
Abstract
Objective:
To evaluate preoperative scoring systems and operative management and their relation to complications in patients older than 75 years undergoing cystectomy at two academic institutions.
Methods:
In total, 212 patients aged 75–95 years with muscle invasive bladder cancer underwent cystectomy at the University of Utah and Central Hospital of Bolzano, Italy. The rates of Grade 3 Clavien-Dindo complications and above in radical cystectomy patients (n = 199) were compared using Eastern Cooperative Oncology Group Scores and American Society of Anesthesiologists Physical Status Classification. The rates of Grade 3 Clavien-Dindo complications and above were also compared by urinary diversion type. Logistic regression was used to control for source institution.
Results:
In total, 199 cases were included in the primary analysis. Neither of the preoperative scoring systems were predictive for identification of radical cystectomy patients with ⩾Grade 3 Clavien-Dindo complications. In secondary analysis (n = 212, including partial cystectomy), none of the urinary diversion types associated with radical cystectomy had a significantly different rate of complications. However, partial cystectomy (n = 13) had a significantly lower rate of complications.
Conclusion:
Complication rates among elderly patients undergoing cystectomy for muscle invasive bladder cancer were very high. For patients who are approved for surgery after the history and physical exam, none of our objective metrics adequately predicted operative risk. A unique diversion procedure described by the Bolzano group, uretero-ureterocutaneostomy, had equivalent complication rates to the more common diversion procedures. It also appears based on outcomes in this cohort that partial cystectomy is a particularly favorable option within the elderly population in terms of perioperative morbidity.
Introduction
Currently, radical cystectomy is typically the recommended treatment for muscle invasive bladder cancer due to its oncologic efficacy.1–4 Unfortunately, there is significant morbidity and mortality associated with radical cystectomy for muscle invasive bladder cancer in patients older than 75 years.5,6 Overall, complications in this age group range from 24% to 60.9% depending on the series and technique used, with the most commonly reported complications being ileus, pyelonephritis, and urinary diversion–related complications.7,8
Using the Clavien-Dindo classification to define and grade post-surgical complications, we had previously shown that overall complications rates in elderly patients were 55.4% with a significant fivefold increase in 90-day mortality in those patients greater than 85 years. 5 Therefore, this procedure is not necessarily the treatment selected for muscle invasive bladder cancer in elderly patients, and optimal management is still controversial.9–11 However, without appropriate treatment, only 14% of all patients with muscle-invasive bladder cancer will survive beyond 2 years. 12 Therefore, it is important that we more aptly identify preoperative risk and appropriate management in this specific population.
Previously, Hopkins Fragility Score, American Society of Anesthesiologists (ASA) scores, and elevated Charlson Comorbidity Index (CCI) scores have been described as instruments for predicting post-operative complications.13–15 However, there are few large studies evaluating these instruments in accurately identifying which patients are more likely to develop complications exclusively after cystectomy among elderly patients. By identifying and selecting elderly patients based on preoperative co-morbidities and risk stratifications, it may be possible to predict which older patients are more likely to develop post-operative complications and mortality and avoid a procedure unlikely to have benefit.
In addition to bladder removal, the urinary diversion portion of the procedure has been associated with significant morbidity and complications. 16 Selection of the appropriate diversion procedure requires consideration of the patient preferences, functional status, and disease process. The evidence for each of the different types of diversion procedures is varied. 16 Each of the procedures have risk of infection, strictures, retention, fistulas, and other complications that vary by both the procedure type as well as between individual studies; thus, comparisons between the procedures are difficult to make.17,18
We sought to evaluate methods for predicting complications as well as identifying operative parameters related to complications in patients older than 75 years undergoing cystectomy. Patients were treated at two large academic institutions and preoperative risk scores were measured using Eastern Cooperative Oncology Group (ECOG) Scores and ASA Physical Status Classification System. We hypothesize that higher ECOG and ASA scores will be associated with increased risk of complications following cystectomy in elderly patients and that partial cystectomy will have the lowest rate of complications followed by radical cystectomy with ileal conduit.
Materials and methods
Study population
We identified all patients aged 75–95 years who underwent both radical and partial cystectomy retrospectively at the University of Utah, Huntsman Cancer Hospital, USA, and prospectively at the Central Hospital of Bolzano, Italy, between 2000 and 2012. Table 1 shows the preoperative and operative patient characteristics. Institutional board approval was obtained at each respective center. Demographic information, comorbidities, Clavien-Dindo classification for surgical complications, ASA scores, and ECOG scores were collected for each patient. For patients with multiple complications, only the highest rated complication was considered.
