
Abstract
Introduction:
Totally endophytic renal masses may be invisible during laparoscopic partial nephrectomy, posing challenge to surgeons regarding tumor’s identification and resection.
Case presentation:
A 22-year-old male was incidentally diagnosed with a completely endophytic, cT1a renal mass. Percutaneous Computed Tomography-guided insertion of a hook-wire was performed prior to laparoscopic partial nephrectomy. The hook-wire anchored centrally into the tumor and its extra-renal part was easily identified intraoperatively, contributing to tumor’s identification and surgical excision. Total operative time was 185 min, warm ischemia time was 21.5 min, tumor excision time was 10 min, and total renorraphy time was 31 min. No complications were encountered perioperatively. The patient was discharged on the fourth postoperative day. Histology revealed a pT1a, clear-cell renal cell carcinoma, with negative surgical margins.
Conclusions:
Our first experience indicates that hook-wire guided excision of a completely endophytic renal mass during laparoscopic partial nephrectomy is feasible, safe, and cost-effective.
Introduction
Completely endophytic renal masses (RMs) are considered a surgical challenge with respect to their identification and resection due to their intraparenchymal growth, which does not alter the renal rim and does not provide haptic feedback during minimally invasive nephron-sparing procedures.1,2 Intraoperative ultrasound (US) is a useful tool in localization of such tumors during laparoscopy, with positive oncologic outcomes reported so far in the literature.1,2 Another option is near-infrared fluorescence imaging using indocyanine green dye. 2 Preoperative, percutaneous, image-guided, intratumoral placement of embolization coil to facilitate intraoperative identification of an endophytic and isoechoic RM with the laparoscopic US during robot-assisted laparoscopic partial nephrectomy (LPN) has also been described. 