
Abstract
Case:
We present a case of spontaneous extra-peritoneal rupture of an acquired diverticulum an elderly male with symptoms of bladder outlet obstruction who presented in emergency with acute abdomen.
Outcome:
The acute phase was managed conservatively with bladder drainage and intravenous antibiotics. He recently underwent Transurethral Resection of Prostate. He is asymptomatic on follow-up.
Conclusions:
Acquired bladder diverticulum are rare in adults and are mostly seen in patients with high pressure bladder due to bladder outlet obstruction. Atraumatic extraperitoneal ruptures of diverticulum are uncommonly reported.
Introduction
A bladder diverticulum is mucosal outpouching through the muscular wall of the urinary bladder; cause may be congenital or acquired defect of bladder wall. 1 Congenital bladder diverticula are usually seen as pop-off mechanism in high pressure bladder associated with bladder outlet obstruction such as posterior urethral valves.
Acquired diverticula seen in adults are mostly due to chronic bladder outlet obstruction as a result of benign prostatic hyperplasia, bladder malignancy, urethral stricture and/or weakness in bladder wall caused by tuberculosis, chronic cystitis and neurogenic bladder. 2 Most of the bladder diverticula are small and asymptomatic; however, some of the diverticula may be complicated by inflammation, infection, calculi, large size and urinary retention or even malignancy. 1
Atraumatic extra-peritoneal rupture of a bladder diverticulum in adults is rare and diagnosis is difficult. We describe an elderly male with symptoms of bladder outlet obstruction due to benign prostatic hyperplasia (BPH) with bladder diverticulum who presented with spontaneous extra-peritoneal rupture of the diverticulum in emergency.
Case summary
A 69 years elderly male patient presented in surgery emergency acute pain in abdomen, urinary retention and haematuria of 2 days duration. He was a diagnosed case of BPH with bladder diverticulum and was kept catheterized. He had presented with lower urinary tract symptoms (LUTS) 4 months back and diagnosed with BPH and a large urinary bladder diverticulum. His symptoms resolved after per urethral catheterization. Voiding Cysto-urethrography had suggested irregular urinary bladder with a large diverticulum with narrow neck arising from left superolateral area of the bladder. The patient had opted for elective TURP and diverticulectomy and was being planned for the same. However, he did not follow up for surgery because of the outbreak of SARS-Co virus pandemic.
Presently, he came in emergency with acute abdomen and urinary retention because of block in his per urethral catheter. There was tenderness and guarding in suprapubic region and bladder was palpable. After stabilization and change of his per urethral catheter, Voiding Cysto-urethrography (VCUG) was done which showed a large diverticulum with narrow neck at left lateral wall of a small irregular urinary bladder with extravasation of contrast (Figure 1). There was no evidence of vesico-ureteric reflux. CT urography was done which revealed extra-peritoneal rupture of the bladder diverticulum (Figures 2 and 3). He was managed conservatively with continuous urinary bladder drainage with intravenous broad-spectrum antibiotics.
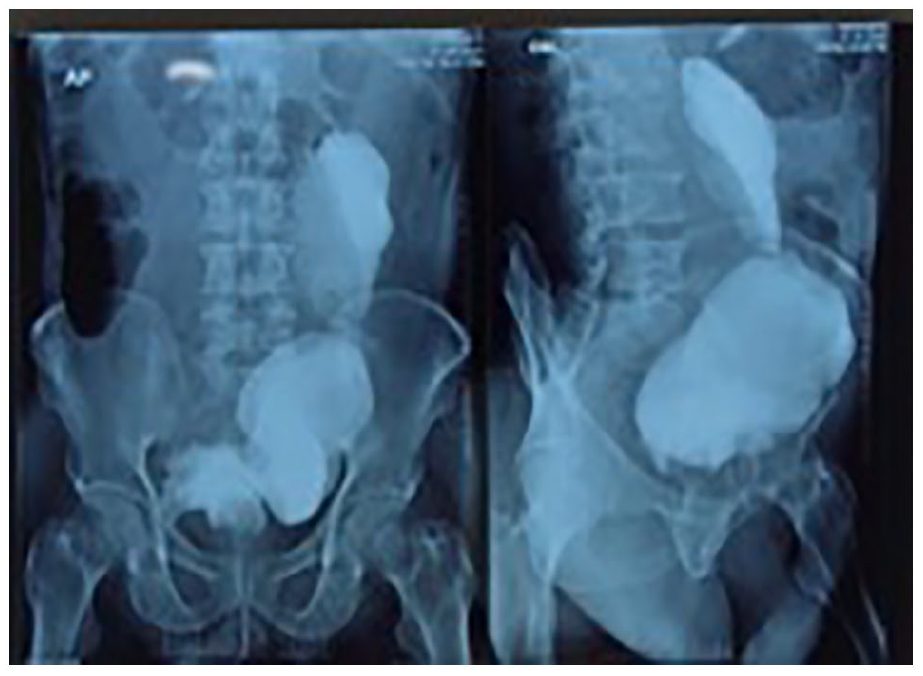
Cysto-urethrography (VCUG) showing a large diverticulum with narrow neck at left lateral wall of a small irregular urinary bladder with extravasation of contrast.