Patient characteristics.
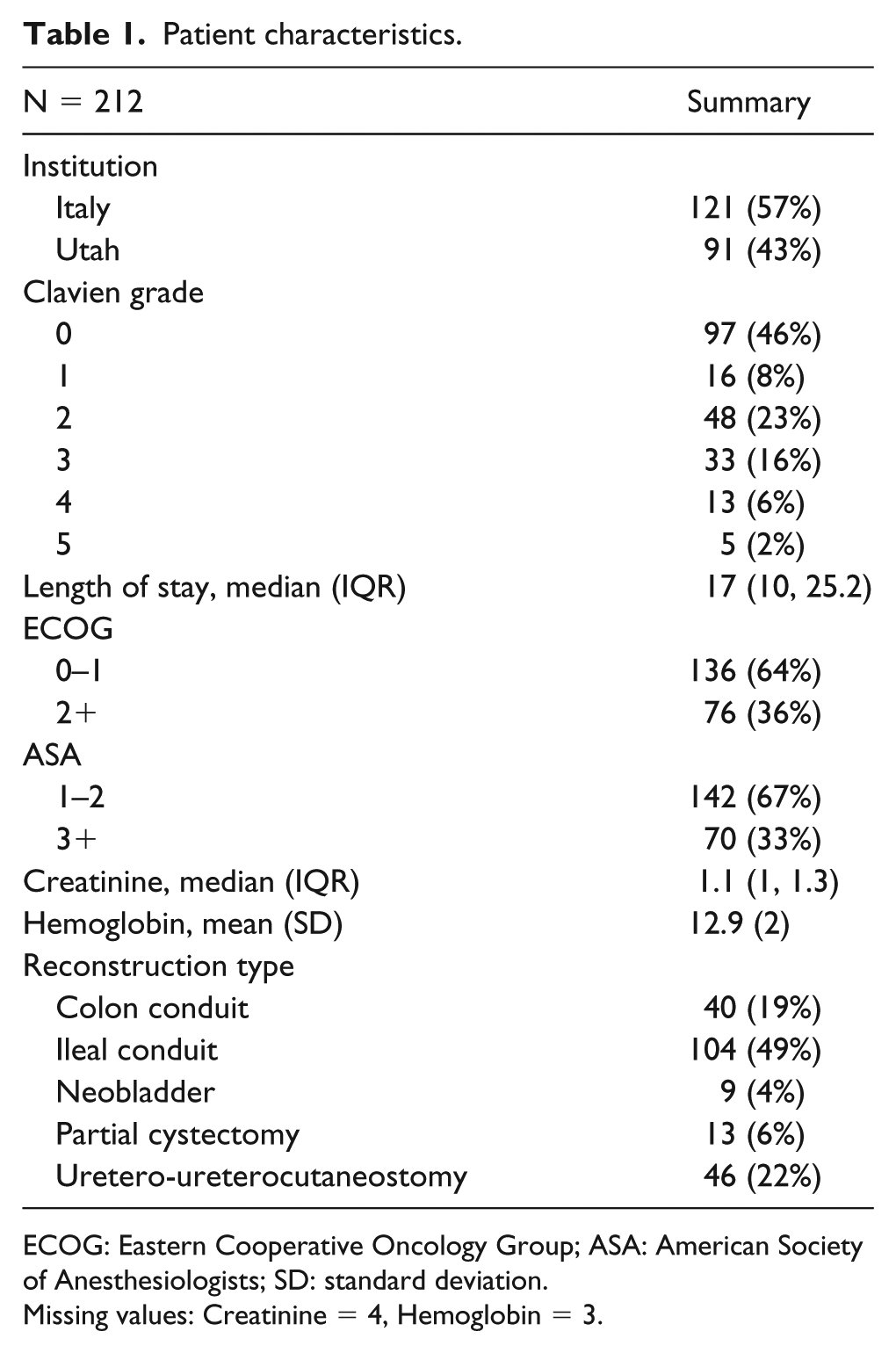
ECOG: Eastern Cooperative Oncology Group; ASA: American Society of Anesthesiologists; SD: standard deviation.
Missing values: Creatinine = 4, Hemoglobin = 3.
