
Abstract
Purpose:
We investigated role of neutrophil-to-lymphocyte ratio (NLR) in the diagnosis and prediction of extracapsular extension (ECE) in clinically localized prostate cancer (PCa).
Materials and methods:
A total of 396 patients with clinically localized PCa who underwent open radical retropubic prostatectomy (RRP), and 260 patients with benign prostatic hyperplasia (BPH) who underwent suprapubic prostatectomy were included in the study. Preoperative NLR, prostate specific antigen (PSA), prostate specific antigen density (PSAD), free PSA, prostate volume (PV), free/total PSA (f/t PSA) in both groups, and relation of NLR with PSA, Gleason Score (GS), and pathologic stage in PCa group were investigated. Records of patients were analyzed retrospectively.
Results:
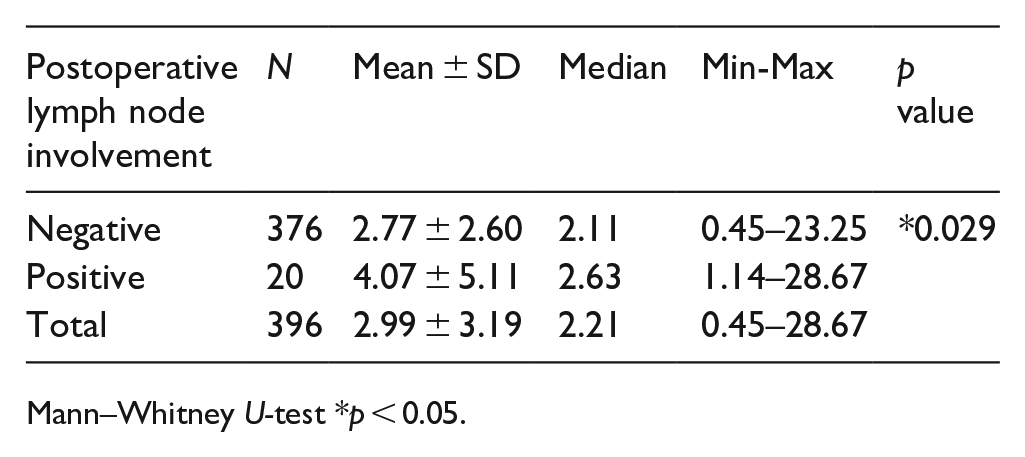
NLR, free PSA, f/t PSA, and PV were statistically higher in BHP, and PSAD was higher in PCa group. In PCa group, NLR was found to be higher in patients with PSA >10 ng/ml compared to those with less than ⩽10 ng/ml. NLR increases as the preoperative GS increases, and it was higher in pT3 patients than pT2 patients. NLR was statistically higher in those patients with positive lymph nodes than those without after RRP (p = 0.029).
Conclusion:
NLR is not a sufficient biomarker in differentiating clinically localized PCa from BPH. NLR increases as preoperative GS and pathologic stage increases. Lymph node involved patients after RRP have statistically higher NLR. NLR can be an indicator of ECE and lymph-node involvement in clinically localized PCa.
Keywords
Introduction
PSA is the most commonly used biomarker in diagnosis of PCa, making biopsy decisions and in the management of treatment. PSA increase alone is not sufficient to distinguish PCa from other benign prostatic diseases such as BPH and prostatitis. 1
In recent years systemic inflammation markers (serum white blood cells, neutrophil, lymphocyte, platelets), f/t PSA, and PSAD have been used to distinguish PCa from other benign prostatic diseases, also in prognosis and response to therapy in PCa.2–5
The desired features of biomarkers to be used in PCa are that they can be used in diagnosis, staging and prognosis, also being cheap, practical, and easy to apply.
Some cancers have harmful effects on the peripheral blood cells causing the release of cytokines and mediators. 6
The role of NLR have been studied in various types of cancer (renal cell, ovarian, stomach, liver, colon, pancreas, bladder) in the literature.6–8
There isn’t any comparative study which shows the role of NLR between definitely diagnosed patients with localized PCa and BPH in the literature. Almost all studies were made with prostate biopsy based. In these studies inability to diagnose PCa as a result of insufficient biopsy material, histopathological evaluation and inability to take samples from the tumor focus may lead us to wrong diagnosis. This situation leads us to incorrect idea about the role of NLR to differentiate PCa from BPH.