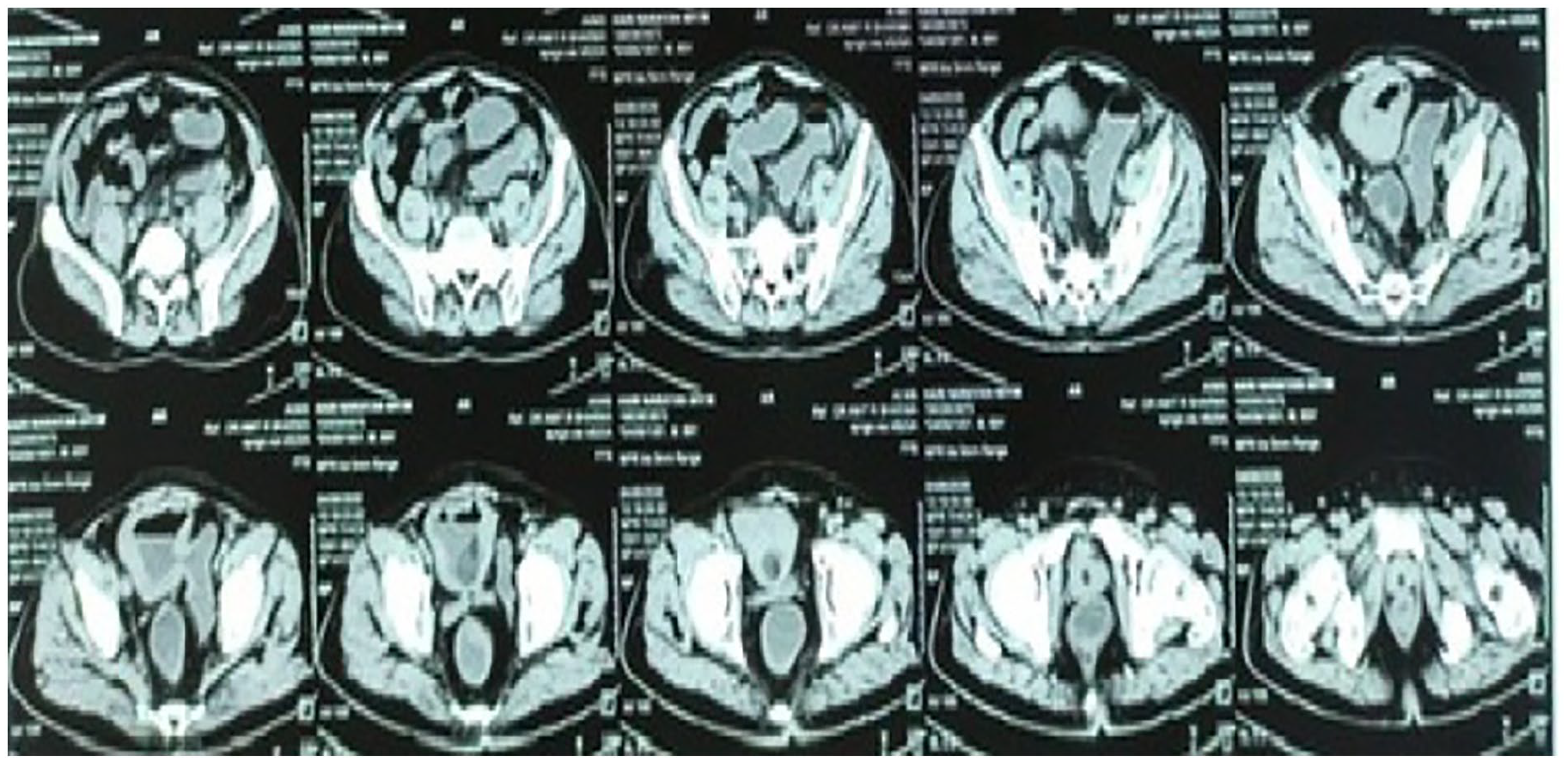
CT urography images revealing extra-peritoneal rupture of bladder diverticulum with extravasation of contrast in retroperitoneal space.