Therapeutic intervention
Neoadjuvant and adjuvant chemotherapy rates were low with a total of 19 of 208 patients receiving systemic therapy over this time period (4 of the patient’s chemotherapy status could not be verified). Average preoperative creatinine was 1.28. All cystectomies at both institutions were performed via an open abdominal approach. Urinary diversions were performed as follows: ileal conduit in 105 (49.5%), uretero-ureterocutaneostomy in 46 (21.7%), neobladder in 8 (3.8%), colon conduit in 40 (18.9%), and partial cystectomy in 13 (6.1%).
Outcomes
Primary outcome was assessing the relationship of ⩾Grade 3 Clavien-Dindo complications to high ASA scores (3/4) versus low ASA scores (1/2) and high ECOG scores (2/3) versus low ECOG scores (0/1) as well as rate by urinary diversion type. Secondary outcomes measured included 30-day mortality, 90-day mortality, and 3-year overall survival.
Statistical analysis
Variables were summarized as counts and percentages. Continuous variables were compared using mean (SD). Multinomial variables were evaluated with the chi-square test considered significant at the p values < 0.05. Logistic regression was used to control for source institution and odds ratios (OR) and 95% confidence intervals (CIs) were reported. Statistical significance was evaluated at the 0.05 level, and all tests were two-tailed. Complications were graded using the modified Clavien grading system.19,20 The rate of Grade 3 Clavien-Dindo and higher complications in radical cystectomy were compared with ECOG Scores and ASA Physical Status Classification System. Rate of Grade 3 and higher complications were also compared by diversion type, which included partial cystectomies. Analysis for reconstruction type used Firth’s penalized logistic regression due to perfect separation for the ileal conduit reconstruction. Data analysis was performed with R v. 3.1.1.
Results
A total of 199 patients were included in the primary analysis at the University of Utah (n = 78) and Central Hospital of Bolzano (n = 121) from 2000 to 2012. Table 1 shows the characteristics of both groups. Median patient age was 79 years. Of the 199, 115 (57.8%) patients experienced a complication of any Clavien grade, and 51 out of 199 (24.1%) patients had a Grade 3 Clavien or higher complication. The 30- and 90-day mortalities were 9.9% and 16%, respectively. The 3-year overall survival was 35.8%.
There was no significant difference in complication rates between institutions (p = 0.77). Table 2 shows the relationships between ⩾Grade3 Clavien-Dindo complications and clinical parameters, preoperative physical assessment scores, and diversion type. There was no significant difference in ⩾Grade 3 Clavien-Dindo complications between ASA Classifications of 3–4 versus 1–2 (OR: 1.28; 95% CI: 0.65–2.45). ECOG scores of 2–3 versus 0–1 had similar Grade 3 or greater complications (OR: 1.69; 95% CI: 0.88–3.22). On analysis by urinary diversion type, the rates of complications showed no significant difference when compared to ileal conduit: colon conduit (OR: 0.95; 95% CI: 0.35–2.57), neobladder (OR: 0.90; 95% CI: 0.16–3.62), uretero-ureterocutaneostomy (OR: 0.89; 95% CI: 0.34–2.28), and partial cystectomy (OR: 0.1; 95% CI: <0.01–0.79). Length of stay was also shown to be associated with the presence of complications.
Regression results controlling for institution.
