
Abstract
Introduction:
Complications due to prosthetic surgery with mesh implantation may be misunderstood due to the insidious clinical presentation and inexperience of many surgeons if not adequately trained for the purpose.
Case report:
A 45-year-old female underwent a trans obturator tape procedure to correct severe stress urinary incontinence 3 months after surgery she developed urethral pain. The sling was partially removed, but the pain persisted. No residue sling was visualized by cystoscopies after surgery, and the pain was attributed to a psychiatric problem. She was treated with opioids, pregabalin without improvement of pain, until an extrusion of the sling into the urethra has been diagnosed by a careful urethrocystoscopy.
Conclusion:
It has been treated in our department by the removal of the residual sling, plus urethroplasty. The patient was followed up at 6 months with resolution of the painful symptoms.
Introduction
The use of synthetic mesh in reconstructive pelvic surgery has increased in the last 20 years. 1
The rising use of synthetic slings has been accompanied by an increase in mesh-related complications. The US Food and Drug Administration noted a spread of complications from 2005–2007 to 2008–2010. 2 Complications from Mid urethral sling(MUS) surgery include (most common) mesh exposure or extrusion, chronic pelvic pain, dyspareunia, mesh contracture, neuromuscular injury, and/or perforation. 3 For these reasons the use of pubo-coccigeal autologous sling has gained consensus again in female pelvic surgery. 4
This case report aimed to highlight how underestimating the signs and symptoms of a woman undergoing vaginal prosthesis surgery can delay the diagnosis of a complication.
Case description
A 45-year-old female with three past vaginal deliveries and no comorbidities underwent a transobturator tape (TOT) procedure to correct severe (8–pads/day) urinary incontinence in January 2011 by other department.
After the procedure, incontinence disappeared. However, 3 months later, the patient developed persistent urethral pain and was referred to the gynecology service. In July 2013, she was operated on and the mesh was removed. Unfortunately, after mesh removal, the patient claimed to have worsening of symptoms that were not present prior to the sling surgery, namely pain persistence, urgency, mild voiding dysfunction, and severe urinary incontinence.
Pain persistence was interpreted as neuropathic pain (chronic pelvic pain). She received different drugs (opioids, pregabalin) without improvement of symptoms.
On March 2014, she visited the Urogynecology Unit of the Urological and Andrological Clinic for the first time. Her symptoms were urethral and suprapubic pain unresponsive to drugs, urinary urgency, mild voiding dysfunction, and severe urinary incontinence.
All previous diagnostic tests performed in other urological centers did not reveal any objective cause of the clinical picture. Cystoscopy, suprapubic ultrasound, magnetic resonance imaging, urinalysis (20–30 leukocytes), and urine culture (vaginal and cervical swabs, negative) were inconclusive.
Given the absence of anomalies in the diagnostic tests performed, other physicians believed that the patient had a psychiatric disorder (depression and somatic symptom disorder).
Clinical evaluation demonstrated no signs of vaginal mesh exposure, urethral hypermobility, stage I cystocele, no rectocele, no uterine prolapse, mild urethral ectropion, positive stress test, and severe tenderness upon urethral palpation. The patient underwent translabial sonography, which showed a hyperechoic urethral spot 23 mm from the bladder neck that surrounded the urethra and a mild hypoechoic periurethral area (Figure 1). The second cystoscopy showed the presence of the previous sling crossing the urethra (Figure 2). The patient had another surgery to remove the sling through using the vaginal approach. A mid-urethral incision allowed us to find the full tape around the urethra. Surprisingly, it had not been removed during the previous surgery in 2013.

Translabial sonography. Urethral hyperechoic spot at 23 mm from the bladder neck that surrounds the urethra, with a mild hypoechoic periurethral area.
