
Abstract
Objective:
To assess the outcomes of surgical repair of anterior apical prolapse using the 6-strap mesh implant.
Study Design:
The prospective study included 100 patients with genitourinary prolapse. We used advanced 6-strap mesh implant. The results were assessed at 1 (n = 100) and 12 (n = 93) months after surgery. Maximum follow-up was over 4 years. The anatomical outcomes according to the Pelvic Organ Prolapse Quantification system and intraoperative and postoperative complications were assessed. Stage II and higher prolapse was considered to be a recurrence. The quality of life and sexual function were assessed using Pelvic Organ Prolapse Distress Inventory 20, Pelvic Floor Impact Questionnaire 7, and Pelvic Organ Prolapse/Incontinence Sexual Questionnaire 12.
Results:
Median age was 57 years (34–78 years (95% confidence interval)). All patients had stage III cystocele. The anterior vaginal wall descent in all the patients was associated with uterine descent: 37 (37%), stage II; 60 (60%), stage III; in 3 (3%), stage IV. In eight cases, postoperative de novo stress urinary incontinence developed. The quality of life improved in 93 (93%) women as judged by the Pelvic Floor Distress Inventory 20 data and in 87 (87%) women, according to the Pelvic Floor Impact Questionnaire 7 data. The desirable anatomical result (⩽stage I according to the Pelvic Organ Prolapse Quantification system) was achieved in 97 (97%) patients. With the exception of mesh fragment excision due to erosion (grade 3a), all the complications were classified as grade I according to the Clavien–Dindo classification.
Conclusion:
Genitourinary prolapse repair using 6-strap mesh is efficacious and relatively safe. The method demonstrates good anatomical results in relation to both anterior and apical prolapses with relatively short-term complications.
Keywords
Introduction
Pelvic organ prolapse is a condition characterized by pelvic organ descent due to defect of the ligamentous apparatus. 1 As a result, the quality of life of millions of women is negatively affected.2,3 Today, pelvic organ prolapse ranks third (up to 28%) in the structure of gynecological morbidity in Russia, and 15% of major gynecological surgical interventions are performed for this pathology. 4 Annually, over 300,000 operations for genital prolapse repair are performed in the United States, with cystocele repair being the most common procedure. 5
Synthetic implants were first used for transvaginal pelvic organ prolapse repair in 1996.
The use of 4-strap meshes from different manufacturers was associated with a number of drawbacks, the main of which were weak apical support and the risk of prosthetic shrinkage with subsequent mesh protrusion and vaginal erosions. Apart from these disadvantages, an essential fault of the implantation techniques was the out-in passage of the posterior strap through the sacrospinous ligament. Poor control of trocar passage was accompanied by a comparatively high rate of injury of the genital neurovascular bundle and rectum.
The hazards and drawbacks of the existing 4-strap techniques, the high prevalence of anterior apical prolapse, and strict United States Food and Drug Administration (FDA) control over transvaginal use of implants (they were not recommended from 2011 through 2016) (FDA. Urogynecologic Surgical Mesh: Update on the Safety and Effectiveness of Transvaginal Placement for Pelvic Organ Prolapse, July 2011; FDA. Reclassification of Urogynecologic Surgical Mesh Instrumentation, February 26, 2016) spurred the researchers on to the development of a novel OPUR 6-strap system (Dr. E. Delorme (Private Hospital Sainte Marie, Chalon sur Saone, France) was directly involved in the development of this system).
Pelvic organ fixation with ligaments and fasciae was described by Delancey and Petros.1,6 The ligaments affording the correct position of the pelvic organs are located anteroposteriorly and laterally. The OPUR implant was developed on the basis of this knowledge. The anterior, apical, and lateral bands support the urinary bladder as natural ones. Such a design eliminates the shortcomings of the 4-strap techniques preventing implant shrinkage, forming an adequate support for the base of the bladder and a reliable apical support (Figure 1). Moreover, a special framework was designed, and an in-out technique of posterior transsacrospinous (TSS) trocar introduction was developed as a substitute for the dangerous and unpredictable out-in technique. This allowed for introducing the trocar through the lesser pelvis under manual control outside the “dangerous” ischiorectal area and preventing severe complications associated with the out-in introduction technique employed when placing 4-strap meshes (Figure 2).
