
Abstract
Aim:
To study the outcome of simultaneous angioembolization and nephron sparing surgery in large renal angiomyolipomas.
Materials and methods:
A prospective study of carried out from 2016 to 2019. A total of 15 patients were included in the study with a lesion (angiomyolipoma) more than 10 cm in size, suitable for nephron sparing surgery. The workup of the patients included history, baseline blood investigations, ultrasonography, and CT urography including angiographic films. All the patients were taken up for selective of angioembolization of the feeding vessels of the AML carried out by the interventional radiologist followed by nephron sparing surgery in the same sitting. The short term outcomes studied were warm ischemia time, average blood loss, and length of post-operative hospital stay. The oncological outcome was evaluated by noting the surgical margins of histopathological specimen and functional outcome by assessing the function of the preserved renal parenchyma.
Results:
Twelve out of fifteen cases were female. The mean age was 42.25 years. All the patients had lesion more than 10 cm with seven tumors located at the lower pole, four at mid-pole, and four at upper pole. Eight patients had low complexity score on RENAL score (i.e. 4–6), five patients medium complexity score (i.e. 7–9), and two had high complexity score (i.e. ⩾10). Average blood loss was 200 ml, warm ischemia time was 18.46 min and postoperative stay was 3.55 days. All the 15 specimens sent for histopathology were confirmed as AML (angiomyolipomas) with margins free of tumor. Follow up CECT done at 4 months postoperatively revealed functioning residual renal parenchyma with prompt excretion of contrast.
Conclusion:
Large AML’s are also amenable to nephron sparing surgery. However patient should always be warned about the possibility of total nephrectomy. Selective angioembolization helps in reducing the blood supply and risk of torrential bleeding thus facilitates in the removal of the tumor and increasing the chances of nephron sparing surgery.
Introduction
Angiomyolipomas (AMLs) are the most frequent benign renal tumor, with a prevalence varying between 0.2% and 0.6% and a strong female predilection. They occur as sporadic, isolated entities in 80% of cases. The remaining 20% of AMLs develop in association with tuberosclerosis complex (TSC) or pulmonary lymphangioleiomyomatosis (LAM).1,2
AMLs are considered as a heterogeneous group of neoplasms. Many types display different pathology, radiological features, and clinical behavior, although they all consist of variable proportions of the same three elements: smooth muscle, blood vessels, and adipose tissue.2,3
Imaging plays a central role in the diagnosis and management of renal AMLs. The detection of adipose tissue is the fundamental diagnostic criterion of a classic AML. 2 However, a minority of AMLs lack visually detectable fat on imaging, making it harder to distinguish from renal cell carcinoma (RCC). Therefore, accurate preoperative diagnosis of renal AMLs is critical to prevent unnecessary nephrectomies and preserve renal functions. 4
About 80% of AMLs present as isolated entities, most commonly manifesting in middle-aged women. They tend to be single and small and rarely progress to cause significant morbidity.3,5
In the remainder 20% of cases, AMLs occur in association with TSC or, less commonly, as part of LAM. Relative to the sporadic form of AML, these hereditary lesions affect both genders equally and manifest at a younger age. They are likely to be multiple, large, and bilateral, and are prone to grow and be more aggressive.3,5,6
AMLs are observed in approximately 75% of patients with TSC. TSC is an autosomal dominant multisystem disorder characterized by the development of benign tumors (hamartomas) in multiple organs throughout the body. The main organs involved are the brain, skin, lung, and kidney. 7 TSC is caused by mutations in one of two genes, TSC1 and TSC2, which encode the proteins hamartin and tuberin, respectively. These proteins interact with each other to form a tumor suppressor complex, which inhibits the mammalian target of rapamycin (mTOR) pathway. This pathway is important for angiogenesis, protein synthesis, and cell growth. Defective or deficient TSC1 or TSC2 activity leads to unchecked activation of mTOR and formation of characteristic hamartomas.2,6,8
AMLs may also develop in patients with LAM. This rare disorder may occur sporadically, in the absence of other diseases, but is common in patients with TSC. It is characterized by diffuse interstitial proliferation of smooth muscle cells (LAM cells) and the presence of thin-walled cysts distributed throughout the lungs. These LAM cells have mutations in the same TSC1 and TSC2 genes.6,8
In our study main aim was to look for the feasibility and outcome of simultaneous angioembolization and nephron sparing surgery in large renal angiomyolipomas. The presenting complaint in all the patients was flank discomfort and the tumor was diagnosed on abdominal ultrasonography.
