
Abstract
Objective:
To study the effect of a novel technique of posterior reconstruction of pubourethralis on early return of continence after robot assisted radical prostatectomy (RARP).
Materials and methods:
The study included 206 patients of organ confined prostate cancer managed at our centre between March 2014 and December 2018.The patients were randomly distributed into two comparable groups with respect to age, height, weight and BMI, with 100 patients in control and 106 patients in study group. After standard excision of the specimen, the posterior reconstruction in the form of Rocco stitch was done in control group while in addition to Rocco stitch pubourethralis was approximated posteriorly in midline at the proposed site of vesicourethral anastomosis in study group. Continence was defined as the need to use 0–1 pad in 24 h. The data was collected on day 0, 3, 7, 15, 30, 90 and 180 after removal of catheter.
Results:
At day zero, 3,7, 15, 30, 90 and 180 days after catheter removal continence rates (⩽1 pad usage per day) were observed to be 18.8% versus 0%, 22.6% versus 0%, 50.9% versus 5%, 72.6% versus 20%, 84.9 versus 32%, 97.1% versus 83%, and 97.1% versus 91% in the study and control group respectively.
Conclusion:
Despite small number of patients in this study the results with respect to early return of continence are encouraging in the reconstruction group and there by in favour of this technique .Furthermore the technique is easily reproducible and may be seen as one more additional step to be applied in order to enhance the recovery of continence after RARP. However it is necessary to further validate the efficacy of this procedure through multicenteric controlled trials.
Introduction
Robot assisted radical prostatectomy (RARP) has been documented to be a viable solution for organ confined disease since 2008. 1 Currently it is the standard of care for disease confined to prostate gland. Despite it being an effective treatment modality for good oncological outcome, the two major concerns after the RARP are risk of incontinence and erectile function. The avoidance of these two adverse associates has been an important marker of success of RARP. The excellent view afforded by the 3D vision has enhanced the expertise of the surgeons with development of increasingly precise dissection techniques resulting in improved outcomes for the patients. Many techniques have been described in an effort to enhance continence rates post radical prostatectomy including peri-urethral suspension (SS),2–5 anterior reconstruction (AR) 6 posterior reconstruction (PR), 7 total anatomic reconstruction (TAR) 6 and various nerve sparing techniques (NS).8–10 Overall the literature suggests benefit of performing an additional repair along with a conventional Van Velthoven anastomosis, with many studies showing continence rate at 1 year post radical prostatectomy being greater than 90%.11–13
The levator ani muscle is considered the most important supportive system of the pelvic floor and has been divided into many portions, according to their attachments or physiological functions. The levator ani muscle is subdivided into the ischiococcygeus, iliococcygeus and pubococcygeus portions. The pubococcygeus muscle is often subdivided into separate parts according to the pelvic viscera to which they relate, that is, pubourethralis and puborectalis in the male. At the level of the urethra and the rectum, the muscle bundles of the pubococcygeus muscle are continuous with those controlateral, forming a sling (pubourethralis and puborectalis). 14
During RARP pubourethralis muscle sling is often splayed wide apart due to dissection from the apex of prostate which is much wider than the urethra. In the present study we describe a novel technique of posterior approximation of a pubourethralis by a reinforcement stitch using a 3-0 barbed suture and its effect on early recovery of continence post RARP.
Materials and methods
This was a prospective interventional study conducted in the department of urology and robotic surgery at Indraprastha Apollo hospital, New Delhi after due clearance from the hospital’s ethics committee. The study included 206 patients of organ confined prostate cancer suitable for radical prostatectomy managed at our centre between March 2014 and December 2018.The patients were randomly distributed into two comparable groups with respect to age, height, weight and BMI, with 100 patients in control and 106 patients in study group. After standard excision of the specimen, the posterior reconstruction in the form of Rocco stitch was done in control group while in addition to Rocco stitch pubourethralis was approximated posteriorly in midline at the proposed site of vesicourethral anastomosis in study group. Continence was defined as the need to use 0-1 pad in 24 h. The data was collected on day 0, 3, 7, 15, 30, 90 and 180 after removal of catheter. All the patients were continent before surgery
Treatment protocol
After obtaining due informed consent from the patients, prospective data was collected and recorded. Baseline demographic data such as age, height, weight and BMI was recorded. A detailed history, clinical examination and baseline evaluation along with initial serum PSA (iPSA), TRUS guided prostatic biopsy with Gleason score was tabulated. After confirming tissue diagnosis on TRUS guided biopsy, all patients were suitably counselled about the treatment options. Those who opted for RARP were taken for procedure after 6 weeks of biopsy. All the patients were operated by single surgeon.