We conducted this study between PCa and BPH patients who had definitive diagnosis revealed with histopathology to find role and cut-off value of NLR in the diagnosis of PCa. A significant number of patients with clinically localized PCa have upgrading and upstaging after radical prostatectomy (RP). This situation affects the management and prognosis of patients. Studies investigating the relationship of NLR with PSA, GS, ECE (seminal vesicle and lymph-node involvement) are quite insufficient in the literature. The relationship of NLR with PSA, GS, and ECE also has been investigated in clinically localized PCa in this study.
Material and methods
This study carried out in the Urology Department of the University of Health Sciences, Prof.Dr. Cemil Taşçıoğlu city hospital, Istanbul, Turkey.
396 patients with clinically localized PCa who underwent open RRP and 260 patients with BPH who underwent suprapubic prostatectomy included in the study between May 2014 and December 2020.
Prof.Dr. Cemil Taşçıoğlu City Hospital ethics committee approval was obtained and all patients provided informed consent (Date 22.09.2020 and NO 366). Data of patients were collected and analyzed retrospectively.
PCa was diagnosed by transrectal ultrasound-guided prostate biopsy of minimum 12 cores based on elevated serum PSA, mpMRI findings or palpable nodule at DRE. The clinical stage was evaluated with using DRE, bone scan, computed tomography (CT), or mpMRI before RRP.
Only localized PCa patients with clinical stage ⩽T2c preoperatively and patients with definite histopathological diagnosis as BPH were included in the study. PCa patients who were treated previously (radiation therapy or androjen deprivation), those with ⩾ cT3 or lymph-positive preoperatively, patients who had systemic inflammatory, or autoimmune diseases and chronic use of drugs for these diseases, patients with missing data were excluded from the study.
In patients who have pre-biopsy complete blood count in his data, NLR of this assay was used in the study. In patients who had biopsy, we obtained blood analysis at earliest 4 week after prostate biopsy and before the operation in both groups. Urine cultures were performed before the surgery.
Almost all transrectal ultrasonography (TRUS) prostate biopsies were performed in our clinic. Prostate volume was calculated by using the formula: PV = 0.52 × (D1 × D2 × D3). D1 is maximum transverse diameter, D2 is maximum anteroposterior diameter and D3 is maximum longitudinal diameter calculated with TRUS.
Prostate biopsy, RRP, and suprapubic prostatectomy specimens and extracapsular extension were evaluated by two uropathology experts in our hospital. Prostate biopsy and final pathology GS were graded according to the international society of urological pathology (ISUP) 2014 classification system. 9
NLR, PSA, free PSA, PV,f/t PSA, and PSAD were compared between PCa (group 1) and BPH (group 2) groups by using statistical analysis to investigate the role of NLR in the diagnosis of PCa. We also investigated relation of NLR with preoperative PSA and GS in localized PCa patients. NLR were compared between pT2 and pT3 patients and NLR also compared between lymph-node positive and negative patients in prediction of extracapsular extension.
Statistical analysis
We used the Number Cruncher Statistical System (NCSS) Statistical Software program (Utah, USA) in all statistical analysis. Shapiro–Wilk test, Box plot charts, Student’s t-test, Kruskal–Wallis test, Mann–Whitney U-test, Chi squared test, and ROC curve analysis were used. p-Values were considered statistically significant if p ˂ 0.05.
Results
Clinical and blood serum parameters in PCa (group 1) and BPH (group 2) groups are shown in Table 1.
Clinical and blood serum parameters in PCa (group 1) and BPH (group 2) groups.

Mann–Whitney U-test *p<0.05.
The age of patients in the study ranged from 52 to 86 (median 68.11 ± 6.87). The mean age in PCa (group 1) and BPH (group 2) groups was 68.39 ± 6.66 and 67.45 ± 7.33 respectively. (Student t-test p = 0.292).
NLR, f/t PSA, free PSA, and PV were higher in BPH, and PSAD was higher statistically in PCa group. There wasn’t statistically difference in PSA between two groups (p = 0.082).
Screening tests for NLR, PSAD, Free PSA and f/t PSA measurements in defining the prostate ca group are shown in Table 2.