Materials and methods
A prospective study of carried out from 2016 to 2019. A total of 15 patients were included in the study with a lesion (angiomyolipoma) more than 10 cm in size (10–19 cm) suitable for nephron sparing surgery. The workup of the patients included history, baseline blood investigations, ultrasonography, and CT urography including angiographic films. The other kidney was normally functioning in all the patients and all the patients were explained in detail and written informed consent was taken about the nature of procedure and need for radical procedure if the need arose. All the patients were taken up for renal angiography and selective angioembolization of the feeding vessels of the AML carried out by the interventional radiologist (Figures 1(a), (b), 2(b) and (c)) followed by partial nephrectomy in the same sitting. The short term outcomes studied were warm ischemia time, average blood loss, and length of post-operative hospital stay. The oncological outcome was evaluated by noting the surgical margins of histopathological specimen and functional outcome by assessing the function of the preserved renal parenchyma.
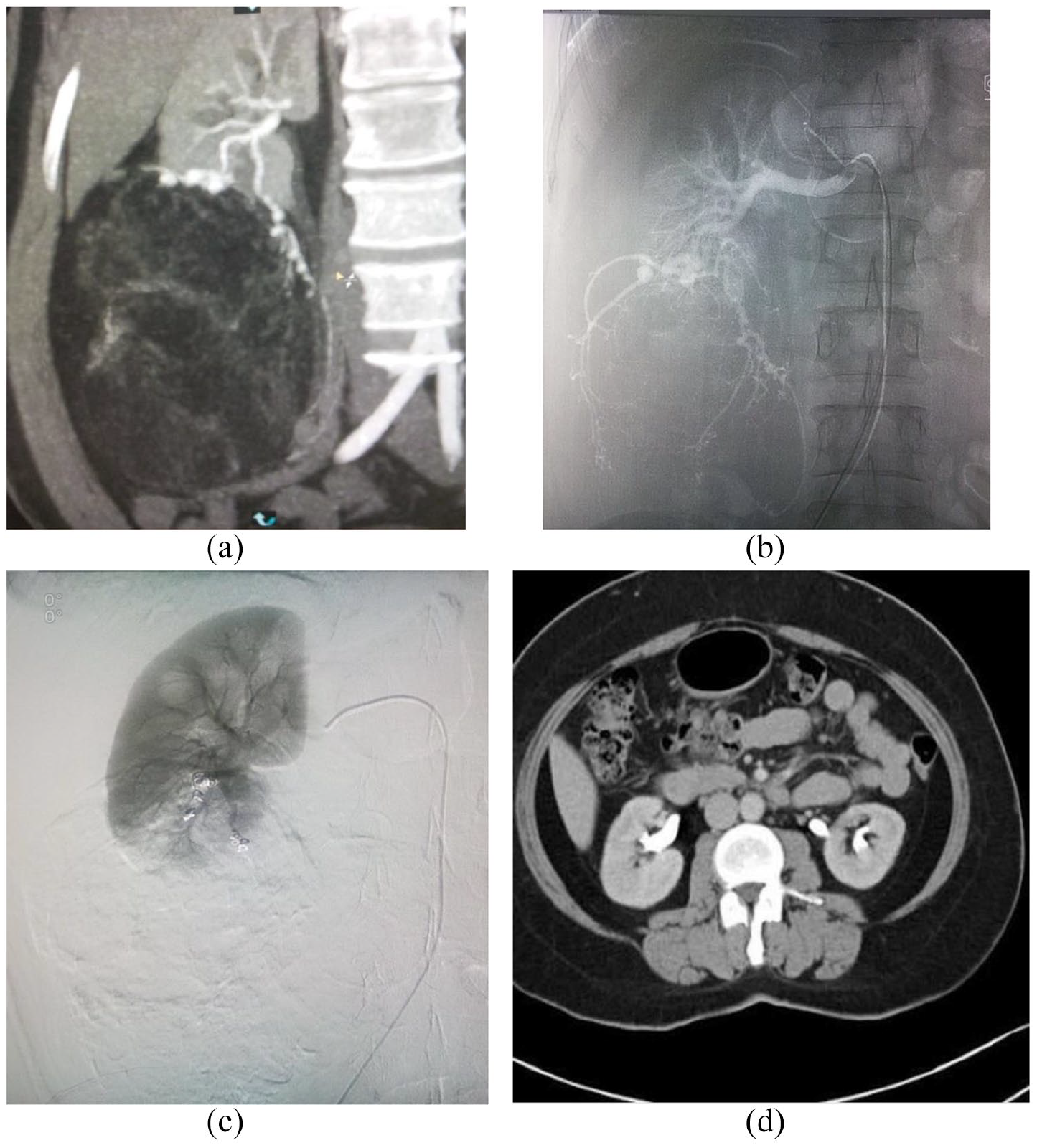
(a) CECT abdomen showing 15 × 9 × 10 cm AML, (b) angiographic film showing tortuous feeding vessels, (c) post coil embolization CT film, and (d) follow up CECT film at 4 months.