Patients were prepared by passing them through adequate pre anaesthesia clearances in a standardized pre operative protocol. A trans peritoneal six-port approach was used in each case, using da Vinci Si surgical robotic system (Intuitive Surgical, Sunnyvale, CA, USA). The patients were placed in the low lithotomy with deep Trendelenberg position. A standard pelvic lymphadenectomy was performed in all cases. Posterior first approach was undertaken, isolating the vasa defferentia and seminal vesicles. Following this, the bladder was dropped and endo pelvic fascia was incised. The dissection of the antero-lateral aspect of prostate on either side was done sharply, lifting off the fibres of levator ani muscle. Anteriorly the dissection was carried out up to the prostato- urethral notch, thereby clearly demarcating the inverted pyramidal shaped bundle of muscle fibres closely applied to prostato-urethral junction on either side. These bundles, which form the pubo urethralis part of levator ani complex, were carefully identified in each case, as these are the muscle bundles which were sutured posteriorly behind the proposed vesico urethral anastomosis to give an additional resistance to bladder outlet. Early ligation of dorsal venous complex (DVC) was performed, followed by bladder neck dissection and ligation and release of lateral prostatic pedicles. The nerve sparing dissection was performed on both sides unless indicated otherwise depending upon the intra operative findings. The DVC was divided and suture ligated if required. The urethra was carefully dissected off the prostatic apex and divided to free the specimen, which was bagged instantly. A Rocco stitch was placed in all cases using an absorbable 3-0 barbed suture. The pubourethralis muscle bundles were identified as inverted pyramid shaped muscle on either sides of the urethral stump. They were regarded as the ‘pillars of continence’ by the authors. A running absorbable 3-0 barbed suture with two or three throws on either side was taken to approximate the posterior apices of the pubourethralis muscle bundles to be brought to midline just posterior to the proposed site for vesicourethral anastomosis (Figure 1).The anastomosis was made as described by Van Velthoven et al. using 3-0 absorbable barbed suture. A silicone 18 F catheter was placed across the anastomosis. Postoperative analgesia was administered with non opioid agents, and patient controlled intravenous opioid as per the standard post operative protocol followed in the hospital. Console time was same in both the groups (2–4 h, average 187 min).All the procedures were nerve sparing.