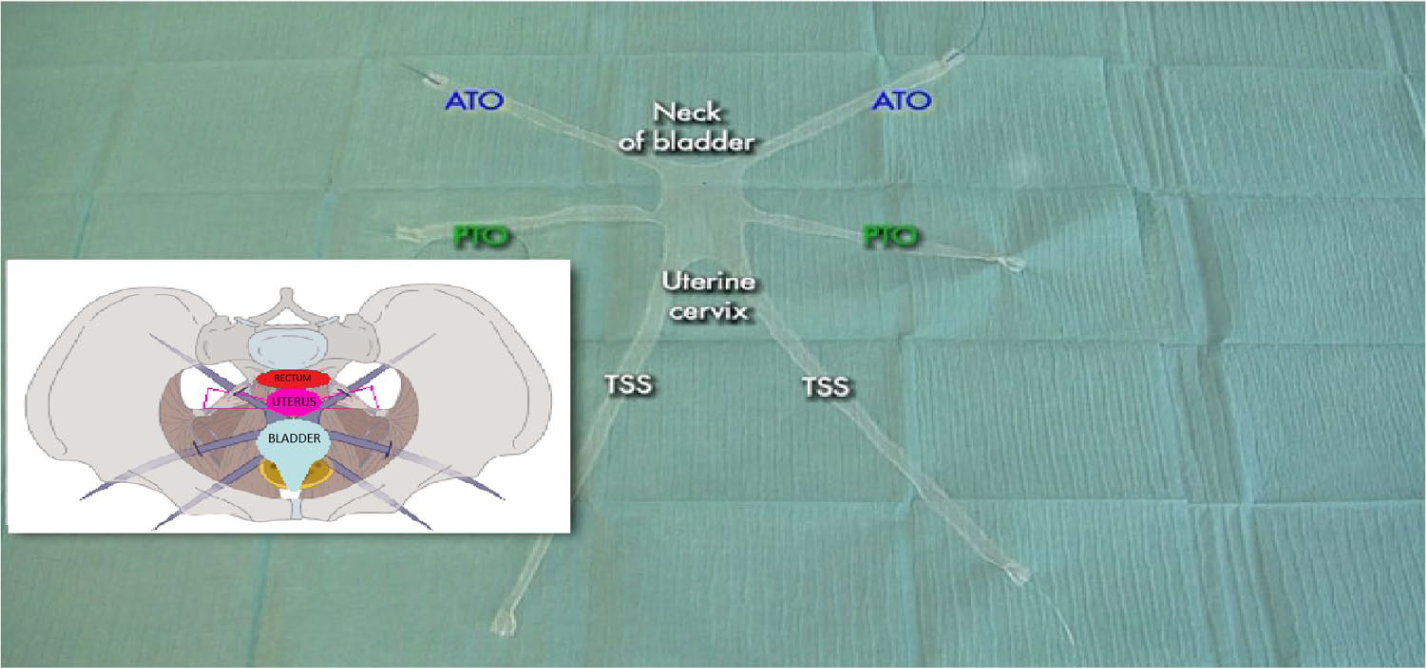
Schematic representation of 6-strap implant positioning for anterior apical prolapse repair.
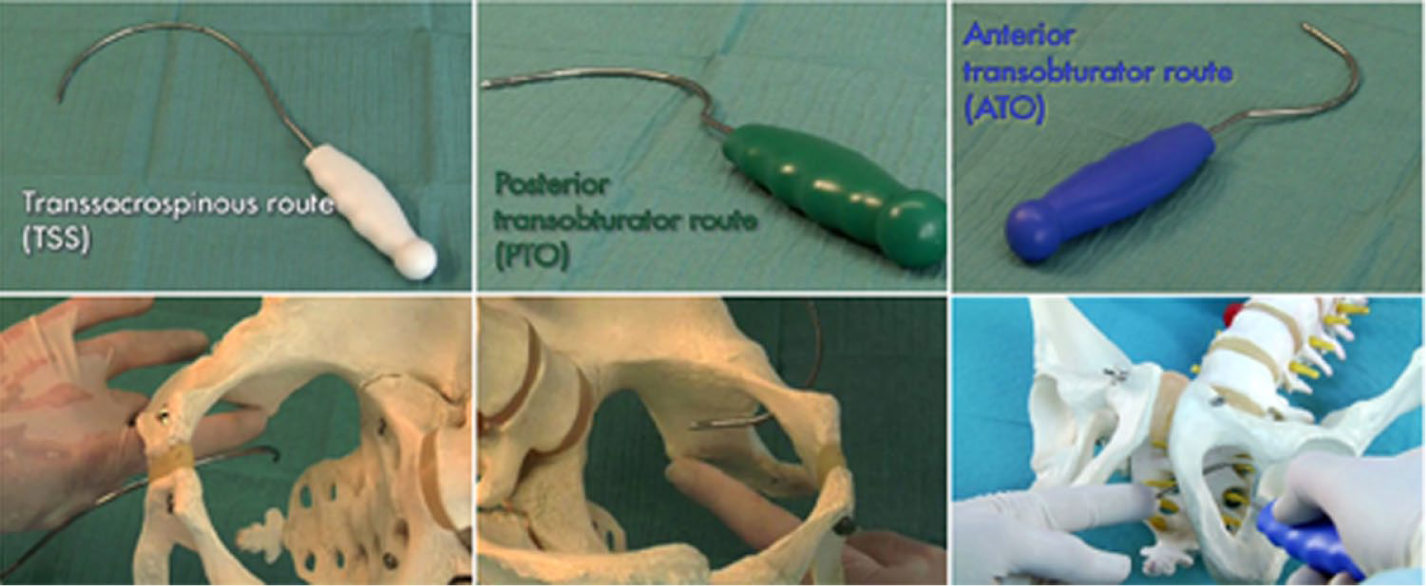
Positioning of trocars.
