
Abstract
Objectives:
To our knowledge, EVs (extracellular vesicles) are heterogenous encapsulated nanoparticles generated by the biological cells. EVs can be found in blood, urine and tissue of origin. They contain DNAs, RNAs, proteins specific to the cell of origin. It has been found that in PCa, increase in number of EVs can modulate phenotype and function of the recipient cells.
Methods:
This prospective randomized double-blind pilot study was conducted in the SMS Medical College, Jaipur in collaboration with All India Institute of Medical Sciences, New Delhi. For morphometric analysis, the number of extracellular vesicles per micrograph were counted under transmission electron microscope.
Results:
Out of 16 patients taken in our study, six were in group 1 (BPH group) and 10 were in group 2 (PCa group). The mean number of EVs was significantly higher in the cells of group 2 in comparison to the group 1. Among the PCa patients, mean number of EVs were 25, 30, 35, 43, 46 for the Gleason score 6, 7, 8, 9, 10 respectively. In our study the mean number of EVs in the newly diagnosed PCa group was less as compared to the CSPC and CRPC group.
Conclusions:
EVs are membrane bound particles shed regularly from the cells in the extracellular milieu under normal physiological and pathological conditions. In our study the number of EVs were more in the PCa cells in comparison with the BPH cells and among the PCa cells they bear a positive correlation with the Gleason score, thus EVs have the potential to become a biomarker.
Introduction
In men prostate cancer (PCa) is the second-leading cause of cancer-related mortality after lung cancer. 1 The initial management plan of newly diagnosed PCa depends on the stage and grade of the disease, patient age, life expectancy, and other medical comorbidities. Although, the pre-treatment serum prostate specific antigen (PSA) level is an important prognostic predictor of this disease 2 but it does not have any correlation with the stage and grade of disease. Therefore, new generation of molecular markers are needed, extracellular vesicle (EVs) are one of the emerging markers. 3 EVs are heterogenous encapsulated nanoparticles generated by the cells. Firstly these cells form endosomes during the process of endocytosis, 4 gradually these endosomes mature and during their maturation they shed intraluminal vesicles within themselves and becomes multi vesicular bodies (MVB), subsequently MVB migrate and fuse with the cell membrane and then they release these vesicles within the extracellular milieu as EVs. Based on size and biogenesis EVs can be divided into exosomes (30−100 nm), micro vesicles (MVs) (100−1000 nm), and apoptotic bodies (>1000 nm). However, the international society of EVs (IESV) favours the term EVs instead of exosomes and others.
Different EVs subtypes have different modes of genesis, size, shape, structure, biomarkers, and functions. Besides extracellular milieu of a cell, EVs can also be found in blood, urine, semen, saliva, and other biological fluids. EVs contain DNA, RNA, proteins, and lipids specific to the cell of their origin. 5 EVs not only help in exchange of genetic material from cell to other sites but they are also involved in cell to cell communication. 6 Because of presence of various molecules in these EVs, they help in cancer development, growth, and metastasis by inducing changes in the local stroma of the cancer cells and leading to development of protumor environment. 7 It has been found that in PCa, EVs contain high concentrations of various molecules such as integrin B4 and avB6, transmembrane glycoprotein Trop-2, vimentin, N cadherin and vinculin (VCL) which help in progression and metastasis of the disease. 8 Thereby, increase in number of EVs can modulate phenotype and function of the recipient cells.
However, despite the overall high prevalence of PCa, only a limited number of studies have indicated that EVs have prognostic relevance in PCa. Therefore, we aimed to compare the number of EVs in the patients with benign prostatic hyperplasia (BPH) and PCa. We also investigated the relationship between number of EVs with the Gleason score, PSA levels and hormonal treatment of PCa patients.