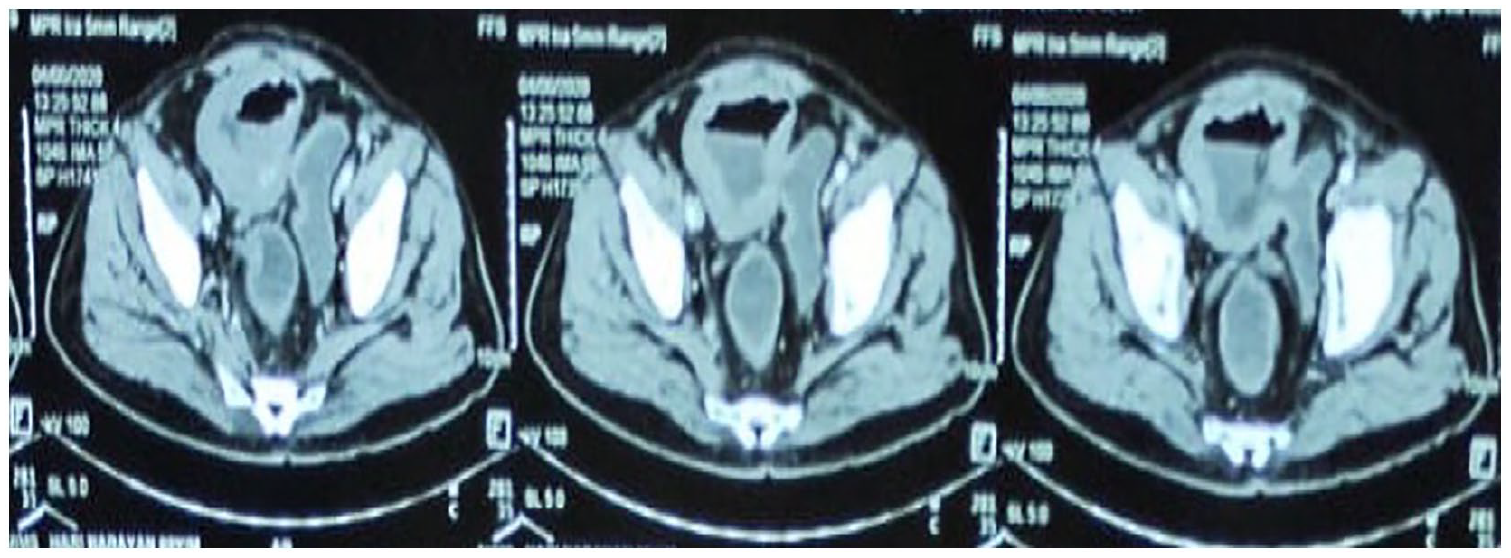
CT urography images revealing extra-peritoneal rupture of bladder diverticulum with extravasation of contrast in retroperitoneal space.
He recently underwent Transurethral Resection of Prostate (TURP) and is asymptomatic on follow-up.
Discussion
Atraumatic extra-peritoneal rupture of bladder diverticulum is less commonly reported in literature.1–8 Pathological bladder wall weakness and/or increased bladder pressures (as a result of bladder outlet obstruction) are harbingers of spontaneous bladder rupture 1 ; predisposing conditions being malignancy, pelvic irradiation, alcohol intoxication, candida cystitis, eosinophilic cystitis, previous bladder surgeries and pregnancy.
A patient with spontaneous rupture of bladder diverticulum usually presents with non-specific symptoms and signs; hence making a clinical diagnosis is difficult.1,2 This is unlike the traumatic intra-peritoneal rupture of bladder/diverticulum, wherein the patient presents with signs of trauma and peritonitis.1,2 A patient with spontaneous perforation of bladder diverticulum would usually present with abdominal pain, distention, decreased urine output and/or other urinary symptoms. 2 Associated history of pelvic malignancy/irradiation, bladder surgery, bladder tuberculosis and chronic bladder outlet obstruction may be present and should be asked. Our patient had an acute presentation with a palpable bladder and haematuria because of his blocked per urethral catheter.
Management of intraperitoneal and extraperitoneal bladder rupture differs; thereby making a clinical diagnosis essential. Intraperitoneal bladder/diverticulum ruptures, usually being traumatic, are managed surgically. On the other hand, extra-peritoneal bladder/diverticulum rupture, conservative approach by Foleys catheter drainage is usually favoured.1,9
A review of literature suggests less than 20 case reports of bladder divertulum rupture.1,10 In a review of 10 cases by Keeler and Sant, the site of rupture was found to be dome and all were intraperitoneal ruptures; associated urinary tract infection and bladder outlet obstruction were present. Kodama et al. reported the role of multi-detector CT urography in diagnosis of rupture of extra-peritoneal bladder diverticulum, for which initial conservative approach was tried, but the patient required surgical repair and drainage of associated retroperitoneal abscess [ucr]. Oh et al. 2 have recently reported successful conservative management of intraperitoneal bladder diverticulum rupture in a critically ill elderly. This suggests that the management approach needs to be individualized and associated underlying abnormality should be sought and appropriately addressed to.
Our case was unique as the patient was already diagnosed with BPH and associated diverticulum and was kept on per urethral catheterization. He had opted for elective surgery for BPH and diverticulectomy but could not come for surgery because of pandemic. In the interim period, he had a block in his catheter and extra-peritoneal diverticulum perforation; and presented with acute abdomen.
Footnotes
Authors’ note
This manuscript has been read and approved by all the authors, the requirements for authorship have been met and each author believes that the manuscript represents honest work.
Author contributions
Amit Sharma: Concept, data collection, drafting of manuscript, editing and Final approval; Deepak Biswal: Concept, data collection and drafting of manuscript; Satyadeo Sharma: Concept, data collection and drafting of manuscript; Siddhant Roy: Concept, data collection and drafting of manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Written and informed consent
Written and Informed Consent was taken from the patient for publication of this case report and also for sharing of the images.