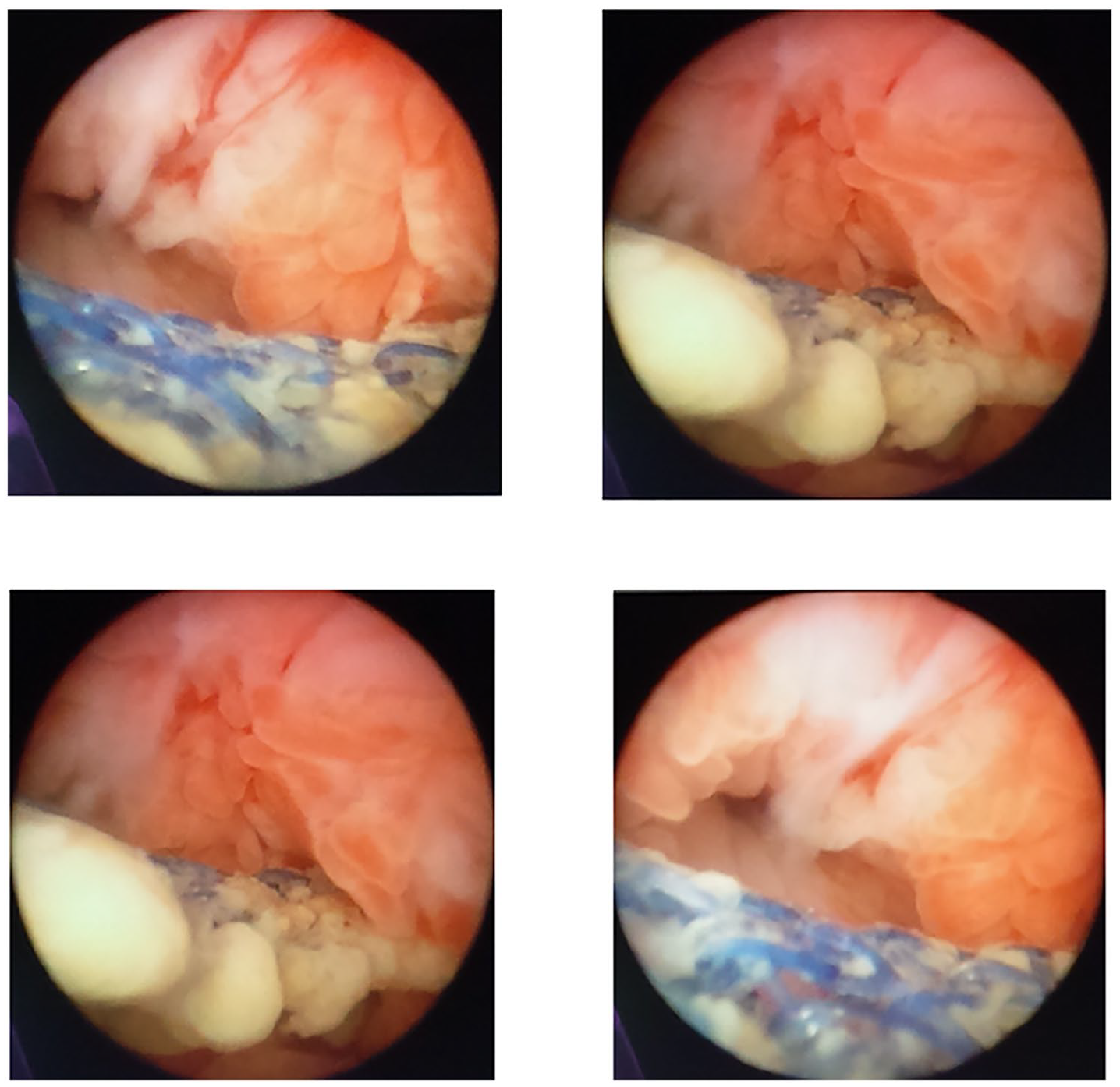
Cystoscopy.
After completing transvaginal mesh removal, deep intra-obturator arms were excluded and double-layer termino-terminal urethroplasty was performed (Figure 3).