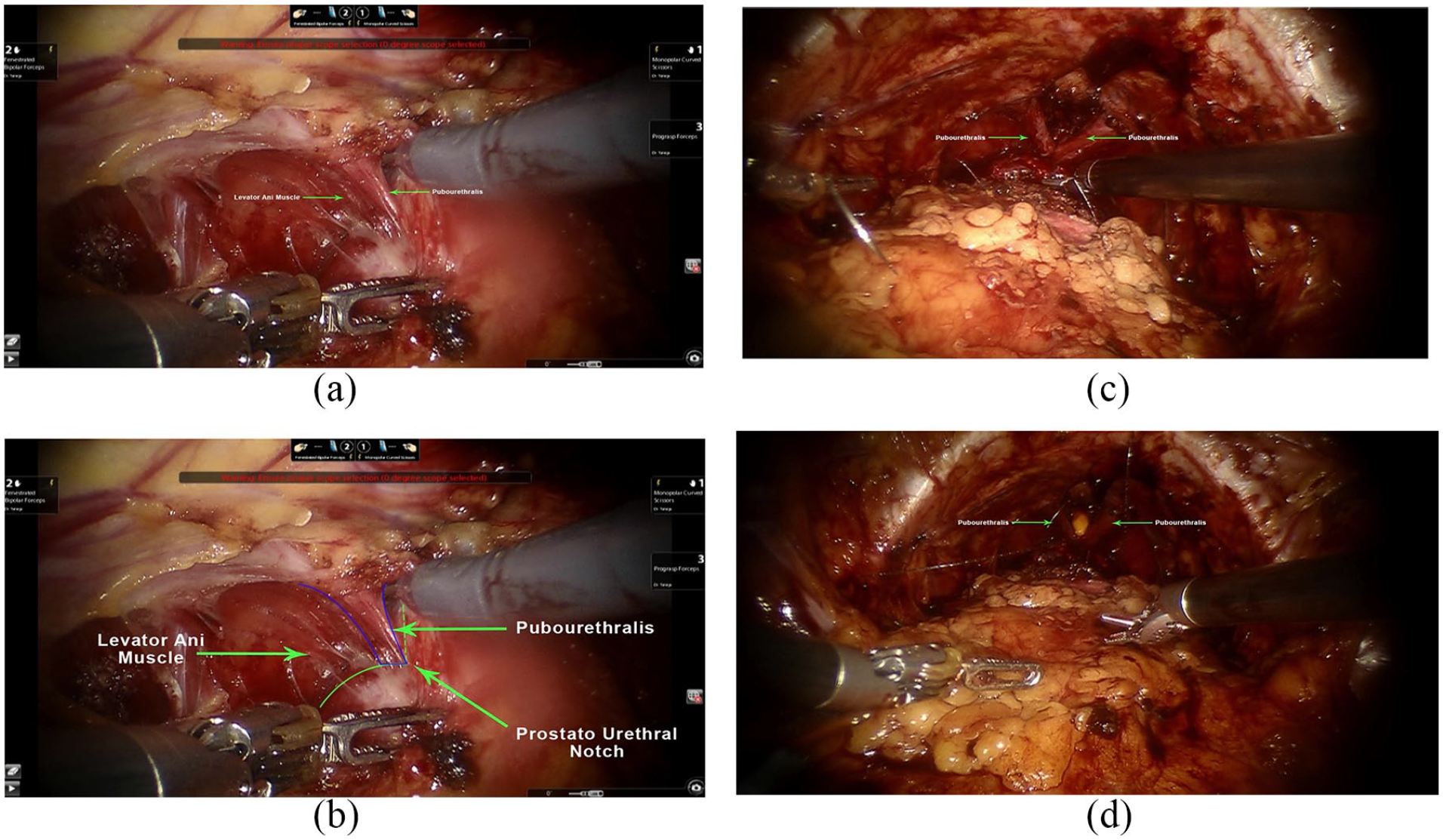
(a–d) Intra-operative pictures of anatomical dissection and reconstruction of pubourethralis.
After RARP the patients were ambulated on first postoperative day of surgery. The drain was removed once the patient passed flatus. Patients were discharged with indwelling catheter once they were ambulatory, tolerating diet.
Patients returned to out patient department 14 days after surgery for catheter removal. Return of continence was assessed on day of catheter removal, day One, day 3, day 7, day 15, day 30, day 90 and day 180. Patients were briefed about the process of estimation of extent of incontinence during their stay in the hospital itself, which was reinforced at the time of removal of catheter. On the day of catheter removal all patients were advised to wear an adult diaper. Depending upon the quantum of leakage of urine they were advised to change from the diaper to protection pads (underwear linings) and record the number of diapers/protective pads per day. The diaper was changed when patient used to feel moist. All the patients were advised to do Kegel exercises post operatively.
The number of diapers used per day was recorded till patient become dry. Urinary incontinence, was evaluated with the following question:
‘How often do you change pad, diaper or sanitary aid during a typical day (24 h) with response alternatives’:
“Not applicable” I don’t use any protective pad (score = 0).
Once or less than once/day (score = 1).
About 2 times/day (score = 2).
About 3 times/day (score = 3).
About 4 times or more/day (score = 4).
About 5 times or more/day (score = 5).
When the number of protective pads was reduced to one a day, they were classified as reasonably continent. When they did not require any protective pads, they were termed fully continent. Incontinence was defined as score of 2 and above. This is accordance with previous researchers. 15
Observation and results
In our study mean age of presentation was 67 years .The mean console time was 110 min (range 90–140 min). Average blood loss was 30 ml (range 10–100 ml). Mean duration of stay in the hospital was 3 days (range 2–14).