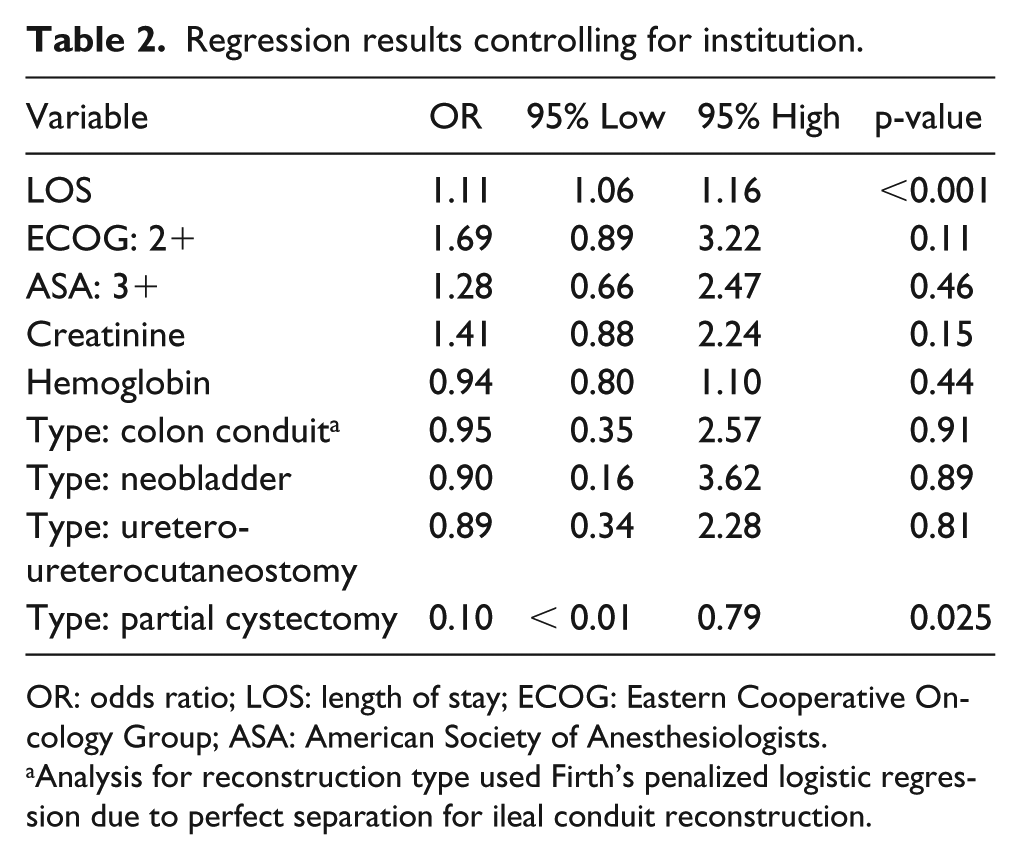
OR: odds ratio; LOS: length of stay; ECOG: Eastern Cooperative Oncology Group; ASA: American Society of Anesthesiologists.
Analysis for reconstruction type used Firth’s penalized logistic regression due to perfect separation for ileal conduit reconstruction.
Discussion
Our results, similar to small studies, suggest that treatment for muscle invasive bladder cancer in the elderly is morbid and appears to be more morbid than treatment in a younger population. Unfortunately, neither prioperative ASA nor ECOG was able to adequately predict complications in this cohort. As expected, partial cystectomy had fewer complications overall and surprisingly had no Grade 3 or greater complications within 90 days of surgery. None of the other types of diversion had significantly different outcomes in terms of ⩾Grade 3 Clavien-Dindo complications.
Given the significant operative morbidity and mortality in the elderly, it is important to continue identifying risk factors for developing complications. Risk stratification in the elderly population is likely to be optimized using both predictive preoperative screening algorithms and appropriate operative decisions. Beyond the surgeons “gestalt” of a given patient’s risk based on history and physical exam, many predictive algorithms have been used to predict complications in younger patients undergoing treatment for muscle invasive bladder cancer. However, there are limited studies identifying risk factors for predicting complications in patients in significantly older patients (over 75 years) undergoing treatment for muscle invasive bladder cancer.
Previously identified preoperative risk factors for complications include a body mass index (BMI) ⩾ 30, increasing age, and an albumin < 3.5 g/dL.21,22 Revenig et al. 14 performed a collaborative study between multiple surgical specialties identifying the Hopkins Frailty Score (HFS) as an excellent predictor of postoperative complications. Markers of frailty include shrinking, weakness, exhaustion, slowed walk, and low activity. While univariate analysis using 30 days of follow-up showed HFS was a statistically significant predictor for post-surgical complications, ASA, CCI, and ECOG scores were not significant predictors of complications in this patient population. More recent studies continue to support frailty as an accurate predictor for postoperative risk. 23 However, for cystectomies being performed at large referral centers, patients may have traveled large distances for their treatment; making it difficult to obtain an accurate assessment of frailty during the immediate preoperative period. Due to these factors, we were unable to properly assess frailty scores for this cohort.
Previous studies in younger patient populations have found that CCI score ⩾ 3 and an ASA score ⩾ 3 were independent predictors of high-grade complications in patients undergoing radical cystectomy.15,24,25 Studies combining sex, BMI, cTN stage, cM+ stage, and age with these comorbidity indices also significantly improved the predictive value for 90-day mortality. 13 By comparison to the HFS, these scores are very easy to obtain and follow, are well validated, and can easily be done on every patient preoperatively. However, in our population, much like the Hopkins study, we did not find a significant difference in Grade 3 complications in patients based on their ECOG and ASA scores. The difference between the younger and elderly cohorts suggests these scores are not adequate predictors for Grade 3 or higher complications in the significantly elderly population.