Screening tests for NLR, PSAD, FPSA, and f/t PSA measurements in defining prostat ca group.
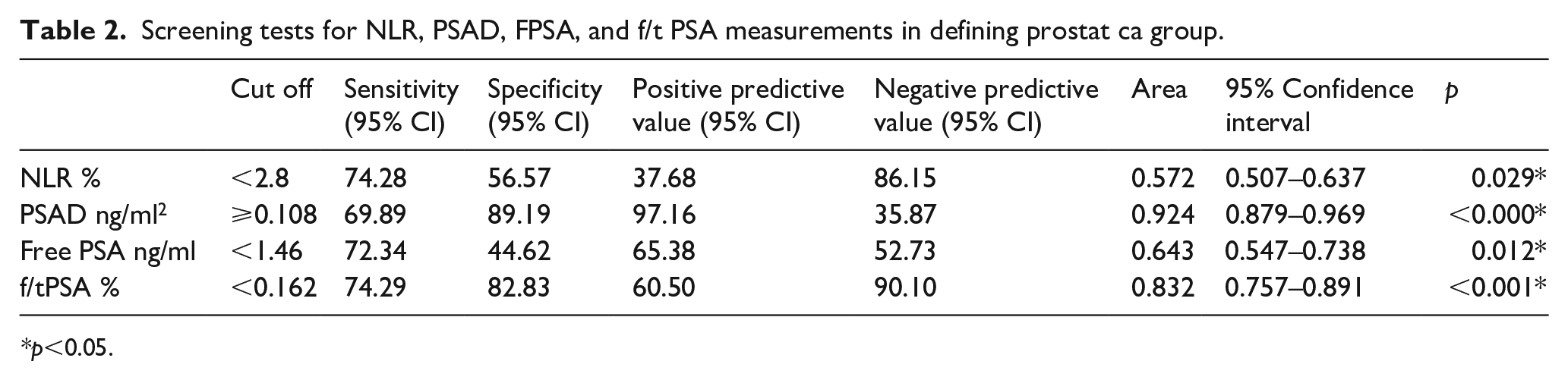
p<0.05.
The AuROC curve of the NLR, PSAD, Free PSA, and f/t PSA to diagnose prostate cancer is shown in Figure 1.
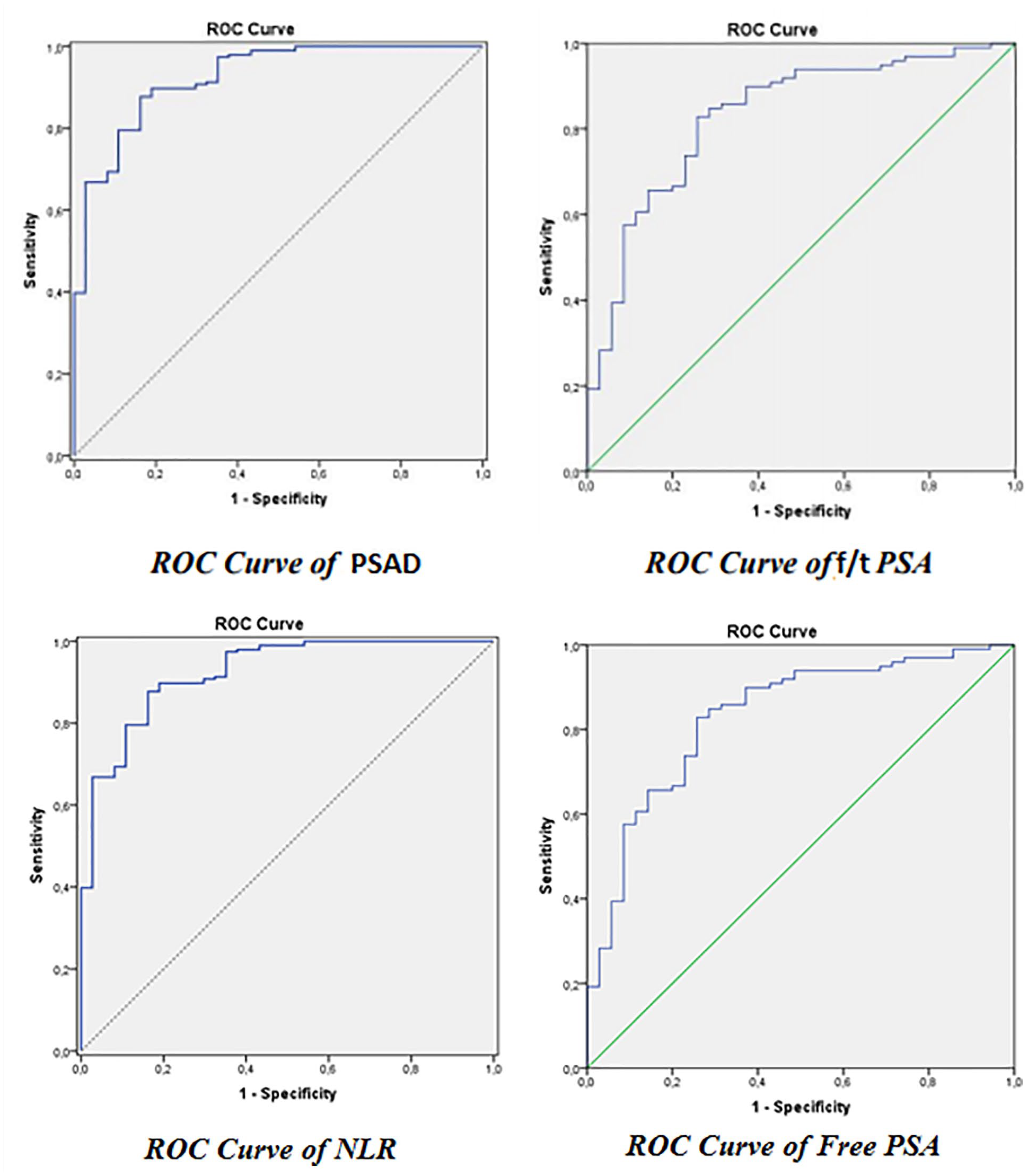
The AuROC curve of NLR, PSAD, free PSA, and f/t PSA to diagnose PCa.
AuROC curve of NLR, PSAD, Free PSA, and f/t PSA were 57.2%, 92.4%, 64.3%, 83.2% respectively. The ODDS ratio for NLR, PSAD, Free PSA, and f/t PSA were 2.107, 19.16, 3.76, and 13 (95% CI) respectively.