Material and methods
This prospective randomized double-blind pilot study was conducted between April 2019 to December 2019 after obtaining ethical clearance. This study was conducted in the Department of Urology, SMS Medical College and Attached Hospital, Jaipur in collaboration with All India Institute of Medical Sciences (AIIMS), New Delhi. Patients were enrolled in this study after understanding the procedure and giving their written consent. Patient’s records of previous diseases including history, past investigations, PSA (prostate specific antigen) levels and biopsy reports were analyzed. All the patients underwent physical examination and DRE (digital rectal examination), USG KUB (ultrasound of kidney, ureter and pre and post void bladder) along with TRUS (trans rectal ultrasound) of prostate. Metastatic workup in the form of Tc 99 Bone scan and/or MRI (magnetic resonance imaging) was done in cases of PCa. The study population was divided into two groups one with BPH and others with PCa (Figure 1).
Group 1: It comprises of patients who underwent TURP (trans urethral resection of prostate) for either retention of urine or severe obstructive LUTS (lower urinary tract symptoms). Inclusion criteria for this group was S.PSA less than 4 ng/ml, DRE suggestive of benign enlargement of prostate and histopathology of resected tissue found to be BPH.
Group 2: It comprise of patients suffering from PCa. This group was subdivided into three subgroups (A) Newly diagnosed PCa cases Patients in this subgroup had S.PSA greater than 20 ng/ml, on DRE whole of the prostate was hard, irregular and fixed, radiological examination suggestive of locally advanced or metastatic PCa and having histopathological proven PCa (B) Castrate sensitive PCa (CSPC) of 3-month duration. This subgroup had locally advanced or metastatic PCa cases associated with biochemical proven response to androgen ablation treatment. (C) Castration resistant PCa (CRPC) this subgroup of patients has locally advanced or metastatic PCa with biochemical proven failure to androgen ablation treatment.