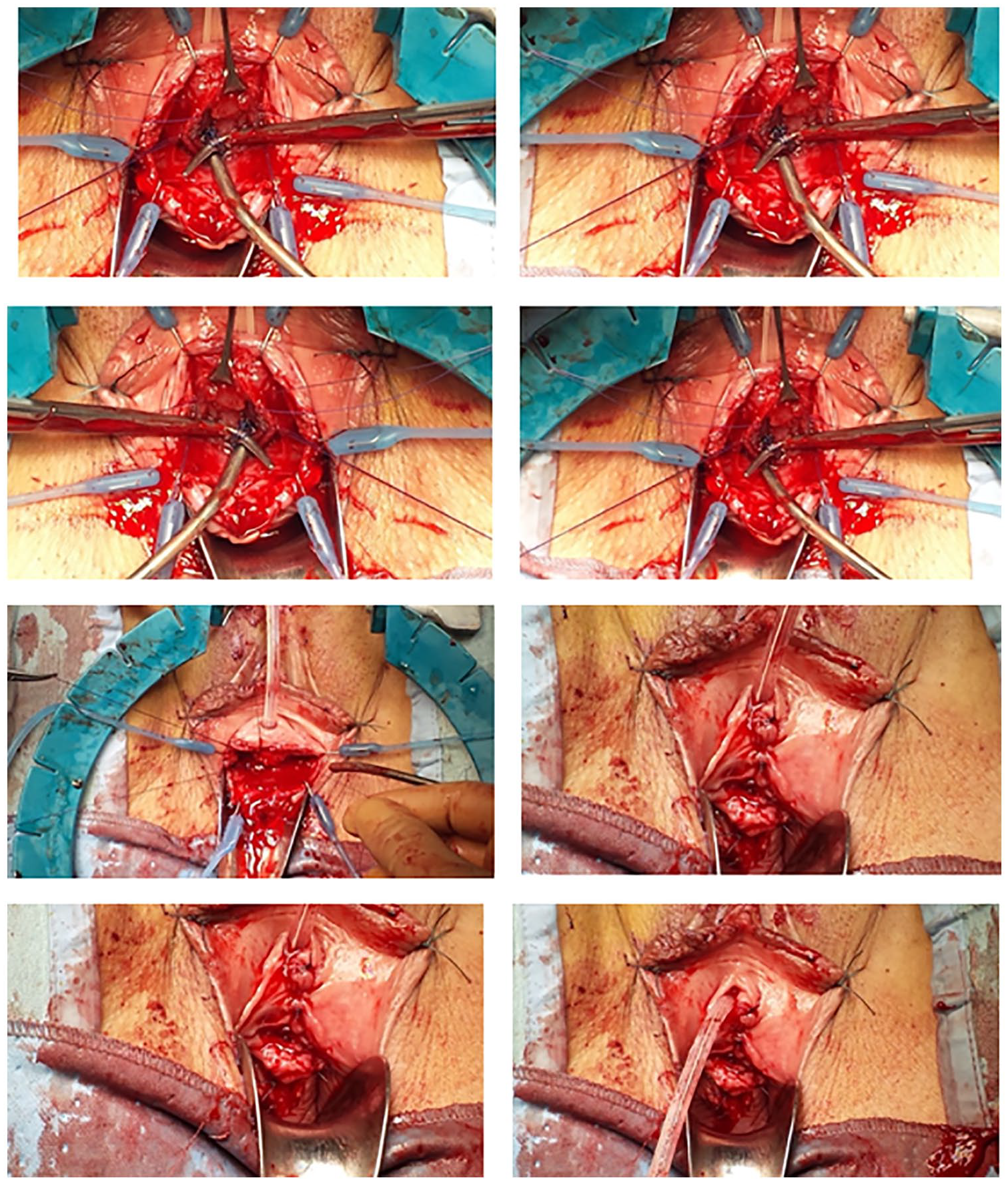
Intra-operative surgery; removal of the mesh and double layer urethroplasty.
On the first postoperative day, the patient had complete pain relief. After 20 days, she underwent bladder catheter removal and cystography did not show the presence of urethro-vaginal fistula.