Biopsy and postoperative GS, preoperative clinical and postoperative pathologic stages of PCa patients (group 1) are shown in Table 3.
Biopsy and postoperative GS, preoperative clinical and postoperative pathologic stages of patients.

n = 396%.
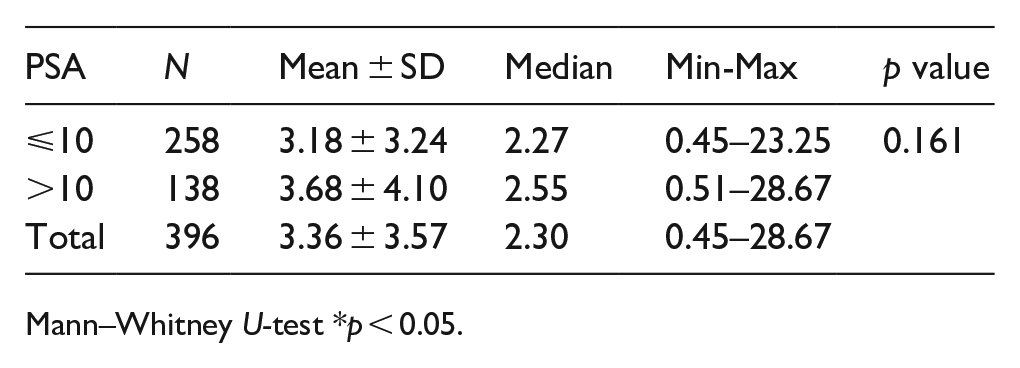
NLR in PCa group according to preoperative Gleason Score and PSA is shown in Table 4.
NLR in Prostate Ca group according to preoperative GS and PSA.