Resected prostatic tissue (of group 1) was submitted for histopathological examination. Patients of subgroup A (group 2) underwent TRUS guided 16 cores prostate tissue biopsy out of which 12 cores were submitted for histopathology. Only those patients who had all the 12 cores positive for malignancy were included in the study. Remaining four prostatic cores were submitted for electron microscopy study. Patients of subgroup B and C (group 2) underwent TRUS guided needle biopsy. Only four cores were taken for electron microscopy study.
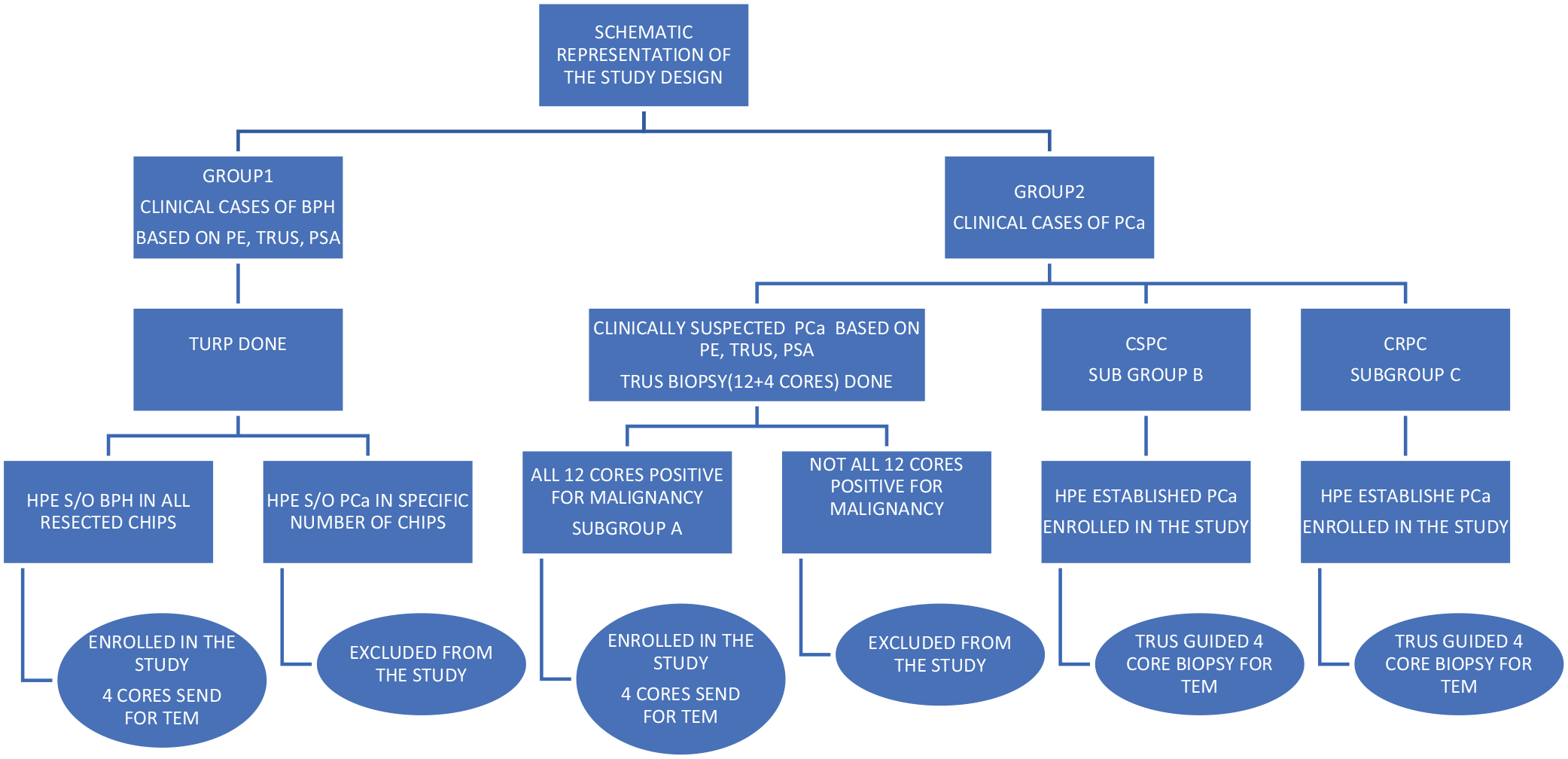
Schematic diagram showing our study design.
Patients having localized PCa requiring definitive treatment in the form of radical prostatectomy or radiotherapy, severe comorbidities, coagulopathies, and not willing to participate in the study were excluded.
For electron microscopy, four cores of prostate tissue of size 0.5 cubic millimeter were taken and fixed in Glutaraldehyde (2.5%) and Para formaldehyde (1%) solution, osmicated and embedded in Araldite CY212. Semi thin sections(1 micron) were stained with toluidine blue and observed under light microscope to select the area of interest for transmission electron microscope (TEM). About 60 nanometer (60 nm) thick sections were cut, stained with uranyl acetate and osmium tetra oxide and then viewed under TEM (Tecnai G2-20, FEI, Netherland), Captured images were analyzed using Image J Software (NIH, USA). For morphometric analysis, the number of vesicles per micrograph were counted under transmission electron microscope. In our study TEM images were obtained by “operator image selection” meaning that an operator takes images at locations where EVs were well visualized. The anatomist operator working on TEM was blinded for the histopathological and clinical findings. Electron micrographs taken (at least 10 images/sample) were examined and the number of EVs were expressed as mean of these images.
Statistical analysis
Statistical analysis was carried out using the Student’s t test correlation test. The chi square test was used to test for a potential association between study variables of interest. Differences were considered significant when p values was less than 0.05.