In addition to preoperative score, the surgical procedures selected for a patient have a large impact on morbidity and complications. Despite having an estimated rate of intravesical recurrence of 38%, patients undergoing partial cystectomy have similar cancer-specific survival rates.26,27 Consistently, elderly patients are treated with partial cystectomy at a higher rate than their younger counterparts likely due to the increased complications associated with this population. 28 In our cohort, patients undergoing partial cystectomy had fewer complications compared to radical cystectomy. Although partial cystectomy likely results in poorer oncologic control, and relatively few tumors are amenable removal by a partial approach, this option should be considered in elderly patients. With these patients having limited life expectancy and increased morbidity associated with surgical therapies, partial cystectomy represents a viable alternative to radical cystectomy for appropriately selected patients.
In elderly patients undergoing radical cystectomy, the selection of an appropriate diversion procedure is also highly important. Each of the procedures have different contraindications and patient preference is an important consideration. The ileal conduit is the least challenging reconstruction technically and requires the least functional capacity on the part of the patient. 16 In comparing the complication rate of ileal conduit to the other types of urinary diversion within our elderly cohort, surpringly there was no difference between the procedures, though some of the diversion types, such as neobladder, may have been underpowered to show a difference.
It is interesting to note the similar outcomes with those patients undergoing uretero-ureterocutaneostomy diversions in this cohort (n = 46). This is a relatively uncommon urinary diversion type in the United States, and its complication rate in relation to the other types of urinary diversion is uncertain. 29 When deciding on performance of a uretero-ureterocutaneostomy, surgeons in our study typically weighed the risk of strictures of the distal cutaneous segment of the ureter with the morbidity of undergoing a bowel resection. In our cohort, uretero-ureterocutaneostomy diversion was typically selected as a minimally invasive option for diversion due to patient’s comorbidities and was often prefered in patients deemed unsuitable candidates for bowel resection.
With consideration for the elevated morbidity and mortality found within these elderly cohorts upon receipt of cystectomy, some of the more frail members of the elderly population presenting with muscle invasive bladder cancer are likely not good surgical candidates and may benefit from bladder sparing modalities. Trimodal therapy with maximal resection, in combination with radiation and chemotherapy, could play a role in this population. 30 While there has not been adequate comparison of radical cystectomy to trimodal therapy (especially in the elderly population), some cohorts utilizing trimodal therapy have been able to obtain acceptable survival and disease-free intervals with the right patient selection. 31 Acceptable outcomes with a modality of potential lower morbidity and mortality would be of particular importance to this elderly population and warrants future study.
To our knowledge, our study is the first time that preoperative ASA and ECOG scores as well as urinary diversion type were used as possible predictors of Clavien-Dindo complications in a large subset of cystectomy patients exclusively older than 74 years. This cohort included all patients who underwent cystectomy at the University of Utah Huntsman Cancer Hospital and at the Central Hospital of Bolzano, Italy between 2000 and 2012. However, this does not take into account the patients who were deemed unfit for surgery or failed to undergo surgery due to other circumstances, though overall very few patients in this age group are offered surgery. The purpose of this study is to provide an overview of surgical outcomes in this population believed to be appropriate surgical candidates despite their advanced age. In accordance with this, we elected to include partial cystectomy in this discussion as patient-specific factors such as disease location, comorbidity, and age likely led to the particular surgical recommendation. None of the preoperative scoring algorithms were predictive of complications. Future studies are necessary to understand if there are better predictors of complications in the elderly population.
Limitations of this study include lack of preoperative stage and albumin as well as previous abdominal surgeries, as this data was unable to be found consistently in the retrospective review of patient charts. In addition, the rate of uretero-ureterocutaneostomy was high in our cohort compared to previous studies. However, our overall complication rate after cystectomy in the elderly was equivalent to previous studies, and it is unlikely that the frequency of this procedure would differentially affect the quality of the preoperative scoring algorithms. Finally, an increase in the sample size may have helped identify more factors predictive of complications.
Conclusion
Complication rates among elderly patients undergoing cystectomy for muscle invasive bladder cancer are very high. Patients undergoing partial cystectomy were significantly less likely to have a ⩾Grade 3 Clavien-Dindo complication. Other preoperative predictors: creatinine, hemoglobin, ASA Classifications, and ECOG scores, as well as diversion type, were not adequate predictors for Grade III or higher complications in this cohort.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.