Our study was designed to assess the outcomes of management of anterior apical prolapse using an OPUR polypropylene mesh implant and to analyze intraoperative and postoperative complications.
Study design
Patients with genitourinary prolapse (n = 142) managed from December 2013 through December 2019 were enrolled. The age of the patients varied between 34 and 78 years (average 57 years). All the patients (100%) had anterior and apical prolapse. In all of them, cystocele was associated with stage III and IV (74% and 26%, respectively) and hysteroptosis with stage II, III, and IV (38%, 60%, and 2%, respectively) (Table 1). The key complaints were foreign body sensations in the vagina and frequent urgent urination. Patients with severe cystocele complained of difficulty urinating. Simultaneous placement of the mid-urethral sling was not performed. The uterus was spared in all cases.
Types and stages of prolapse in patients before and after surgery.
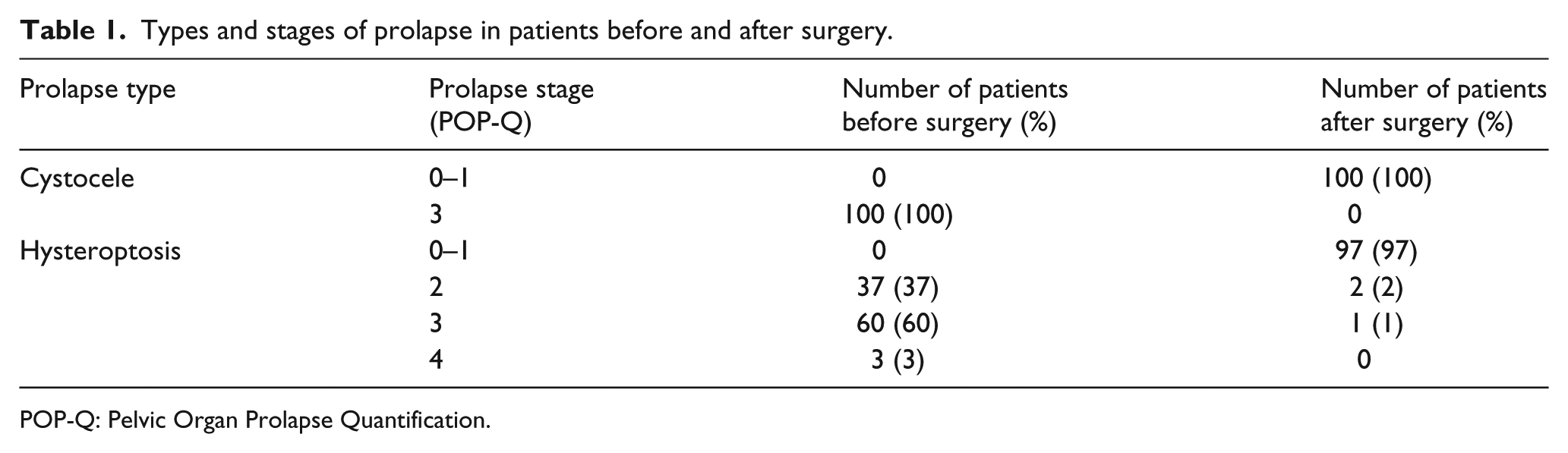
POP-Q: Pelvic Organ Prolapse Quantification.
Exclusion criteria were posterior vaginal wall prolapse and rectocele (grade II and higher), prior hysterectomy, uterine diseases requiring hysterectomy, prior genitourinary prolapse surgery, and insulin-dependent diabetes.
Preoperatively, 75 (53%) patients had frequent sexual activity (once a week or more often).
Mean body mass index (BMI) was 29.0. Forty (28%) patients had unsuccessful experience with various pessaries.