Results
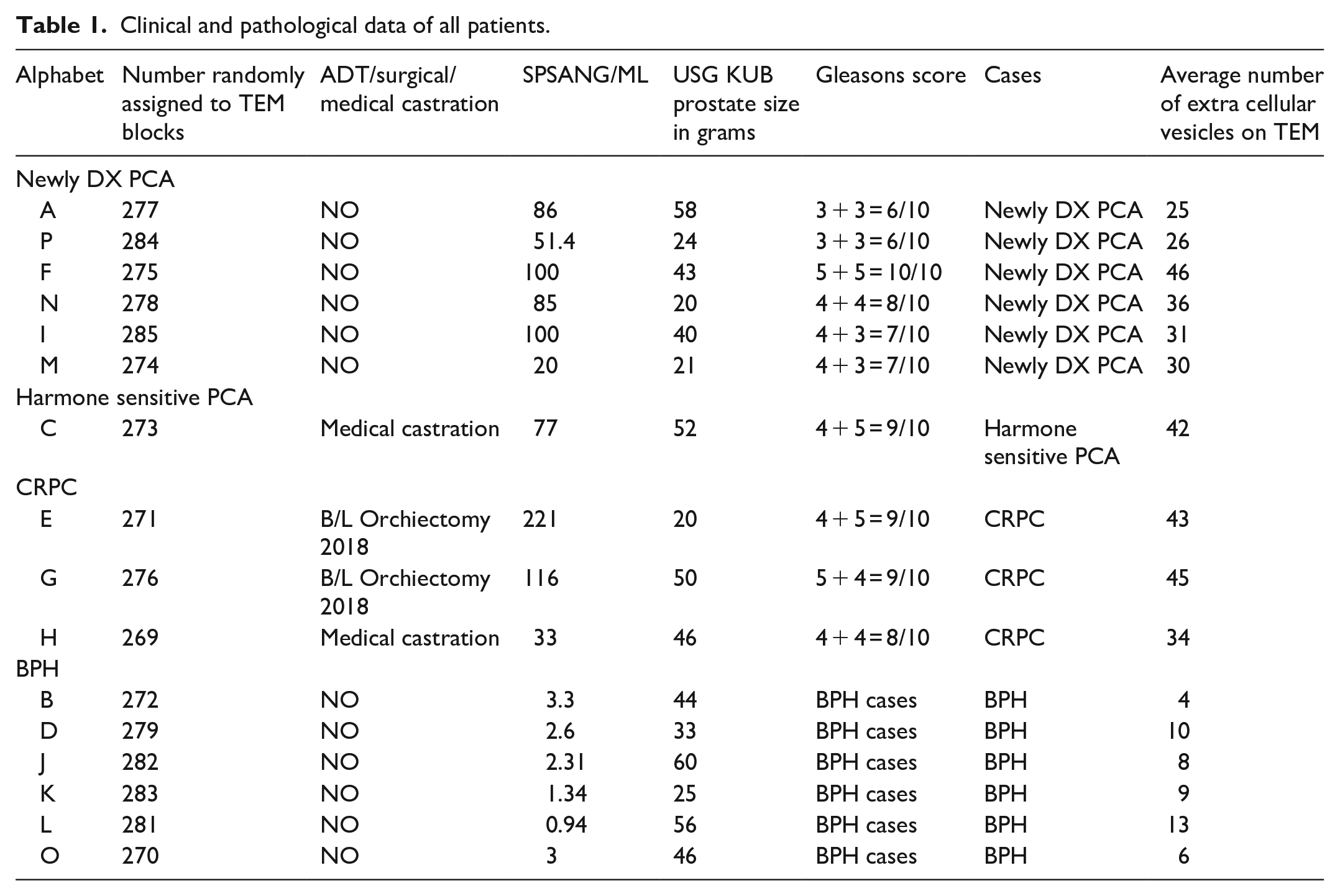
Out of 16 patients taken in our study, six were in group 1 (BPH group) and ten were in group 2 (PCa group). The clinical and pathological features of all patients enrolled in this study are reported in detail in Table 1. Average serum PSA levels was significantly higher in PCa group compared to BPH (88 vs 2.24 ng/ml). Prostate volume in both the groups were comparable (37.4 vs 44 gm).
Clinical and pathological data of all patients.