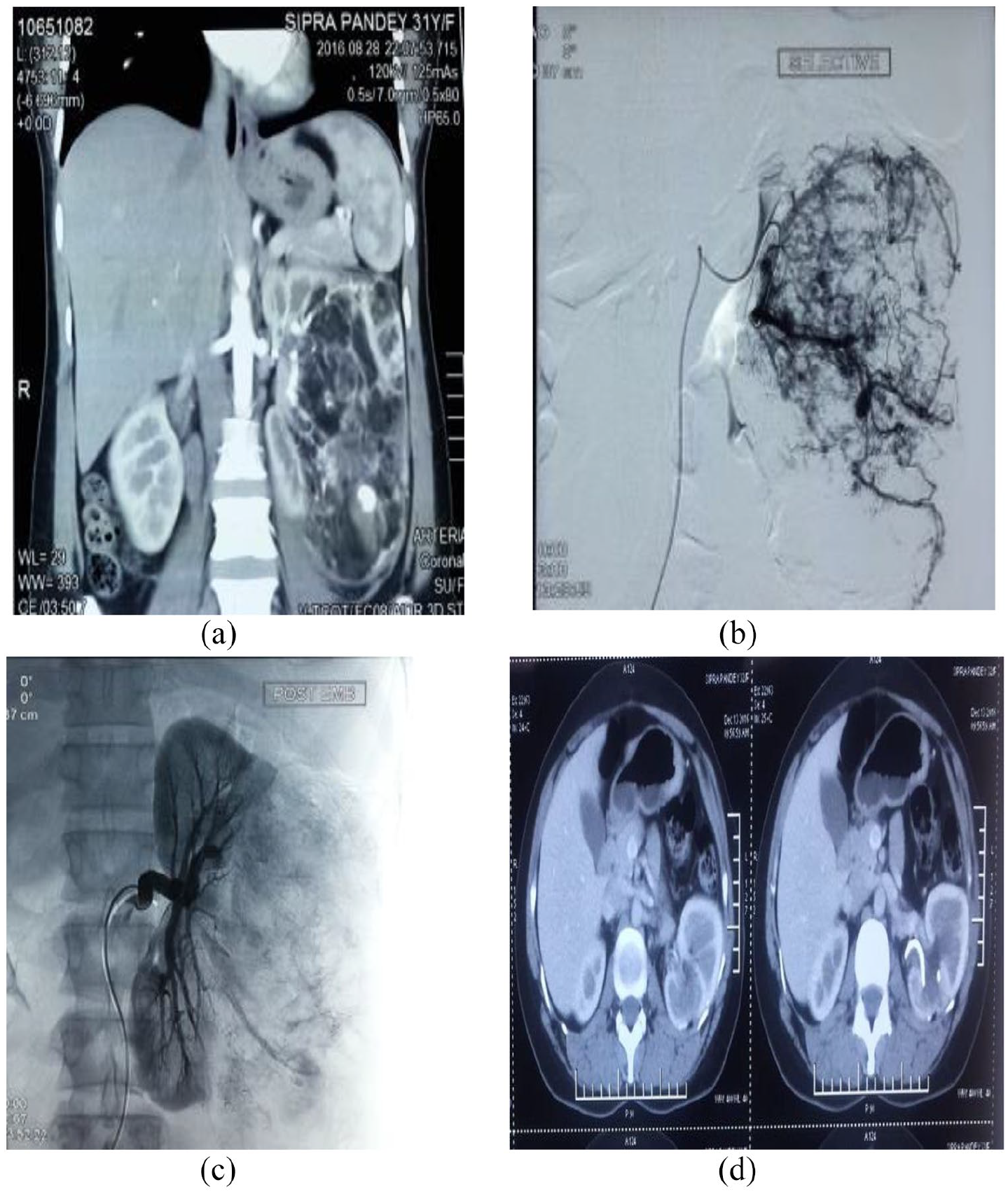
(a) CECT abdomen showing 17 × 14 × 14 cm AML, (b) angiographic film showing tortuous feeding vessels, (c) post coil embolization CT film, and (d) follow up CECT film at 4 months.