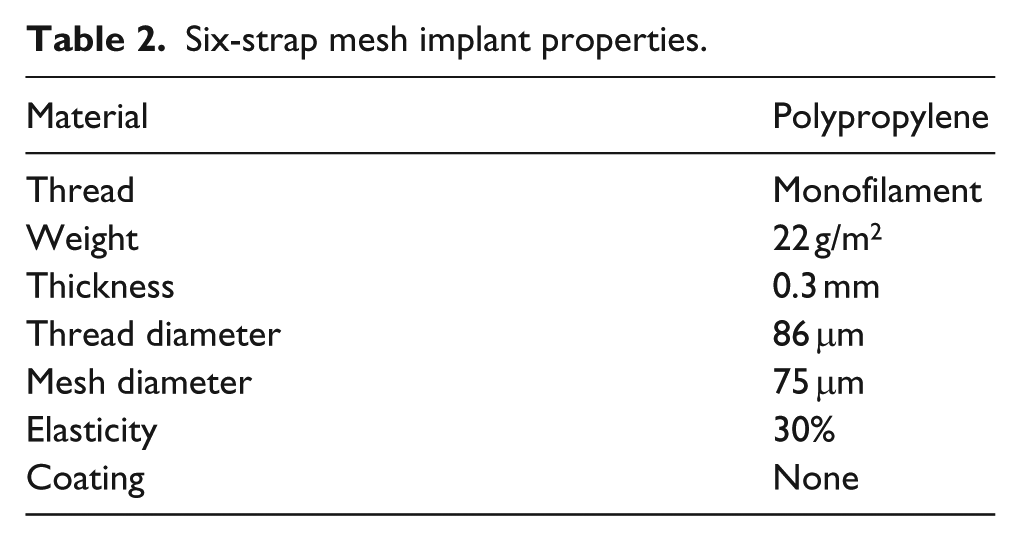
The operations for genitourinary prolapse repair were performed using an OPUR implant (Abiss). The implant characteristics are shown in Table 2.
Six-strap mesh implant properties.
Preoperative examination included the standard laboratory tests, cytology of endocervical scraping and aspirate from the uterine cavity, electrocardiography (ECG), chest X-rays, therapeutist’s and gynecologist’s examinations, and ultrasound examination of the pelvic organs. Uroflowmetry and complex urodynamic tests were performed, and post-void residual urine was assessed. Imitation cough test was performed to predict postoperative stress urinary incontinence (SUI). During the test, the patient is positioned in the examination chair with a full bladder. The uterus and bladder are returned to their normal positions. Following that, the patient is requested to cough. The test is considered positive if there is urine leakage.
The anatomical defect stage was assessed with the Pelvic Organ Prolapse Quantification (POP-Q) score.
All 142 (100%) patients underwent postoperative examination at 1 month with 126 (89%) patients also examined at 12 months after surgery. Subsequent follow-ups were performed on a yearly basis. They were also examined at 1 month and 12 months after surgery by an experienced urogynecologist in an outpatient department. The examination included history taking, using the questionnaires to assess the quality of life and the sexual activity, and evaluating the anatomy of the perineum and the internal genitalia in lithotomy position according to the POP-Q system. The women were examined for protrusion of the mesh implant and potential tissue lesions adherent to the straps; deep palpation of vaginal walls was carried out to pinpoint painful areas. Stage II and higher prolapse according to POP-Q was considered to be a recurrence.
Intraoperative, early postoperative (the period of in-hospital stay), and late postoperative (4 months after surgery) complications were evaluated. The quality of life was assessed according to the following questionnaires: Pelvic Organ Prolapse Distress Inventory 20 (POPDI-20), Pelvic Floor Impact Questionnaire 7 (PFIQ-7), and Pelvic Organ Prolapse/Incontinence Sexual Questionnaire 12 (PISQ-12) (Table 3). Questioning was carried out 1 day before surgery and at 12 months after surgery.
Questionnaire mean scores.
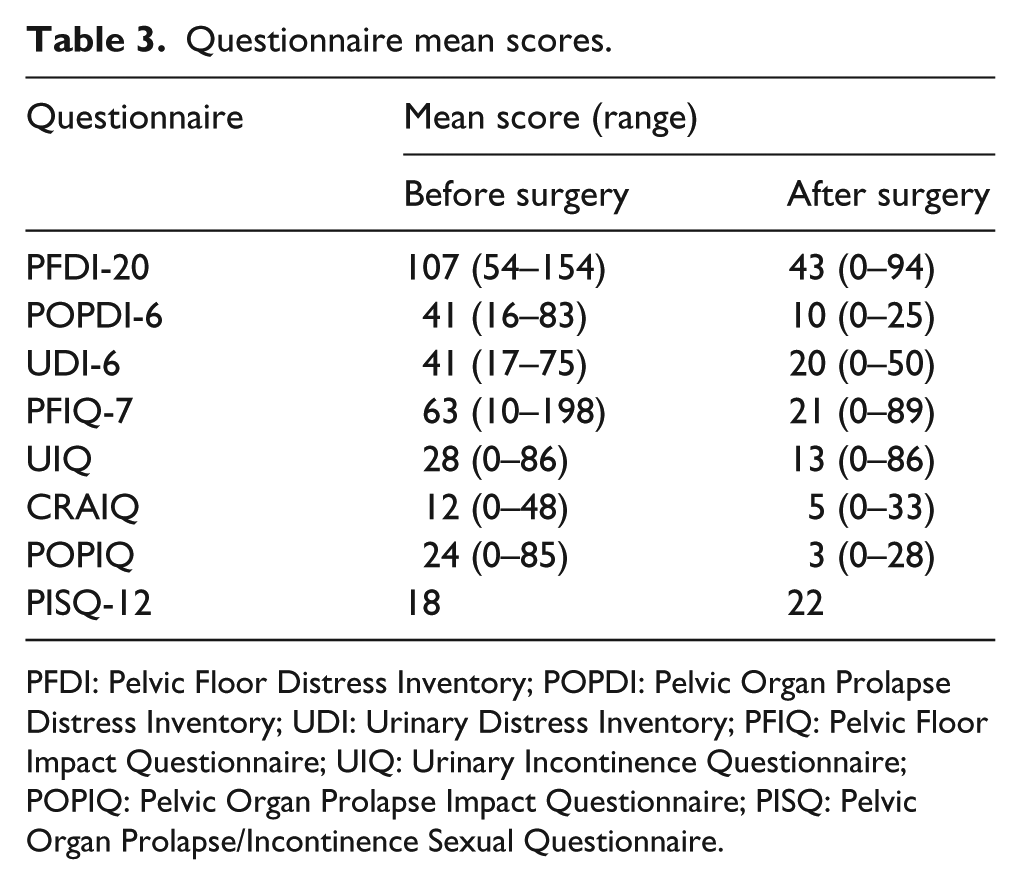
PFDI: Pelvic Floor Distress Inventory; POPDI: Pelvic Organ Prolapse Distress Inventory; UDI: Urinary Distress Inventory; PFIQ: Pelvic Floor Impact Questionnaire; UIQ: Urinary Incontinence Questionnaire; POPIQ: Pelvic Organ Prolapse Impact Questionnaire; PISQ: Pelvic Organ Prolapse/Incontinence Sexual Questionnaire.
The PFDI-20 assesses the degree of functional dysfunction of the pelvic organs based on 20 symptoms. The questionnaire includes three subquestionnaires: Pelvic Organ Prolapse Distress Inventory 6 (POPDI-6) containing questions on pelvic organ prolapse symptoms and Urinary Distress Inventory 6 (UDI-6) revealing functional disorders of the bladder. Median follow-up was 34 months (2–60 months; 95% confidence interval (CI)).
Operative technique