3 However, the appropriate equipment may be unavailable in several hospitals. 2 Computed Tomography (CT)-guided hook-wire (HW) placement for tumor localization has gained popularity during the last years mainly in breast and lung surgery, as an effective and safe technique. 1
We present our technique using a HW in order to overcome the “tumor identification problem” during three-dimensional (3D) LPN, in a patient bearing a completely endophytic, cT1a RM.
Case presentation
In June 2020, a 22-year-old Caucasian male was incidentally diagnosed with a small, totally endophytic, left RM. Abdominal CT scan and Magnetic Resonance Imaging (MRI) demonstrated a 3.26 × 2.84 cm in size, contrast-enhanced tumor, located posteriorly, between the polar lines (Figure 1). After obtaining informed written consent, the patient was scheduled for 3D-LPN.
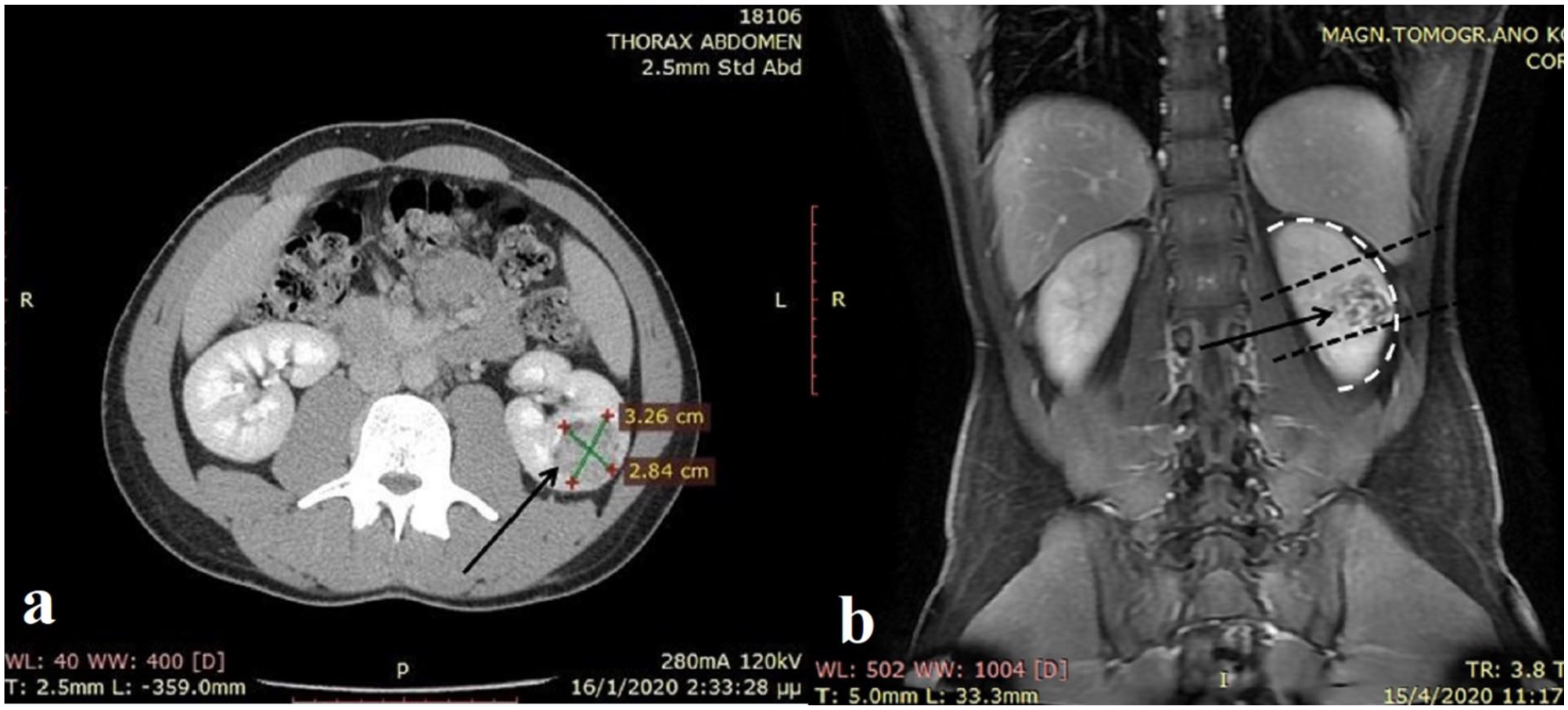
(a) Preoperative CT scan following intravenous administration of contrast medium depicting the 3.26 × 2.84 cm in size, left renal mass (black arrow) and (b) preoperative T1-weighted MRI (coronal view) demonstrating the left renal mass (black arrow), located between polar lines (black dotted lines), not causing alteration of the renal rim (white curved dotted line).
As laparoscopic US is unavailable in our institution, a 20 gauge in diameter, 90 mm in length localization HW (Duo System, Somatex® Medical Technologies, Berlin, Germany) was inserted percutaneously, under local anesthesia and CT-guidance by an interventional radiologist, in order to overcome the tumor identification problem intraoperatively. The procedure took place 1 h prior to LPN, lasted 18 min and was uneventful. The wire was depicted anchoring centrally to the RM at the end of the process (Figure 2).
