context of primary health care.
Concerning male sexual disorders, we found an expected progressive increase in erectile dysfunction with age among the three different age groups, although the percentage of erectile dysfunction in the third age category was lower than those reported in the literature, especially when we considered diagnosed and treated patients (14.0% and 12.2%, respectively).6,7 However, this can be explained by the differences in methodology, age ranges, and the socioeconomic and cultural status of the populations studied. A similar progressive increase in phimosis and prostatic disorders was also described, probably due to the development of chronic diseases such as diabetes and benign prostatic hyperplasia with increasing age.8,9
There was a mild progressive increase in the sexually transmitted diseases from adolescence to adulthood, supporting the main development of these disorders during this period of life. 10 Surprisingly, although the rate of premature ejaculation increased through the different age categories, it was never higher than 14.4% and 9.3% of reported and diagnosed patients, respectively. This is in contrast with the majority of the literature, which has reported premature ejaculation rates between 20% and 40%. 11 However, when, as with our study, specific diagnostic tools were not used, other series have reported data similar to our results.12,13 A progressive increase in penile curvature was noted across the age categories reflecting the age-related development of Peyronie’s disease. 14 In contrast, we found a comprehensive progressive decrease in the varicocele and testicular disorders, which generally tend to recur less in adulthood. 15
Concerning female sexual disorders, we found a progressive increase in low libido, dyspareunia, arousal disorder and low sexual satisfaction throughout the three different age categories. In particular, there was a strong decrease in sexual satisfaction in women over 50 years old, 36.0% of whom reported low sexual satisfaction. Similar or even higher incidences of low sexual desire and sexually related female distress which generally emerged early and increased with age with a peak at midlife have been reported.16–20 The decrease in the rate of sexually transmitted diseases in the last age category tended to confirm these aspects. Higher rates of infertility were more commonly reported in the first two age categories in both male and female groups.
This study has a number of limitations. First, our data are derived from analysis of a survey and diagnoses were not confirmed by subsequent physical examination or compilation of disease-specific questionnaires. Furthermore, the design of our study did not allow for statistical analysis of the data. However, our aim was to provide a snapshot of the extent of reported sexual disorders in patients during routine visits to their doctor; it was not our aim to perform a prevalence study. In contrast, the main strength of this article is the large sample size represented by male and female subjects from different age categories throughout all regions of Italy.
Conclusion
The results of our survey suggest sexual problems are common in patients making routine visits to their doctor, with a third of participants in our survey sample reporting a sexual disorder. The majority of these sexual disorders increased with age across the different age categories of both male and female subjects. Despite the limitations of our study, we consider that these data confirm the importance of physicians making discussion and evaluation of the sexual health of their patients a routine part of daily clinical practice.
Footnotes
Appendix
Survey questionnaire.
| Age __________ Gender ______________ | ||||
| Chronic diseases (Medical History): Diabetes Mellitus, ischaemic heart disease, hypertension | ||||
| YES _______ NO ________ If YES specify which condition(s): | ||||
| Y = YES; N = NO; U = UNSURE | ||||
| Place a cross (X) in the box that represents your answer. There are no correct or incorrect answers, everyone should respond according to his or her personal situation. | Y | N | U | |
| 1 | Varicocele is the most common cause of male infertility, rarely causing pain and is characterized by the dilatation of veins in the spermatic cord, a set of vessels and nerves to which the testicle is ‘attached’. |
|||
| 2 | Testicle cysts or tumours: Normally, the testicles resemble hard boiled eggs, any nodule or irregularity should be reported to your doctor. In some cases, testicular cancer causes pain, but testicular self-examination remains the safest prevention. |
|||
| 3 | Penile curvature can be congenital (seen from birth) or acquired (due to a specific cause). If curvature is congenital, it is usually due to an asymmetric development of cavernous erectile bodies seen at onset of puberty. In adults, the curvature is acquired, and is secondary, called Induratio Penis Plastica (IPP) or Peyronie’s Disease (the physician who described the disease for the first time). In 30% of cases, it can be preceded by pain in the penis, while penis curvature often occurs at morning awakening: the fibrotic plaque prevents the penis side from extending into erection, forming curvature. |
|||