After preliminary hydrodissection, a semicircular transverse incision of the anterior vaginal wall and the pubocervical fascia was made approximately at a level of the isthmus. After the vaginal wall was separated from the bladder in a blunt way, sharp and blunt bladder dissections were made. Midline dissection was made to the point that was approximately 4 cm apart from the meatus, laterally, to reach the tendinous arch of the pelvic fascia. The tendinous arch of the pelvic fascia was dissected with Cooper’s scissors. Blunt digital dissection was then carried out to release the surface of the internal obturator muscle and the sacrospinous ligament, the ischial spine (IS) being the main landmark. The rectum and the bladder were displaced medially. Next, using the appropriate trocars, three pairs of punctures (TSS and two transobturators—anterior transobturator (ATO) and posterior transobturator (PTO)) were made. The in-out TSS trocar was passed through the center of the sacrospinous ligament. It was passed to reach the sacrospinous ligament under digital control which also ensured there was no contact between the trocar and the medially located rectum with the surrounding fatty tissue. The out-in ATO trocar was passed through the pubic notch of the obturator foramen in the pelvic cavity and exteriorized above the tendinous arch of levator ani (ALA) muscles just behind the inferior pubic ramus. The out-in PTO trocar was inserted 1 cm above the sciatic notch of the obturator foramen and passed through the depth of the obturator muscles. It entered the pelvic cavity above the ALA in the middle of the line between the pubis and the IS to avoid traumatic injury of the pudendal neurovascular bundle. The implant was fixed cranially to the isthmus of the uterus anteriorly with non-absorbable ligatures, caudally, to the pubocervical fascia 4 cm apart from the meatus. The implant straps were exposed onto the skin by means of the NITINOL guidewires passed transobturatorly and transsacrospinally. The anterior vaginal wall wound was stitched with running double-row suture (Vicryl 3/0). The sacrospinous straps were tightened as much as possible without compromising intestinal patency, and the transobturator straps were only tightened until the prosthesis was properly spread. When assessing efficacy, stage II and higher prolapse according to POP-Q was considered to be a recurrence.
Results
Of 142 patients, 126 (89%) were available for follow-up within a year after surgery. Seventy-one (50%) have been under medical supervision for 5 years. In 62% of patients, urinary disorders were observed. Among them, the irritative component (urgency, pollakiuria) seen as detrusor overactivity in urodynamic tests was detected in 112 (79%) cases.
Contractility was normal in 110 cases. In two cases, flow and pressure indicators slightly increased immediately after urination. After surgery, overactivity resolved completely or incompletely in 100 patients. In 30 cases (21%), we observed obstructive urination (mainly in women with severe prolapse in which urodynamic tests revealed reduction of detrusor tension). In 31 cases, post-void residual urine was 70–400 mL (mean, 120 mL), and the “pressure-flow” test revealed detrusor hypocontractility. Postoperative urination was evaluated using special questionnaires (The Overactive Bladder Questionnaire (OAB-q) and Urgency, Severity and Impact Questionnaire (USIQ)).