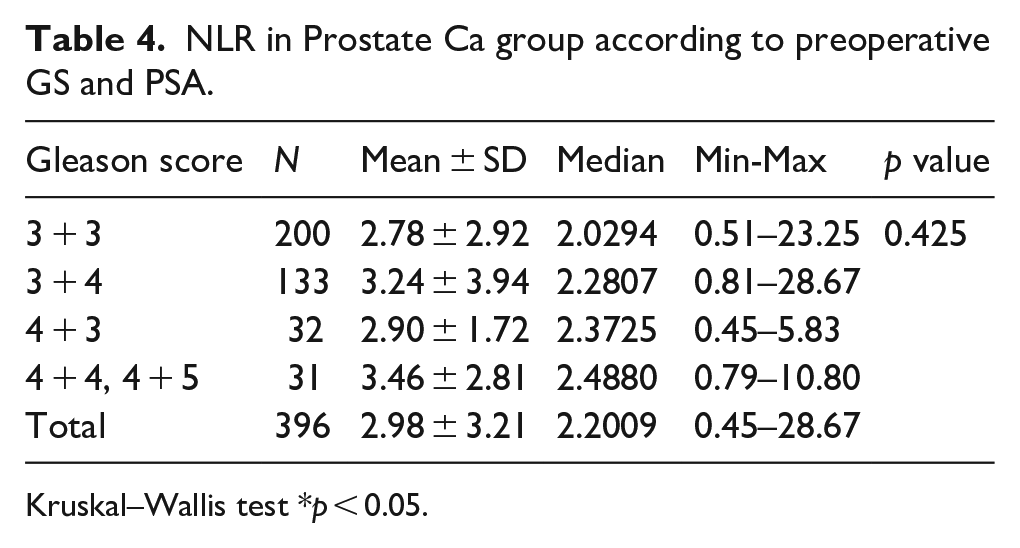
Kruskal–Wallis test *p < 0.05.
Mann–Whitney U-test *p < 0.05.
NLR increases as the Gleason Score increases in patients, but this does not indicate a significant difference (p = 0.425). NLR is higher in patients with PSA>10 ng/ml (p = 0.161).
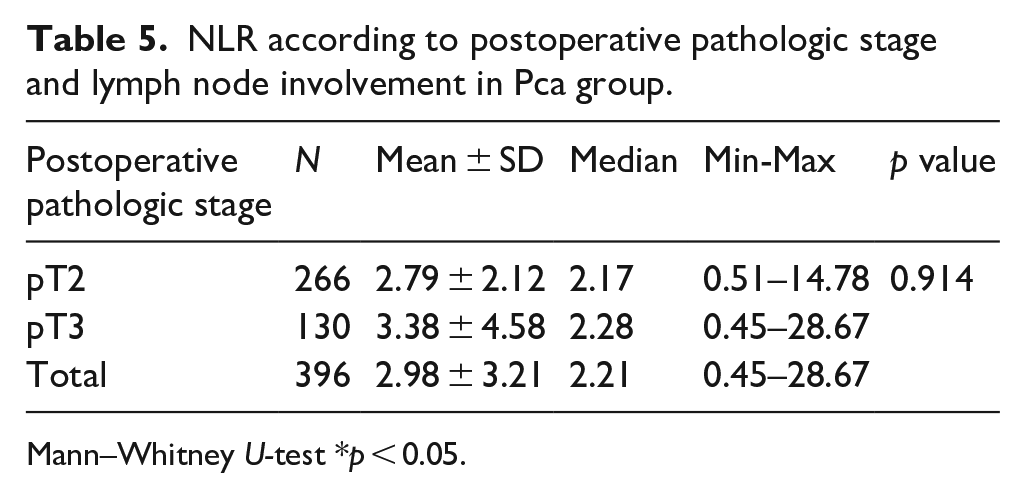
NLR in postoperative pathologic stage T2, T3, and lymph node involved patients in PCa group are shown in Table 5.
NLR according to postoperative pathologic stage and lymph node involvement in Pca group.
Mann–Whitney U-test *p < 0.05.
Mann–Whitney U-test *p < 0.05.
Mann–Whitney U-test *p < 0.05.
Mann–Whitney U-test *p < 0.05.