| 4 | Premature ejaculation is defined as very early ejaculation, sometimes even before or during early vaginal penetration, with unsatisfying intercourse and distress as a result. The cause is often psychogenic and rarely due to a prostate inflammatory problem. It is possible to manage the problem: specific drugs can delay ejaculation, exercises aimed at restoring the elasticity of the pelvic floor, or psychologist intervention. |
|||
| 5 | Prostatitis is inflammation of the prostate gland that causes pain during micturition and painful ejaculation and even difficulty sitting down. The prostate, together with the seminal vesicles produce seminal fluid while the sperm is produced by the testicles. Prostatitis affects young or elderly men, especially young people as a result of excessive motorcycling, bicycles and alcohol and spicy foods, possibly associated with sub-fertility. |
|||
| 6 | Retractile testicles: In this condition, the testicle does not always stay in the scrotum but, on certain occasions, tends to migrate into the inguinal canal due to a congenital lack of being secured in the scrotum. It is often associated with mild pain and sometimes stays outside of the scrotum. It would be beneficial to fix the testicle in the scrotum in select cases. |
|||
| 7 | Erectile dysfunction (ED) is the inability to initiate and maintain an erection sufficient for satisfactory sexual intercourse. When it occurs with gradual onset, even with the disappearance of night time and early morning erections, the deficit should never be ignored. In the presence of risk factors such as hypertension, hypercholesterolaemia and diabetes mellitus, it may be a signal of future cardiovascular events such as a heart attack or stroke. The cause can be of vascular, neurological (trauma or surgical interventions) or hormonal origin. When the deficit is of a sudden onset, it is likely that the cause is of a psychological origin. |
|||
| 8 | Phimosis is the narrowing of the foreskin (the skin that covers the penile glans) with the inability to retract the foreskin. This condition is common at birth, or affects adult men as a result of glandular and foreskin infections. Beware of this condition in elderly patients: in adult people, they may be a warning sign of diabetes. Another condition is paraphimosis, a condition in which a phimotic foreskin of a penis becomes trapped behind the glans penis and cannot be reduced. |
|||
| 9 | Female sexual disorders covers a spectrum of conditions commonly seen |
|||
| 10 | Infertility is the inability to conceive after regular timed unprotected intercourse for 12 months. |
|||
| 11 | Sexually transmitted diseases (STD) result in lesions on the penis, vagina, labia majora or around the anus. There is often a green or white discharge from the urethra and vagina, or a non-healing ulcer seen. |
|||
| 12 | Female arousal disorder is characterized by the inability to initiate or maintain, until the completion of sexual intercourse, adequate lubrication and/or tumescence (swelling) of the clitoris in response to sexual arousal. In cases where the absence of excitement is accompanied by severe pain during sexual intercourse, it is easier for a woman to begin to avoid sexual contact with her partner. In addition to hormonal deficiencies (oestrogen and/or testosterone), that is, menopause, there is often an increase in the perivaginal muscles tone and the difficulty in developing sexual fantasies. |
|||
Thank you for taking part in the prevention campaign for sexual and reproductive wellness as promoted by ASS.A.I. (Consapevole e’ ASSAI Meglio).
The data that you have provided will be included in a database that will gather the epidemiological data of 20,000 people and the results of the elaboration can be viewed on the ASSAI website: www.associazioneandrologi.it.
Acknowledgements
The authors thank Ray Hill and Carmen Innes, two independent medical writers, who provided English language editing and medical writing support prior to submission, on behalf of Springer Healthcare Communications. This assistance was funded by IBSA Institut Biochimique S.A. The authors thank the following colleagues for their important contribution: Francesco Gattuccio (Palermo), Maurizio Bossi (Milan), Lamberto Coppola (Rome), Raffaella Longo (Rome), Marina Baldi (Rome), Anna Carderi (Rome), Guglielmo Mantica (Genoa), Andrea Pacchetti (Genoa), Nicolò Testino (Genoa), Alberto Olivero (Genoa), Dotta Federico (Genoa), Gaetano Ninotta (Savona), Claudio Giberti (Savona), Andrea Ortensi (Rome), Ilaria Ortensi (Rome), Benincasa Maria Luisa (Palermo), Gagliando Ambra (Palermo), Orlando Gaetano (Palermo), D’Anna Elena (Palermo), Francesca Gattuccio (Palermo), Francesco Losavio (Brindisi), Marcello Falconieri (Brindisi), Claudio Manna (Rome), Marco Di Pierro (Genoa), Irene Pontedell’oglio (Milan), Giacomo Tuo (Genoa), Canepa Pierandrea (Genoa), Paolo Codispoti (Rome), Gianfranco Piccolelli (Rome), Claudio Prono (Rome), Raffaele Oteri (Rome), Alessandro Di Lorenzo (Rome), Filippo Di Pasquale (Rome), Domenico Carpita (Rome), Marco Maria Giardina (Rome), Antonella Simonato (Rome), Francesco Guidotti (Rome), Anna Lisa Nicosia (Rome), Patrizia Lentini (Rome), Francesco Raggi, (Terni), Pierfrancesco Prusciano (Biologist from Taranto), Paolo Rossi (Pisa), Giuseppe Gallo (Savona), Fulvio Testa (Savona), Fabio Caratti (Savona), Domenico Canini (Celle Ligure), and Livio Operto (Finale Ligure).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.