In our study the mean number of EVs was significantly higher in the cells of group 2 patients as compared to group 1 (35.8 vs 8.33 respectively) (Image 1, Figure 2). Similarly, EVs density was statistically different among BPH and PCa specimens. An extensive vacuolation and the presence of large vesicles containing lipid droplets and membranous material, suggestive of defective apoptosis were observed in our study (Image 2). Number of these type of EVs were more in PCa group as compared to BPH group. Among the PCa patients, mean number of EVs were 25, 30, 35, 43, 46 for the Gleason score 6, 7, 8, 9, 10 respectively (Figure 3). Thus, there was a positive correlation between the Gleason score and the number of EVs. Although the mean number of EVs (35.8) were more in PCa groups having higher average PSA values (88 ng/ml) in comparison to BPH group (8.33 and 2.24 respectively), but there was no correlation when we compared the PSA values and number of EVs among the different subgroups of PCa. There was no difference in the mean number of EVs between CSPC and CRPC (42, 40 respectively). However, the mean number of EVs in the newly diagnosed PCa group was less (30) as compared to the CSPC and CRPC group.
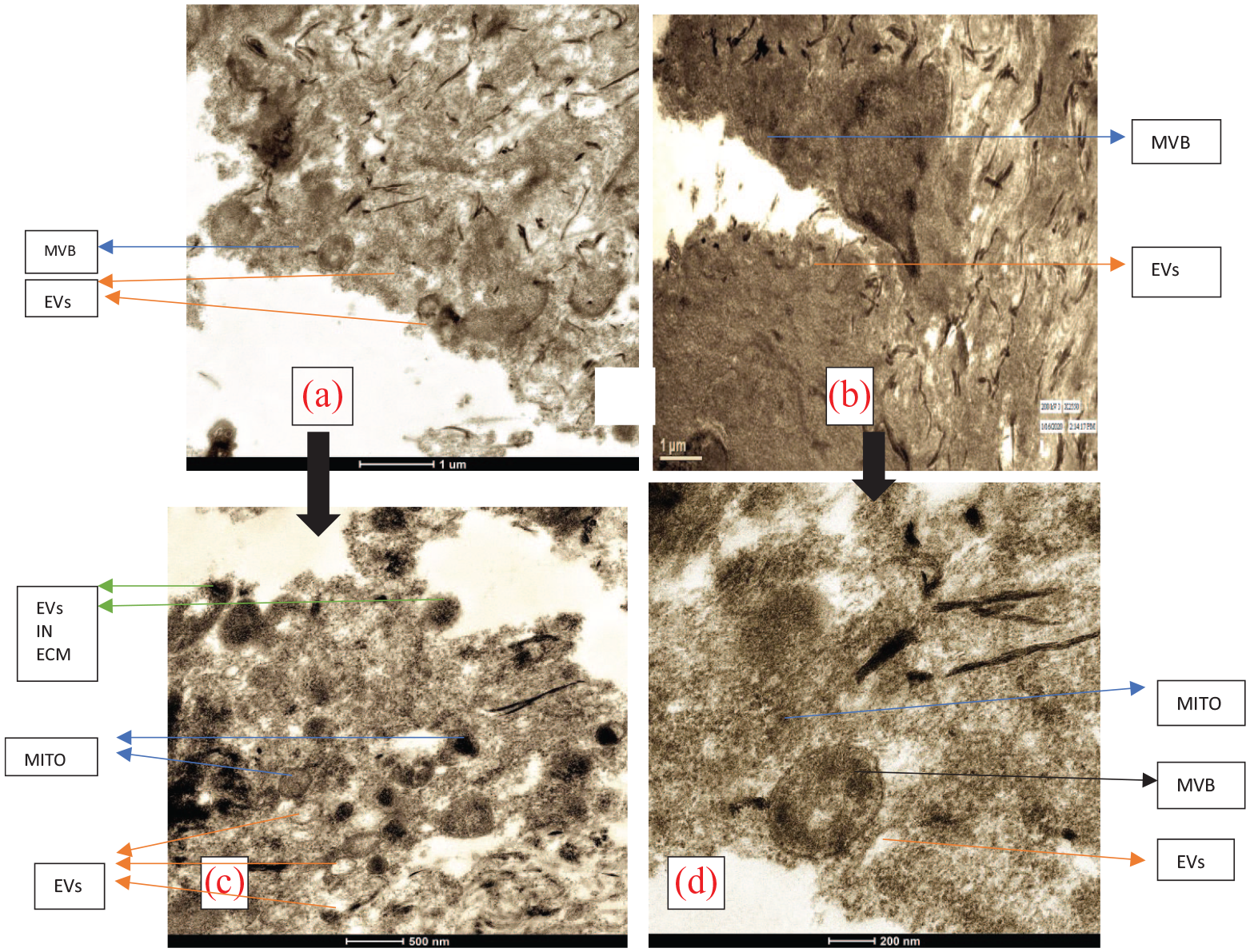
TEM micrographs of PCa (a and c); Where c is the magnified. View of a and BPH patients (b and d) where d is the magnified view of b showing greater number of EVs and MVB in PCa group.