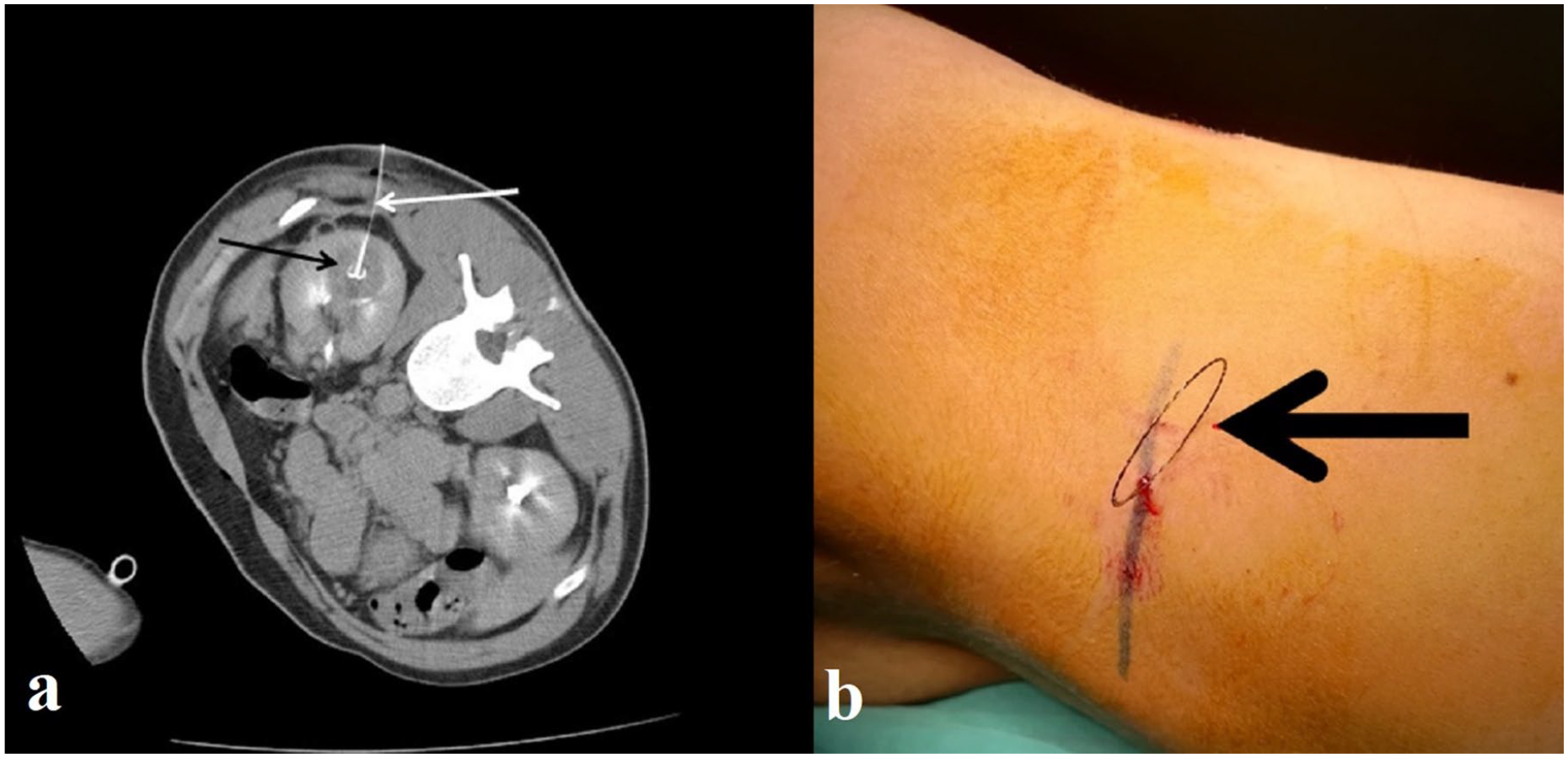
(a) Preoperative abdominal CT scan following intravenous administration of contrast medium demonstrating the hook-wire (white arrow) anchored centrally into the left, renal mass (black arrow) with equal distance to tumor margins and (b) preoperative photo following percutaneous placement of the hook-wire with the patient on the operating table showing the extracorporeal part of the wire (black arrow) with 90° skin to wire angle. Black line on patient’s skin depicts 12th, left rib.