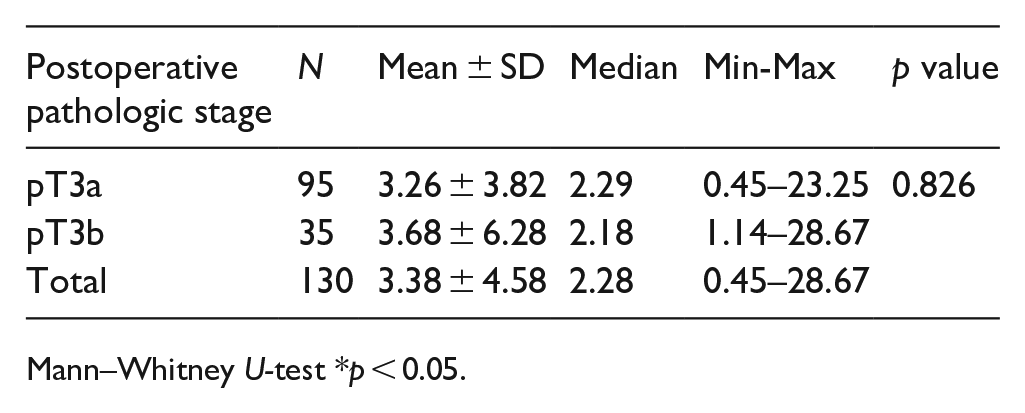
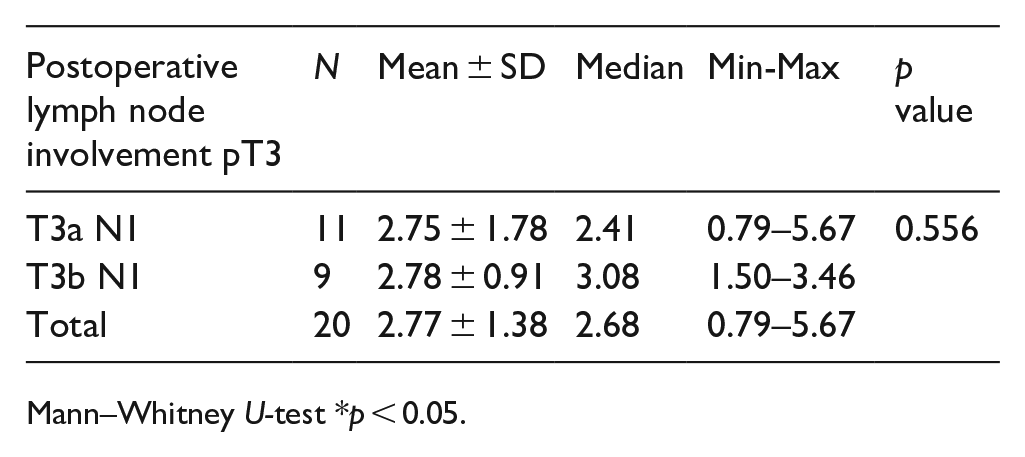
NLR in patients with postoperative pT3 stage is higher than patients with postoperative pT2 stage (p = 0.914). NLR in patients with pT3b N1 is higher than patients with pT3a N1 (p = 0.556).
A total of 95 of 396 patients (24.0%) had extraprostatic extension (pT3a) and 35 of 396 patients (8.8 %) had seminal vesicle invasion (pT3b) in our PCa group.
A total of 11 of the patients (2.8 %) found as pT3a N1 and 9 of the patients (2.3 %) found as pT3b N1 after RRP. A total of 20 patients had lymph node involvement in our study. Lymph-node positive patients had statistically higher NLR than lymph-node negative patients in PCa group (p = 0.029).
Discussion
PSA is the most commonly used biomarker in the diagnosis of PCa. PCa cannot be diagnosed in the first prostate biopsy ın approximately 20% of patients. 2 Various studies are currently being conducted to find new biomarkers that can replace PSA. The roles of systemic inflammation markers in various cancer types have been investigated.2,10–12
Mc Donald et al. 13 investigated the relationship between systemic inflammation markers and PSA in patients without prostate disease, and they found that serum NLR, fibrinogen, and c- reactive protein (CRP) were higher in men with higher PSA.
Gökçe et al. 14 found higher NLR in PCa patients compared to BPH patients, but lower NLR compared to patients with prostatitits.