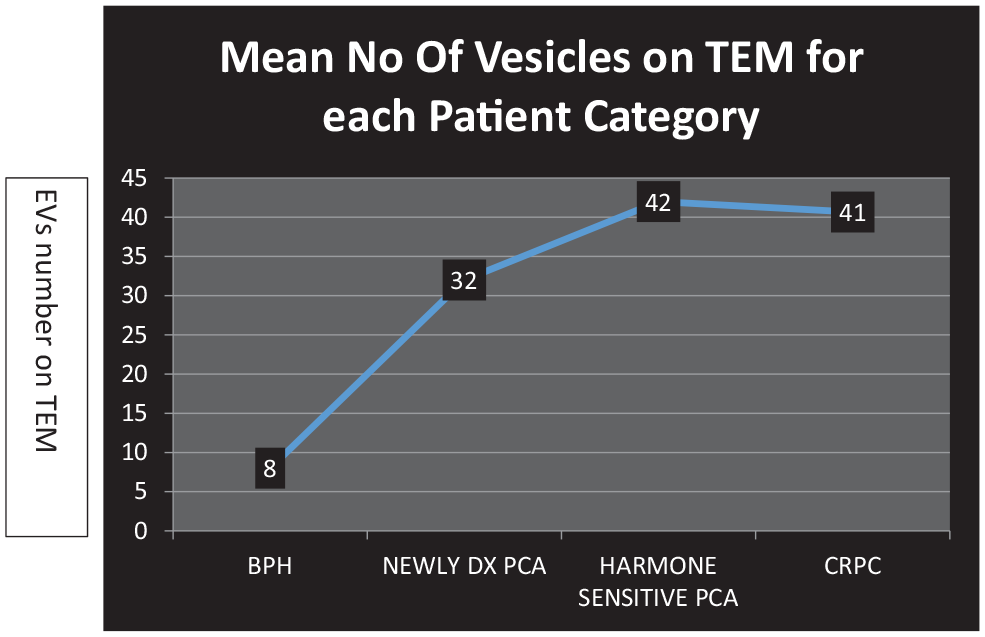
Relation between EVs number and the subgroups in our study.