The patient was followed up at 6 months after resolution of the painful symptoms.
During the clinical assessment, the patient complained of stress urinary incontinence (SUI) during moderate-to-severe efforts with a positive stress test due to urinary stress incontinence persisted at follow-up. The patient opted not to have any further surgical interventions to correct this problem. She tolerated the urethral pain until it finally disappeared without any further treatment.
Conclusion
This case report showed how late diagnosis of a mesh complication, inappropriate treatment thereof, and underestimation of persistent symptoms can result in serious consequences. The first mistake was claiming to have removed the sling completely in 2013. It is difficult to remove a MUS once implanted. Consequently, the extrusion sling was not visualized during the first cystoscopy and may have been mistaken as a fibrous reaction. Thus, symptoms were not considered to be due to the probable persistence of a sling around the urethra.
After 10 years follow-up in a tertiary urogynecological center study, no case of urethral sling extrusion was noted. 5 Vaginal sling exposure was 3%. 6 Sling extrusion was reported in 0.2%–0.3% of patients. 7
In another case report, the mesh eroded into the urethra up to the bladder neck with symptoms mimicking a bladder cancer, and was successfully treated by a suprapubic-assisted transurethral excision; this case showed that multiple approaches to remove the mesh should be carefully considered after accurate mesh identification, and the final procedure should be as radical as possible. 8
Pain is usually related to mesh usage, and it decreases with time. The incidence of groin pain after TOT was 2.3%–15.9%. 9
Chronic pelvic pain may develop in patients with incidence ranging from 2.9% to 25%. 9 Chronic pain, conventionally defined as pain persisting >6 weeks, is not common. The etiopathogenesis of pain after vaginal surgery is not well understood. Etiologic factors may be endopelvic hematoma formation, local infection, nerve injury, and muscle injury by inappropriate positioning of the mesh.
Rigaud et al. demonstrated that in approximately 88% of chronic pelvic pain cases, there was an abnormality in mesh position. Most frequent position abnormalities were in the anus elevator, near the obturator nerve, and bladder wall. 10 Another theory was the presence of oxidative reaction by local neutrophil influx. These can release inflammatory cytokines and cause chronic inflammation. 10
In our case, the pain was considered to have vaginal origin. However, during micturition, it worsened and persisted after voiding.
Patients with painful symptoms following mesh implantation should be carefully evaluated. It is important to determine whether the pain was present before mesh implantation or occurred after surgery. In addition, a thorough clinical examination is required. In particular, abdominal, vaginal, and thigh physical examination must be performed. Upon physical examination, the pain had a specific trigger point along the urethra. The first step is to understand the pathophysiology of pain. The absence of any clinical result has misled physicians in fact, the diagnosis was oriented towards a neurological and even psychiatric problem.
The patient spent 1 year in a debilitating situation under anti-depressant and opioid therapy with a terrible quality of life and without any support.
Another consideration is that cystoscopy (without urethroscopy) performed by urologists not specialized in urogynecological field can lead to no diagnosis being made.
This case is unique because it is linked to a possible wrong initial diagnosis of the complication. It implied that an incorrect surgical operation was performed. These events, although rare, represent a clinical reality where the reiteration of the diagnostic error can lead to extremely difficult situations.
It is necessary to carefully evaluate rather than underestimate what woman reports, and a well-conducted clinical examination is more important than any superficial and inadequate assessment. Multiple approaches to remove the mesh should be always considered after good mesh identification, and the chosen procedure should be as radical as possible to achieve the best result.
Footnotes
Authors’ contributions
E.I.: drafting the manuscript and given final approval of the version to be published; F.T.: acquisition of data and given final approval of the version to be published; L.M.V.: acquisition of data and English revision of the draft; V.M.: data analysis and given final approval of the version to be published; G.C.: interpretation of data and given final approval of the version to be published; E.C.: conception and design, general coordinator of the study, and given final approval of the version to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.