Surgical technique
All the procedures were done in supine position using anterior subcostal incision, colon was reflected and hilar control was taken in all the patients using bulldog clamps, warm ischemia time was noted, average blood loss measured, pelvicalyceal system if opened was repaired using 4-0 vicryl after stent placement.
Post operative care
All the patients were mobilized out of bed on second postoperative day and catheter was removed once patients were ambulatory and pain free. Drain was removed once 24 h drainage was less than 50 ml and post operative ultrasonography showed no collection.Postoperative stay in patients ranged from 3 to 5 days with a median of 4 days.
Results
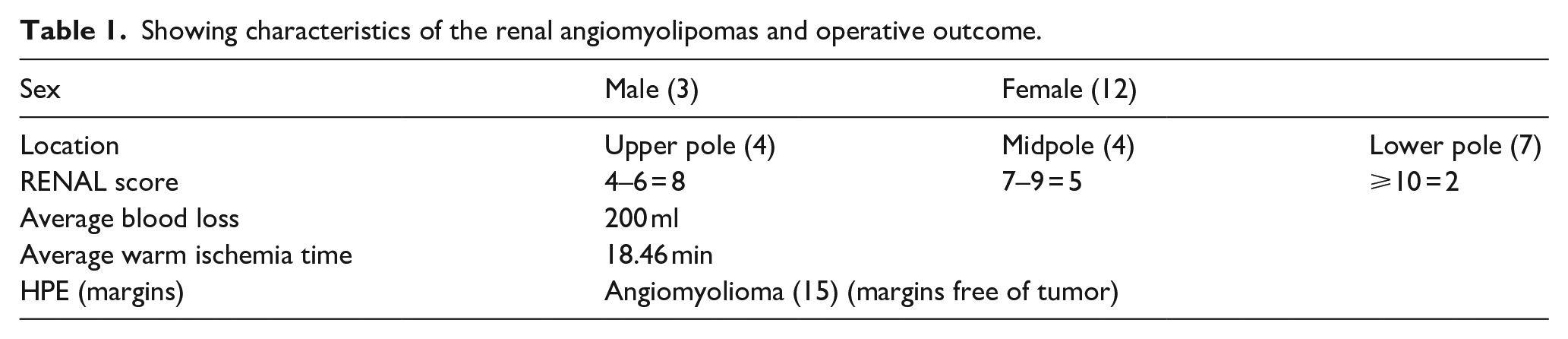
Twelve out of fifteen cases were female. The mean age was 42.25 years. All the patients had lesion more than 10 cm with seven tumors located in the lower pole, four in mid-pole, and four in upper pole. Eight patients had low complexity score on RENAL score (i.e. 4–6), five patients medium complexity score (i.e. 7–9), and two had high complexity score (i.e. ⩾10). Average blood loss was 200 ml, warm ischemia time was 18.46 min and postoperative stay was 3.55 days (Table 1). All the 15 specimens sent for histopathology were confirmed as AML (angiomyolipomas) with margins free of tumor. Follow up CECT done at 4 months postoperatively (Figures 1(d) and 2(d)) revealed functioning residual renal parenchyma with prompt excretion of contrast.
Showing characteristics of the renal angiomyolipomas and operative outcome.