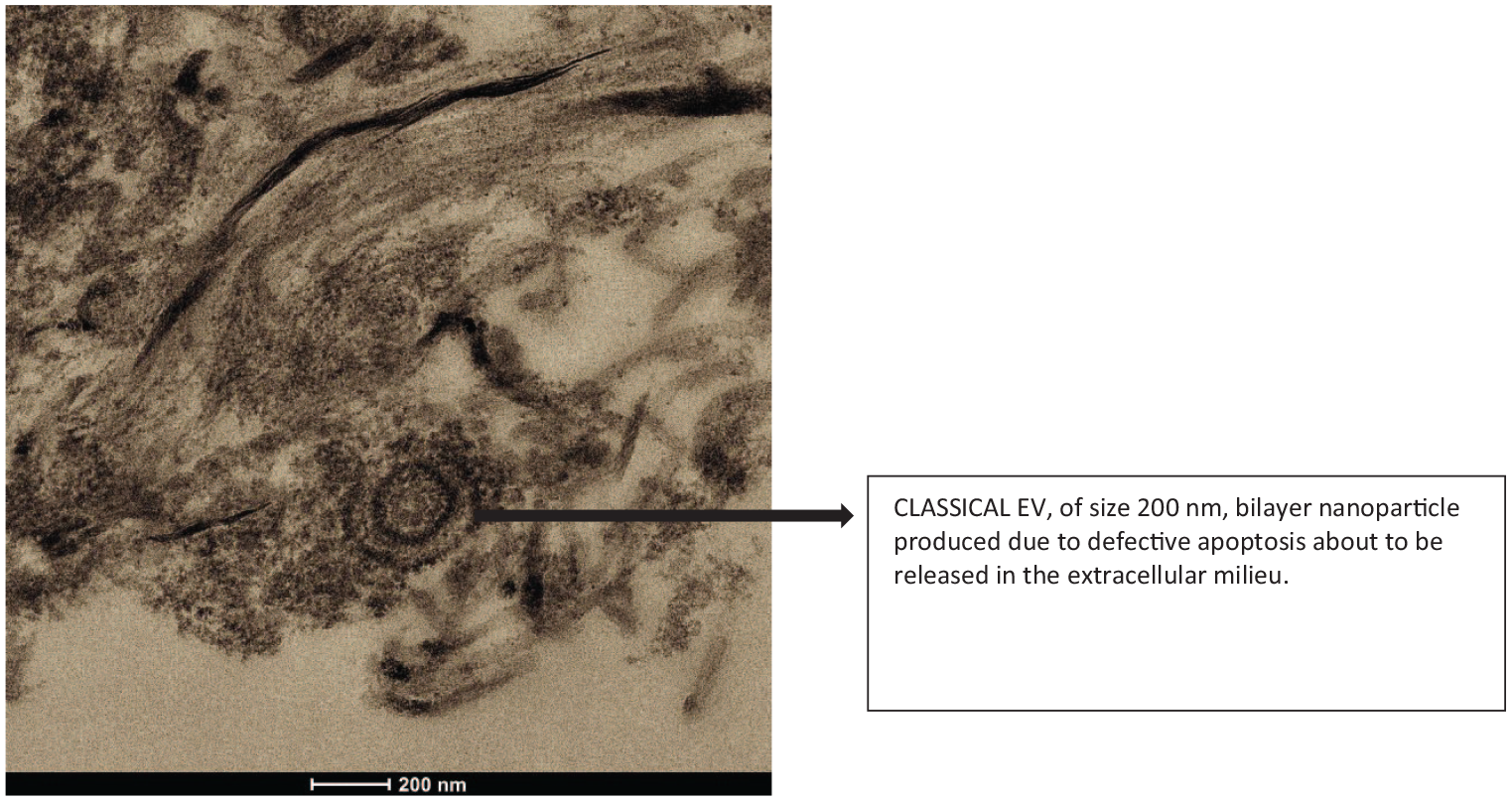
An extensive vacuolation and the presence of large vesicle containing lipid droplets and membranous material, suggestive of defective apoptosis.