After removal of Foleys catheter on post op day 14, continence was assessed as per the protocol of the study. At day zero, 3, 7, 15, 30, 90 and 180 days continence rates (⩽1 pad usage per day ) were 18.8% (20) versus 0%, 22.6 %(24) versus 0%, 50.9%(54) vs 5%(5), 72.6%(77) versus 20% (20), 84.9% (90) versus 32%(32), 97.1% (103) versus 83% (83)and 97.1%(103) versus 91% (91) in the study and control group respectively (Tables 1 and 2).
Number of pads used per day by patients in days after catheter removal.
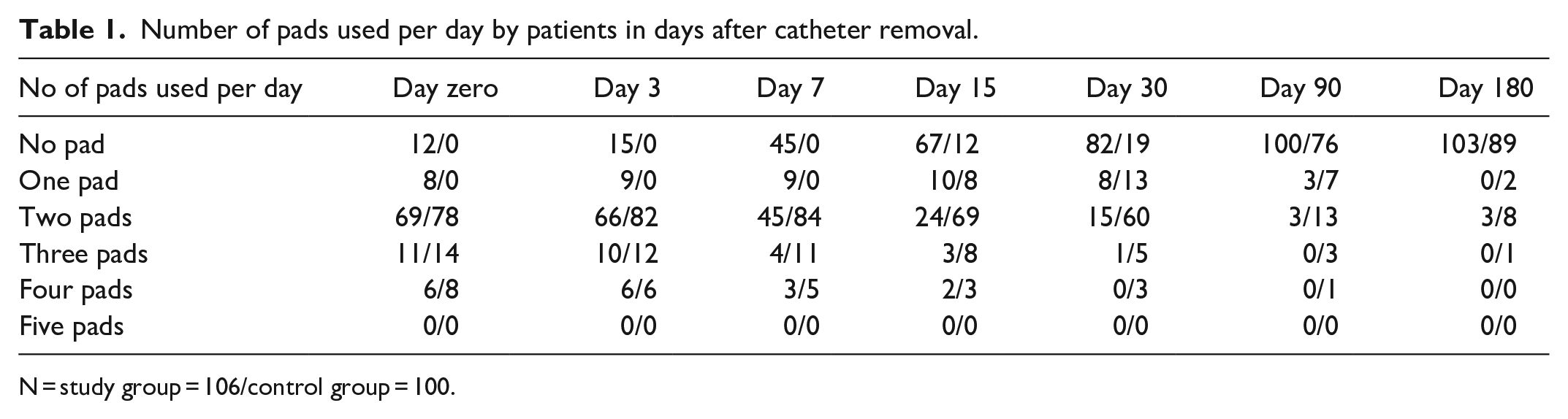
N = study group = 106/control group = 100.
Continence status of patients after catheter removal.

N = study group (106) /control group (100).
Sixteen patients in study group and 10 patients in control group who were continent complained of urinary urgency. These patients were managed with oral extended release tolterodine 2 mg once daily with good results.
No correlation was seen between prostate size and age with respect to continence.
No specific adverse effects attributable to this technique were observed.
As for as complications are concerned two patients in the study group had complications .One of the patients had introperative ureteric injury which was detected introperatively and ureteric reimplantation was done while other patient had ileus post operatively which settled with conservative management after 2 weeks. None of the patients in the study group had vesico-urethral stenosis or post operative urinary retention.
Discussion
It is clear from the published literature that the return of continence after RARP is an enigmatic issue with unclear physiological explanations. This has resulted in various attempts that have been made in order to enhance the recovery of continence after RARP. The fact that none of these attempts has been found to be exacting, we decided to make yet another such attempt. The posterior approximating suture on the pubourethralis muscle in the present series was hypothesized to augment the bladder outflow resistance in more than one ways.
This suture was aimed to approximate the two pubourethralis muscles on either side in midline posteriorly, with a thought to better co apt the rhabdosphincter.
The placement of this suture resulted in adding bulk of muscle padding just posterior to the vesicourethral anastomosis site, resulting in angulation of the vesicourethral junction. This in an upright posture would seem to offset the posterior urethra ventrally thus increasing the out flow resistance (Figure 2).