All the patients (100%) had their cystocele managed. In 138 cases (97%), uterine cervix prolapse was repaired. The anatomical results are shown in Table 1.
The mean blood loss was 75 ± 49.6 mL. The operative time was 38–143 min. Of 142 patients, 118 (83%) agreed to fill in the quality of life questionnaires. The results of questioning are shown in Table 3. We did not observe any dependence of the surgical technique features or the outcomes on age and BMI.
Urination quality was assessed at 1 month after surgery. The irritative component completely resolved or became milder in 95 (85%) cases. Obstructive urination was eliminated in all cases (Figure 3). De novo SUI was observed in 11 women (8%). Over the subsequent 12 months, eight of them had slings placed.
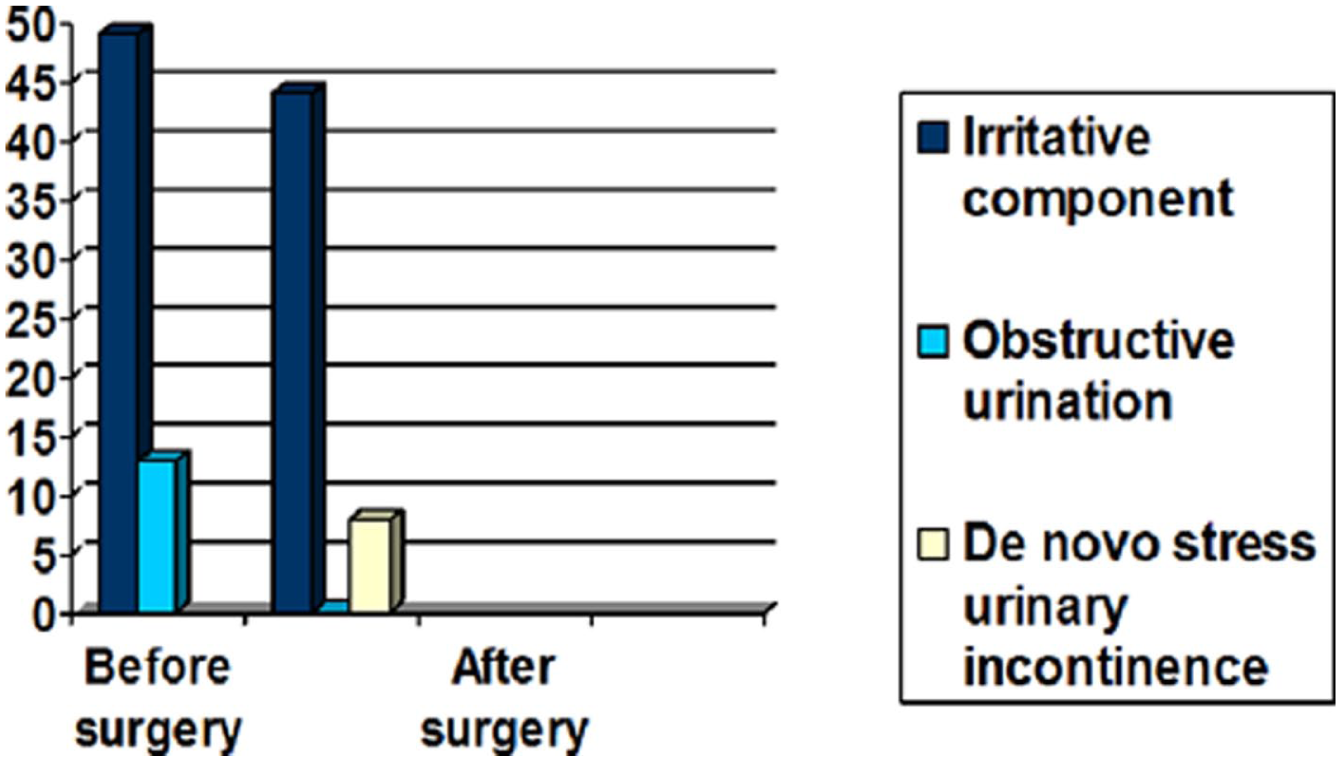
Urination disorders before and after surgery.
In all cases, the patients no longer reported foreign body sensation in the vagina. Questionnaires revealed no cases of dyspareunia, and the patients did not experience any significant painful sensations at 12 months after surgery.
Seventy-five (53%) women were sexually active prior to surgery. Questionnaires showed that at 1 year after surgery, 65 patients remained sexually active. Sexual activity was usually resumed by the third month of follow-up. Analysis of the PISQ-12 score gives evidence of an insignificant improvement in the quality of sexual activity (Table 3).