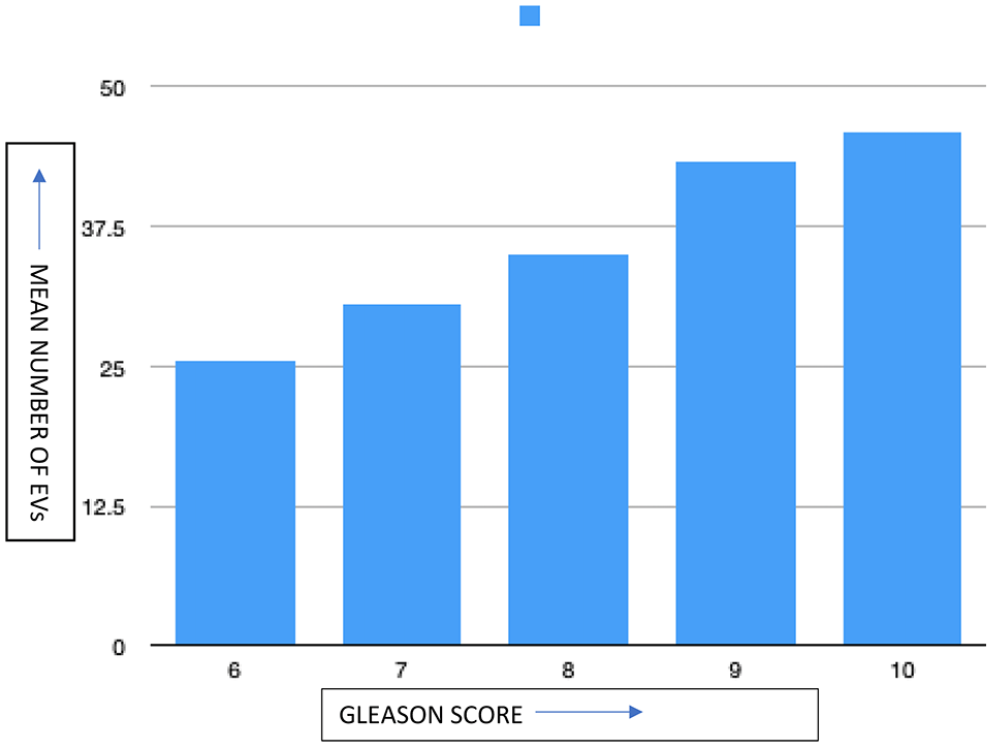
Relation between mean number of EVs and Gleason score Of PCa patients.
Discussion
EVs are membrane bound particles shed regularly from the cells in the extracellular milieu under normal physiological conditions as well as during apoptosis in the stressful and pathological conditions. 9 EVs of individual organs are unique because of the presence of specific molecules in them. However, EVs concentration is found to be more in that particular organ as compared to body fluids. In PCa cells, EVs are able to significantly reduce apoptosis by reducing the activity of caspase 3 and caspase 7. 10 The accumulation of AMBRA1 and SQSTM1 apoptosis related proteins in PCa patients represents a direct link between defective apoptosis and tumorigenesis 11 Our study suggests that the PCa cells shed a greater number of EVs in comparison to BPH cells which coincides with other studies. 12 This could suggest that EVs confer changes in the surrounding cells and create a protumor environment that helps in sustaining and spreading of PCa. 9
In our study as the Gleason score of PCa increases the number of EVs also increases, which is concurrent with the other studies. 10 We found a positive correlation between PSA levels and the number of EVs; however, no correlation was seen between the PSA values and number of EVs in the PCa group. No significant difference was found in the mean number of EVs between CSPC and CRPC subgroups (42, 40 respectively). However, the mean number of EVs in the newly diagnosed PCa group was less (30) as compared to the CSPC and CRPC group. This could be due to the expression of Clusterin, a stress induced antiapoptotic chaperone protein which increases after treatment with androgen ablation, conferring a more resistant phenotype. 13
There were few limitations in our study, firstly we could not use immunohistochemical markers to stain the EVs due to high cost and availability issues. Secondly it was not a vertical study and finally mechanical disruption of tissues obtained through needle biopsy.
Conclusion
As EVs are present in increased number in PCa and they share a positive correlation with the Gleason’s score. We conclude that EVs have the potential as biomarkers for diagnosis and prognosis of PCa.
Footnotes
Acknowledgements
V Agarwal wrote the manuscript, ethical clearance and analyzed the data and edited the manuscript. S Yadav was involved in the approval of the final manuscript. N Mehta and G Talwar were involved in patient recruitment. J Qadri and S Sarwar were involved in TEM study. S Kumar was involved in data recruitment.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.