Fujita et al. 15 investigated the role of differential white cell count and c-reactive protein level in prediction of prostate biopsy result. They showed that neutrophil count, PSA, PV, and PSAD were independent factors in their study and patients with low neutrophil count with higher PSA should be considered for prostate biopsy. 15
We investigated clinical and blood serum parameters in patients who had definitive diagnosis of localized PCa and BPH with histopathology. We found NLR, PV, Free PSA, and f/t PSA as statistically higher in BPH group. We found only PSAD as higher in PCa group (p = 0.001). Difference of PSA between two groups was not statistically significant (p = 0.082). We used cut off value of NLR as 2.8.
Kamali et al. 16 showed that NLR is not a predictive factor for diagnose of PCa in biopsy similar to our findings.
Kawahara et al. 4 found that NLR as significantly higher in PCa patients compared to patients without PCa unlike to our study and they found NLR cut off value as 2.4 to predict PCa. They stated that NLR with or without f/t PSA ratio may predict Pca. 4
The prognostic role of neutrophil count in PCa is a new hypothesis and was first mentioned in a study by Keizman et al. 17 They investigated the role of NLR in patients with metastatic castration-resistant PCa patients under treatment, and they found pretreatment NLR >3 was associated with the cancer progress free survival time but not with the overall survival. 17
Murray et al. 5 showed that NLR could not distinguish PCa from benign prostatic diseases in patients with PSA 4–10 ng/ml.
Our study showed that NLR was not an effective marker in the diagnosis of localized PCa. We found that PSAD, f/t PSA, and free PSA were more valuable in the differentiation of localized PCa from BPH.
Several studies in the literature investigated role of NLR on preoperative GS, postoperative pathologic stage, extraprostatic disease and prognosis, on the other hand different cut off values of NLR were used in these studies.
We observed that NLR increased as the GS increased in PCa patients although this increase is not statistically significant (p = 0.425).
Kawahara et al. 4 couldn’t find significant correlations between NLR and GS in nonmetastatic PCa patients similar to our findings using cut off value of NLR as 2.4.
Gökçe et al. 14 found that NLR was higher in GS 8–10 patients compared to GS 5–6 and GS 7 patients. In the same study the difference between GS 5–6 and GS 7 patients were not statistically significant.
Lee et al. 18 showed that patients with NLR ⩾2.5 had a higher GS, pathologic stage and extraprostatic disease than patients with NLR ˂2.5. In the same study they also found that higher NLR is related with biochemical recurrence in localized PCa patients after RP. 18 Minardi et al. 19 showed no difference in GS and pathologic stage in patients with NLR ⩾3, on the other hand they found that higher NLR is associated with poor prognosis.
NLR in pT3 patients was higher compared to pT2 patients (p = 0.914) and NLR couldn’t differentiate pT3a patients from pT3b patients statistically (p = 0.826) in our study.
Kwon et al. 20 found that higher NLR was not associated with upstaging and GS upgrading in low risk PCa patients.
NLR is higher in pT3b N1 patients compared to pT3a N1 patients (p = 0.556) and NLR is higher in lymph node involved patients statistically (p = 0.029) compared to lymph node negative patients in our study. This study showed us that NLR may be useful in demonstrating lymph node involvement in localized PCa. Cut-off value of NLR (2.8) can be used together with preoperative nomograms in prediction of extraprostatic extension. The cut-off value of NLR may be useful in clinical practice in deciding whether to perform lymphadenectomy and nerve-sparing surgery in RP.
Özsoy et al. 3 found that NLR ⩾3 was associated with higher GS, extracapsular extension, seminal vesicle invasion, and nodal involvement similar to our findings.
Retrospective, single center nature, along with the relatively small number of patients were the limitation in this study. Our study was conducted in patients with a definite pathological diagnosis and stage, so we could determine the true values of NLR more accurately than biopsy based studies. This was the advantage in this study.
There is a need for prospective studies including a large number of patients to investigate the role of NLR especially in extracapsular extension and lymph node involvement.
Conclusion
NLR is not a significant biomarker in differentiating localized PCa from BPH. In this distinction PSAD, f/t PSA, and free PSA were found more valuable in our study.
NLR increases as the GS and pathological stage increases in localized PCa patients. NLR is higher in patients with PSA >10 ng/ml compared to patients with PSA⩽10 ng/ml. NLR is higher statistically in lymph node positive patients compared to lymph node negative patients after RRP.
We can use NLR with cut off point as 2.8 in prediction of lymph-node involvement before RP in localized PCa patients in addition to preoperative nomograms in clinical practice.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.