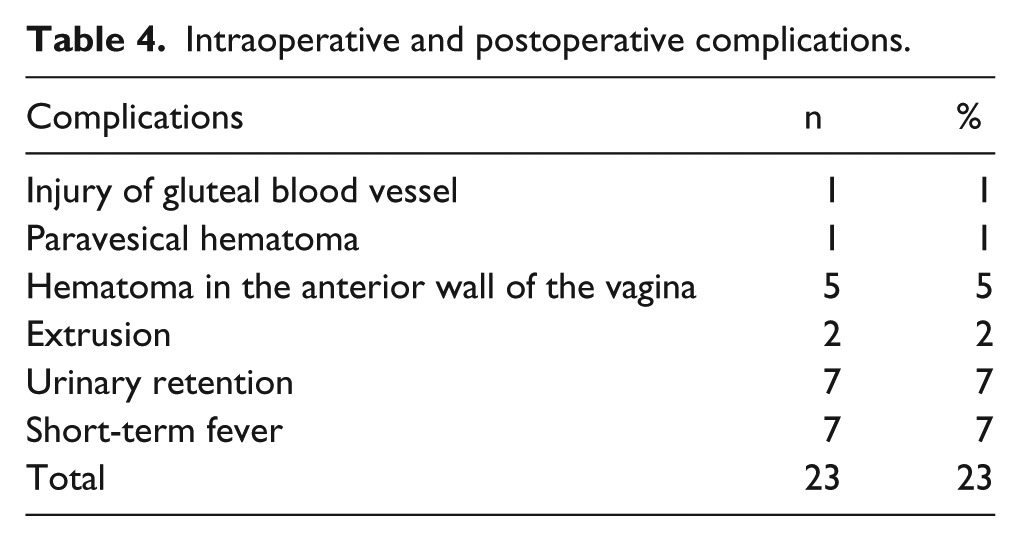
Thirty-five postoperative complications were observed (Table 4). With the exception of mesh fragment excision due to extrusion (n = 2) and bladder injury, detected and sutured intraoperatively (n = 1) (grade IIIa), all the complications were classified as grade I according to the Clavien–Dindo system. Immediately after surgery, most patients (73%) complained of tenderness in the gluteal region, which apparently was associated with a traumatic injury of the sacrospinous ligament and the gluteal muscles. The tenderness did not affect the quality of life or require analgesics and was relieved within 3–10 days after surgery.
Intraoperative and postoperative complications.
Mean hospital stay was 5 days (3–12 days). To date, no recurrence of cystocele has been noted. In three cases, we observed a recurrence of stage II–III hysteroptosis 3 months after surgery.
Hysteroptosis recurrence is still limited to four cases described above.
Discussion
According to the systematized Cochrane 2012 review, 7 surgical repair of anterior prolapse with the techniques using synthetic materials was found to be more efficacious compared to those using one’s own tissues. The trocar techniques in previous years implied “blind” introduction of trocars which carries the risk of injury of pelvic vessels and nerves. As a result, the complications such as bleedings, hematomas, and chronic pelvic pain occurred. Naturally, they contributed to the decline in popularity of the transvaginal mesh surgery using conventional 4-strap prostheses.
An additional disadvantage of previous models was unreliable apical fixation in cases of most frequent anterior and apical prolapse. Moreover, four straps were insufficient for even spreading of the mesh under the bladder. A large number of extrusions resulted from the location of the prosthesis in the immediate vicinity of the longitudinal incision of the front wall of the vagina and failure to follow the technique of two-layer closure of the wound. 7
During development of the OPUR mesh, the authors took into account the shortcomings of previous 4-strap models. 7 OPUR® relies on trocars for implant fixation in pelvic tissues. Three different trocars have been designed for each pair of implant straps: ATO, PTO, and TSS. The trocars’ configuration and the technique of their introduction allow forming channels for the straps at a safe distance from neurovascular bundles with a constant stable trajectory. The posterior TSS trocar is inserted through the middle of the sacrospinous ligament (2–3 cm medial to the IS). Unlike previous 4-strap models, this trocar is inserted using the in-out technique. The rectum is shifted medially, and the trocar insertion is controlled manually. These technique modifications allow for reliable apical fixation and minimizing the risks of rectum and genital neurovascular bundle injury. 7
Minor bleeding/hematomas and postoperative tenderness in the gluteal region are results of insignificant muscle injury. This tenderness does not require special treatment and does not influence the length of hospital stay.
The key diagnostic techniques in our study were assessment of the prolapse stage in the examination chair and imitation tests for predicting de novo incontinence. The quality of life and urination disorders were evaluated using questionnaires. Despite the fact that the assessment of the bladder function in cases of significant prolapse is not often necessary, we preferred to perform the urodynamic tests. Our results revealed that urination disorders in patients with anterior and apical prolapse are mostly irritative and are characterized by detrusor overactivity on cystometry. In cases of significant prolapse, the obstructive component prevailed, sometimes up to substantial urine retention. Normal urination was restored in the majority of cases after surgery. The irritation symptoms that remained in some patients could be due to age-related estrogen deficiency and some other factors. 7
Our results fit into the integral theory, that is, the recovery of normal topography and anatomy of the pelvic organs is followed by normalization of its functions. Weak ligaments and fasciae cannot support the walls of the vagina and the bladder leading to them dropping and sagging. As a result, the stretch receptor activity of the bladder increases, which is accompanied by premature and often urgent urination.