Discussion
Angiomyolipomas are rare lesions, arising in the kidney and are a part of a group of tumors with a diverse appearance known as PEComas (tumors of perivascular epitheliod cell origin). Angiomyolipoma most commonly occurs in the kidney. The typical sporadic presentation is of a middle-aged woman with a single asymptomatic tumor. Sporadic angiomyolipomas appear to have a slow growth rate and are usually detected incidentally. Large angiomyolipomas can be confused with retroperitoneal liposarcomas, which are very rare. 7
The classical clinical presentation of AML is a palpable tender mass, flank pain, and gross hematuria, known as Lenk’s triad. 9 The two major morbidities associated with renal AML are retroperitoneal hemorrhage and impingement of AML on the kidneys and other vital organs. 10 In general, most symptomatic angiomyolipomas have been relatively large and most studies in the literature have focused on a 4-cm cut point. 7
AML is the only benign renal tumor that is confidently diagnosed on cross-sectional imaging. There are two imaging characteristics that are highly suggestive of an angiomyolipoma. On ultrasound, they are echogenic. On CT scan, they have the density of fat, which is less than that of water. 11 The presence of fat (confirmed on non-enhanced thin-cut computed tomography) by a value of −20 Hounsfield units or less seen within a renal lesion on imaging is considered the diagnostic hallmark. MRI can also be used to identify the fatty tissue. However because the presence of bleeding in any renal tumor can mimic the typical pattern of angiomyolipoma, MRI should not be considered the diagnostic method of choice. AML can vary in size from a few millimeters to larger than 20 cm. It is unusual to see an AML over 10 cm, therefore many studies have demonstrated that any AML measuring over that number is considered as “giant.” CT findings usually help to differentiate AMLs from other tumors, such as perinephric liposarcomas.11,12
Treatment must be individualized for optimal management of angiomyolipoma, 4 Large renal AMLs can rupture which can be sudden and painful with manifestations of hypovolemic shock. The management of AMLs has been correlated with symptoms. The management should take into account the size of the tumor, presence of symptoms, and patient factors. In particular, the risk of hemorrhage must be weighed during evaluation. 4 Tumors larger than 8 cm generally tend to be symptomatic and they are at a greater risk of spontaneous or traumatic rupture resulting in hemorrhagic complications. These patients are therefore treated by selective arterial embolization as a first line.12,13
Giant renal AMLs are exceedingly uncommon and review of literature showing few cases of giant renal AMLs, all of which required radical nephrectomy for definitive treatment, with variable outcome.14–19 Several cases of giant renal AMLs excised using partial nephrectomy have been reported.20–30 Exophytic renal AMLs of large size may be easily confused with malignant conditions on CT imaging, such as well-differentiated forms of perirenal liposarcomas. However, sharp defects in the renal parenchyma and the presence of enlarged vessels on CT imaging favor the diagnosis of renal AML. Although possible, very rarely has liposarcoma been found to arise from within the renal parenchyma. 31 All the patients with large renal angiomyolipomas a due consideration should be given to pe operative angioembolization so as to avoid any torrential bleeding and lok for the possibility of nephron sparing surgery.
In our study the patient population was specifically chosen to assess for the possibility of nephron sparing surgery especially when the AML is large with size more than 10 cm (10–19 cm in our study).The other kidney was normally functioning in all the patients with no lesion. The use of preoperative selective angioembolization although demanding significantly reduces the blood supply to the AML and thereby significant decrease in perioperative blood loss, warm ischemia time, and increases the chances of nephron sparing surgery in an otherwise radical procedure.
Conclusion
Large AML’s are also amenable to nephron sparing surgery. However patient should always be warned about the possibility of total nephrectomy. Selective angioembolization helps in reducing the blood supply and thus facilitates in the removal of the tumor and increasing the chances of nephron sparing surgery in a large renal angiomyolipoma which may otherwise warrant radical nephrectomy.
Footnotes
Acknowledgements
Highly thankful to my guide Dr Anshuman Agarwal for his support and guidance.
Author contribution
MA Rouf: Project development, Manuscript writing; Shayesta Ali: Project development, Manuscript writing; V Kumar: Project development, Manuscript writing; Mahendra Sharma: Project development; Anshuman Agarwal: Project development; Vijay Rawat: Project development.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Approved by hospital ethics committee.
Informed written consent
Explained and Taken.
Guarantor
Dr Malik Abdul Rouf