The patient was transferred to the operating room and received general anesthesia. Subsequently, he was placed in the left, lateral position with the operating table half-flexed, as for transperitoneal laparoscopic renal procedure. Our technique regarding transperitoneal LPN has previously been described. 4 In brief, an open Hasson technique was used in order to place the first trocar of 12 mm for the 30°, 3D laparoscope. Pneumoperitoneum was applied and three more trocars (two 12 mm and one 5 mm) were placed under direct vision. After bowel mobilization, Gerota’s fascia was incised and the kidney was mobilized and defatted down to the renal capsule. HW was then recognized and the tumor margins were marked circularly, using a self-made, radiopaque, 3 cm long ruler, prepared from a 14 Fr nelaton catheter rotated around the wire (with the wire being always at the center of the circle) and a monopolar hook electrocautery for demarcation (Figure 3). Two renal artery branches were identified and each one was occluded (Rummel Tourniquet technique) in order to achieve warm ischemia (WI). The RM was excised (enucleo-resection) using cold scissors (Figure 4). Subsequently, inner renorrhaphy was performed, WI stopped by releasing the tourniquets (early unclamping technique) and outer renorrhaphy was performed. The specimen (with the HW in-place) was finally retrieved with an endoscopic specimen bag via a 12 mm port and was grossly inspected. As we were satisfied with our resection, perirenal fat was reapproximated over the cutting surface, a 16 Fr drain was placed via a port incision and port incisions were closed.
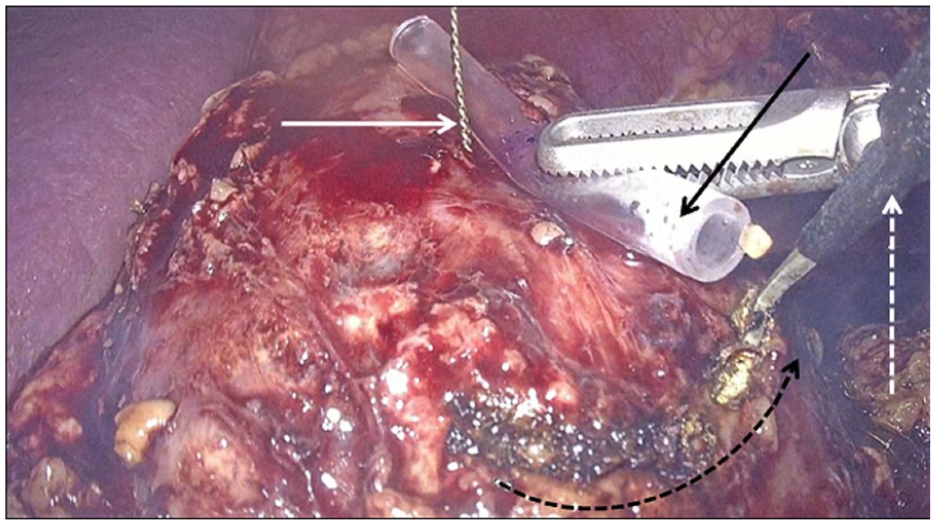
Intraoperative photo demonstrating the self-made ruler (black arrow) rotated around the hook-wire (white arrow) facilitating tumor demarcation by using monopolar hook-electrocautery (white dotted line arrow). Curved, dotted, black line with the arrow shows the anticlockwise movement of the ruler around the wire.
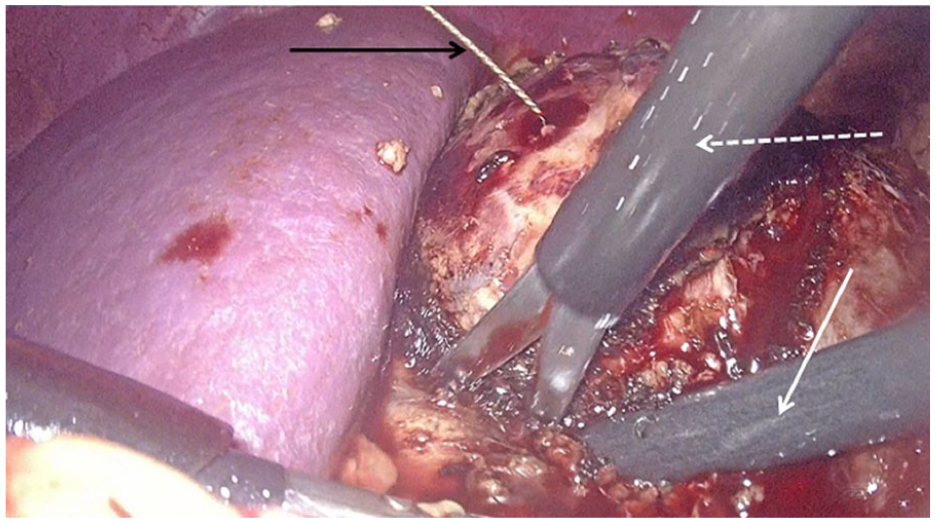
Intraoperative photo demonstrating tumor’s resection by using cold scissors (white dotted line arrow) and the hook-wire (black arrow) entering the renal mass. Laparoscopic suction/irrigation system (white arrow) is located in the tumor bed to control bleeding and stabilize the kidney during tumor’s resection.