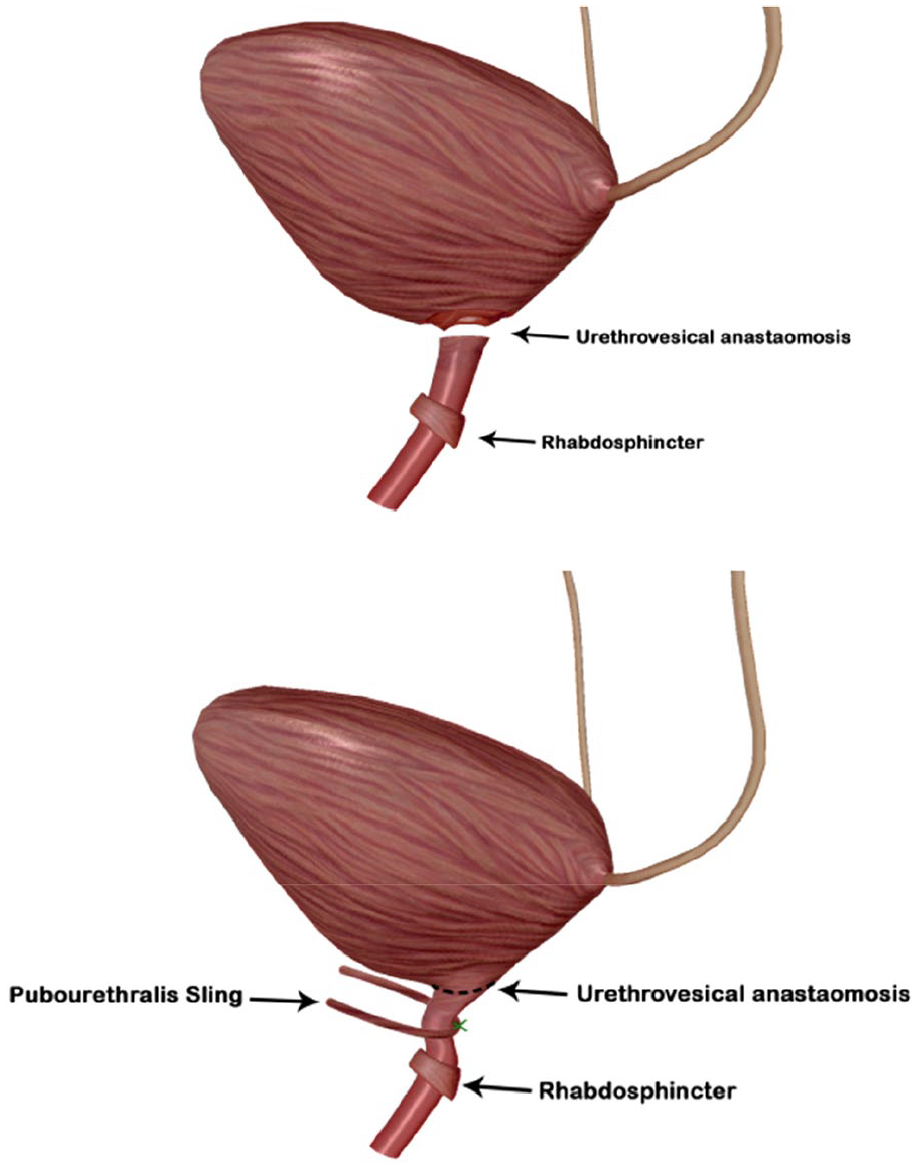
Schematic diagram representing effect of posterior reconstruction of Pubourethralis.
When the technique was initially applied the first four patients became continent upon catheter removal. This encouraged us to enrol more patients for this technique.
The fact that over all four patients were totally continent within 24 h after removal of catheter (not requiring a single protective pad), there is indeed a reason to believe that this technique of posterior reinforcement of pubourethralis adds to the over all recovery of continence after RARP. Although the number of patients is less but the modification seams to improve the early recovery of continence after RARP.