In patients with severe cystocele, obstructive urination and residual urine prevailed as a result of urethrovesical angle becoming smaller. These patients were prone to postoperative ischuria that we believe to be associated with chronic urinary retention and underactive detrusor. Cholinesterase inhibitors and short-term intermittent catheterization led to complete recovery of normal urination. Taking into consideration that urodynamic test results did not influence treatment strategies, the utility of cystometry and “pressure-flow” tests in such patients is debatable.
We did not perform magnetic resonance imaging (MRI), although we are aware that some complex types of prolapse currently require it. 8 We excluded such cases from the study, as well as women who had undergone earlier surgical treatment on the pelvic organs and with uterine diseases that required a separate correction technique.
The results of our investigation are similar to those of the author of the method. 9 Delorme’s and our data are better than those presented for the procedures using the 4-strap techniques,10,11 with lower rates of significant complications.
We only observed four cases of hysteroptosis. In our opinion, such good outcomes are mostly due to the additional mesh straps and uniform distribution of the load on the prosthesis. We believe four factors to be the reason for apical prolapse recurrence: (1) Failure to follow recommendations to avoid physical exercise and excessive intra-abdominal pressure increase when coughing, straining, and so on; (2) The tissue characteristics of the sacrospinous ligament where the muscle tissue component is prevalent over connective tissue; (3) Constitutional causes such as large uterus or wide uterine isthmus; (4) Inadequate cranial implant fixation to the isthmus leading to suture exposure.
SUI is often associated with genitourinary prolapse—75% of cases according to some investigations. 12 SUI masked by anterior prolapse is difficult to detect before surgery. Simulation tests do not guarantee similar results after actual surgery. According to the available data, simultaneous elimination of urinary incontinence during prolapse treatment using the vaginal approach is a rare occurrence. 13 In our study, 11 women developed de novo SUI. In eight cases, incontinence resolved with placement of a mid-urethral sling within a year after surgery.
Temporary gluteal pain due to injury of the sacrospinous ligament and the gluteal muscles occurred frequently in our study (73%). It resolved within the first month of follow-up. Minor pain at the site of the straps sometimes lasted a little longer and resolved within 3 months.
Mesh implant exposure is the most common complication according to published data with the complication rate varying between 3.6% and 18.0%.14–18 The main cause was the overlap of the implant and vaginal wall incision planes. In our study, mesh implant protrusions were observed in two cases (1.4%). Such low rates of erosions and protrusions were achieved by separation of the mesh and transverse incision in the anterior vaginal wall at the level of the uterine isthmus.
Surgical repair of the anatomical defect alone satisfies neither the doctor nor the patient. What is important is to restore the normal function of the pelvic organs. The systematized Cochrane 2012 review devoted to surgical repair of genital prolapse emphasizes the scarcity of data on the quality of life of patients in the studies available, which makes it difficult to assess the effectiveness of surgery. The use of anatomical criteria to formulate indications for operative treatment is being questioned because there is not always a correlation between the extent of prolapse and the degree of the symptoms of dysfunction of descended organs.
As judged by the PISQ-12 score assessment, genital prolapse was noted to exert little influence on the quality of sexual function. These findings are also similar to the results of the study on the quality of sexual function after surgical repair of genital prolapse.19,20 Questionnaires completed at 12 months after surgery by 65 patients who resumed sexual activity revealed no dyspareunia.
While no cases of compromised rectal function were noted in the study, digital rectal examination at the end of surgery is required to ensure rectal patency and rule out its compression by the prosthesis and dislocation toward the sacrum.
The key limitations of our study are its single-center design and relatively small sample, which does not allow for reliable conclusions on long-term safety and efficacy of the technique.
Conclusion
The OPUR mesh for genital prolapse management is an alternative method for simultaneous repair of anterior and apical defects. The results of our investigation demonstrate high effectiveness of surgical treatment of genitourinary prolapse using OPUR. Good anatomical and functional results were obtained for both anterior and apical prolapses. Given the follow-up period of over 5 years for the majority of the patients, we may conclude that transvaginal repair with a 6-strap mesh implant is a viable and effective management option for cystocele and hysteroptosis.
Footnotes
Author contributions
M.E.E., A.N.N., L.M.R., and P.V.G. helped in conception and design, drafting of the manuscript, and supervision. D.V.E. helped in data acquisition and critical revision of the manuscript for important intellectual content. D.O.K. helped in analysis and interpretation of data and statistical analysis. O.V.S. helped in drafting of the manuscript and data acquisition. M.V.L. helped in acquisition of data and statistical analysis.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Research involving human participants
Ethical approval: All procedures performed in the study involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.