Total operative time was 185 min, WI time was 21.5 min, tumor excision time was 10 min and total renorraphy time was 31 min. Estimated Glomerular Filtration Rate preoperatively and on discharge were 112 ml/min/1.73 m2. Serum hemoglobin value was 13.5 g/dL preoperatively, 11 g/dL on the first postoperative hours, and 12.3 g/dL on discharge. Histology revealed a pT1a, clear-cell renal cell carcinoma, Fuhrman grade 2-3, with negative surgical margins (NSMs).
No complications were recorded perioperatively. Urine catheter and drainage tube were removed on the first and on the fourth postoperative day, respectively. The patient was discharged on the fourth postoperative day and will be re-evaluated 6 months postoperatively.
Discussion
Reviewing the literature, two cases of HW tumor localization during LPN have been reported, to the best of our knowledge.1,2 Both resulted in successful endophytic RM localization and excision, NSMs and no perioperative complications.1,2 Kouriefs et al. also used a ruler for tumor demarcation. 1 However, the HW was placed at the deepest margin of the RM and was used in order to lift the tumor from its renal bed, while we placed the HW at the center of the tumor and we did not apply any traction. 1
The reason for the selection of our method was not only the unavailability of laparoscopic US. Regarding cost-effectiveness, our method deems very appealing as the cost of the HW we used is 39€ (according to our hospital’s financial service). On the other hand, the expense for a laparoscopic US probe, 5–12 MHz, 46.5 mm width with four directional articulation range is approximately 30.000$. 5 HW technique takes advantage of the precise CT scan depiction. 2 Skin to tumor and core to margin distance measurements to place the HW centrally within the RM with the proper direction and insertion angle are limitations easily overtaken by using CT scan. 2 Diligent preoperative planning and cooperation with interventional radiologists is of paramount importance. 3 In combination with the use of a ruler, similar to our self-made ruler, the technique can achieve excellent precision in RM delineation. 1 Finally, completely endophytic and isoechoic in nature RMs may be unidentifiable by the intracorporeal US intraoperatively. 3 This problem could be easily overtaken by inserting a HW preoperatively.
In terms of safety, no complications have so far been reported regarding RM localization with a HW, as observed in our case.1,2 Regarding tract seeding by tumor cells or tumor spillage, we can only make assumptions and correlations with CT-guided renal biopsies and ablative techniques. 1 These procedures share similar principles to our technique and only sporadic cases of seeding have so far been reported, while the risk of bleeding is negligible. 1 Caution must be spent on surgical maneuvers, as inadvertent dislocation of the “barbed-tip” wire might destroy preoperative preparation and might encompass a risk for tumor spillage or adjacent organ injury. 6 Application of safety measures such as bending HW 90° to the skin, careful patient transport to the operating room and accounting for the full length of the wire by the surgeons could ensure HW’s security. 6 In addition, we encourage HW insertion just prior to the operation. 1
HW localization technique for intraparenchymal RMs is a technically feasible, cost-effective and safe method, providing high precision in identification and demarcation of such tumors. This technique may be an alternative to intraoperative US-guidance, especially when performed in high-volume centers by experienced laparoscopic surgeons or when laparoscopic US is unavailable. Considerable limitations of the method are the small number of cases already reported and the lack of long-term follow-up data in published studies. Larger series of patients and comparative studies with the already used techniques for endophytic RM localization are needed to safely evaluate the method.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.