In most of the studies continence after RARP has been described as no pad or single pad usage per day. In a study by Patel VR et al continence has been assessed at 1, 3, 6 and 12 months with the continence rate being reported as 40%, 92.8%, 97.9% and 97.9%, respectively. 2 In another study by Mun Su Chung et al percentage of patients continent has been reported as 42.1%, 70.1% and 89.7%, at 3, 6, and 12 months, respectively. 16
In the present study we have studied the recovery of continence(⩽one pad usage per day ) with and without posterior reconstruction of pubourethralis after robotic assisted radical prostatectomy at zero, 3, 7, 15, 30, 90 and 180 days after catheter removal was 18.8% (20) versus 0%, 22.6% (24) versus 0%, 50.9% (54) versus 5% (5), 72.6% (77) versus 20% (20), 84.9% (90) versus 32% (32), 97.1% (103) versus 83%(83) and 97.1% (103) versus 91% (91) in the study and control group respectively (Tables 1 and 2).
Some of the studies which focused on the early return of continence include Effect of puboprostatic ligament reconstruction on continence recovery after robot-assisted laparoscopic prostatectomy by Stefano Puliatti et al in which Complete continence (no pads) rates were reported at time of catheter removal (T0), 1 month (T1), 4 months (T4), 6 months (T6) and 12 months (T12) postoperatively. Moreover, the social continence (0–1 security pad) was reported at 12 months postoperatively. Complete continence was significantly different between both groups at T0 and T6 (p = 0.022, and p = 0.035, respectively). The social continence was not significantly different between both groups (85.1% vs 89.6% in group A vs group B). 17
While in Total anatomical reconstruction during robot-assisted radical prostatectomy by Matteo Manfredi et al, 1008 patients were enrolled and continence was assessed at 24 h, and 1, 4, 12, 24 and 48 weeks after catheter removal, 621 (61.61%), 594 (58.93%), 803 (79.66%), 912 (90.48%), 950 (94.25%) and 956 (94.84%) patients were continent, respectively. In the logistic regression model, the variables analysed had a higher impact on continence recovery at 4 and 12 weeks. At 4 weeks, the postoperative odds of urinary continence recovery increased with the absence of diabetes (odds ratio [OR] 2.76, 95% confidence interval [CI] 1.41–5.41) and D’Amico low vs high risk (OR 2.01, 95% CI 1.01–3.99). At 12 weeks, urinary continence increased with the absence of diabetes (OR 3.01, 95% CI 1.23–7.35), D’Amico low vs high risk (OR 4.04, 95% CI 1.56–10.47), and D’Amico intermediate vs high risk (OR 3.33, 95% CI 1.66–6.70). ROC curves were drawn and an AUC value of 61.9% (95% CI 57.49–66.36) at 4 weeks and 63.8% (95% CI 58.03–69.65) at 12 weeks were computed. 18
During the period of current study, Student et al reported a similar technique. 19 In their study continence has been assessed at 24 h, 2 weeks, 4 weeks, 8 weeks, 6 months and 12 months, with continence rates reported as 21.9% at 24 h, 43.8% at 2 week, 62.5% at 4 week, 68.8% at 8 week, 75.0% 6 months, and 86.66% 12 months, respectively. 17 It is interesting that similar thought process has dwelled upon the minds of groups working almost simultaneously in different parts of globe, the present study was conceived and registered at the hospital’s ethics committee in February 2016.
Conclusion
Despite small number of patients in this study the results with respect to early return of continence are encouraging in the reconstruction group and there by in favour of this technique .Furthermore the technique is easily reproducible and may be seen as one more additional step to be applied in order to enhance the recovery of continence after RARP. However it is necessary to further validate the efficacy of this procedure through multicenteric controlled trials.
Footnotes
Acknowledgements
Highly thankful to my guide Dr rajesh Taneja for his support.
Author contribution
Malik Abdul Rouf: Project development, Manuscript writing; Rajesh Taneja: Project development, Manuscript editng; Anshuman Agarwal, Project development; Suresh Kumar Rawat Project development; Venkatesh Kumar: data collection; Mahender Sharma, data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Approved by institutional ethics committee.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Explained and Taken.
Guaranter
Academics Indraprastha Apollo Hospitals Sarita Vihar, New Delhi.