
Abstract
Objective:
To evaluate the features and prognosis of melanoma of glans penis and urethra, with the presentation of a significant case report.
Materials and methods:
A systematic literature review was performed using the MEDLINE (PubMed) and Cochrane Libraries databases to identify all cases of male mucosal melanoma reported.
Results:
Two hundred fifty-two patients with male mucosal primary melanoma were found. Glans penis and fossa navicularis as primary site includes the 81.6% of all lesions considered. Median Breslow’s depth is 2.1 mm, whereas nine in situ melanomas have been reported. At the diagnosis, the disease was at a non-localized stage in 21.4% for glans penis melanomas and 11.7% urethral lesions, respectively. The 2 and 5-year survival for glans melanoma is 62.5% and 38.4%; higher rates were observed in the 2012–2020 period (76% and 58.8%, respectively). Two-year survival for urethral melanomas is 66.7%, while 5-year survival is 12.5%. 22 patients survived over 5 years with a Breslow’s depth reported always < 3.3 mm.
Conclusion:
Melanoma of the glans penis and urethra is a rare neoplasm associated with a poor prognosis, however recent reports show higher survival rates. Surgery remains the mainstay for a localized disease. Taking into account the small number of cases reported, topical imiquimod seems to be a valid non-surgical alterative for melanoma in situ. The use of immunotherapy and targeted therapy should be considered only in an adjuvant setting according to the recommendations of cutaneous melanoma; however, additional clinical data on male mucosal melanoma are needed to draw definitive conclusions.
Introduction
Primary malignant melanomas of the glans penis and urethra are rare neoplasms occurring in < 0.1% of all melanomas. 1 Although these tumors have been classified together with penile melanomas of the skin shaft and prepuce, melanomas arising from glans and urethra are more accurately described as mucosal melanomas, differing significantly from cutaneous melanomas in terms of presentation, genetic profile, staging, response to treatments, and progression. 2 Given the rare presentation, the local anatomy that makes margin-free surgery challenging and the scarce evidence reported in the literature, specific guidelines referred to early stages mucosal melanomas are lacking; moreover, in case of advanced disease, indications and protocols are often bases on experts’ opinions, and without the availability of any strong evidence, the therapy recommended for cutaneous melanoma may be offered to patients with mucosal melanoma.3,4
In this context, the recently established European Reference Networks focused on rare urorectogenital diseases and complex conditions (ERN eUROGEN), including also glandular and urethral melanoma, highlighted new attention to the field, and started to work on new Guidelines in order to optimize care pathways and innovate cure potential for all these rare condition in the European Union. 5
In the present paper we report a case of melanoma of glans penis with long-term urethral recurrence in a 41 year-old Caucasian man. In addition, we performed a systematic review on this rare and complex clinical entity, in order to summarize and collect all the available published evidence.
Case Report
A 41-year-old Caucasian man presented with a recently appeared, fast-growing, asymptomatic pigmented macule on his glans penis. His medical history was notable for neurofibromatosis type 1, while no familiar history of melanoma was reported. Physical examination revealed an irregular lesion, measuring approximately 2 cm at its maximum diameter, with a variable pigmentation from the light brown to black and mucosal paler regions of regressive origin involving half of ventral surface of the glans; in this context, a 5 mm amelanotic nodule was revealed (Figure 1(a) and (b)). Inguinal lymph nodes were not palpable. A diagnostic biopsy confirmed the clinical suspicion of malignant melanoma. The patient was submitted to glansectomy and sentinel lymph node biopsy. On histopathological examination, the hematoxylin-eosin stained sections revealed a malignant melanoma arisen in melanosis characterized by horizontal growth with a vertical phase nodule infiltrating the chorion for 2 mm Breslow’s depth, characterized by fused and pigmented epithelioid cells showing a marked polymorphism and a mitotic rate of 6/mm2 with vascular invasion features. Histological margins were negative whereas one right inguinal lymph node resulted positive for micrometastasis. A right inguinal-iliac-obturator lymphadenectomy was subsequently performed showing no secondarisms. The patient was then referred to a multidisciplinary team with indication to adjuvant therapy with interferon and a regular clinical, dermoscopic and radiological follow-up. No evidence of disease was shown until, 76 months after surgery, a sudden onset of urethrorrhagia and hemospermia was reported; the physical examination and urethroscopic investigation confirmed a black nodule involving the neo-meatus and extending along the penile urethra for 1 cm (Figure 1(c) and (d)). The patient underwent to excisional biopsy of the lesion and meatoplasty, histologically confirming melanoma recurrence; immunohistochemical analysis revealed no BRAF, NRAS, and KIT mutations. No complications was reported and 1 day after surgery the patient was discharged from our hospital. At 24 months follow-up, no clinical or pathological recurrences were documented.
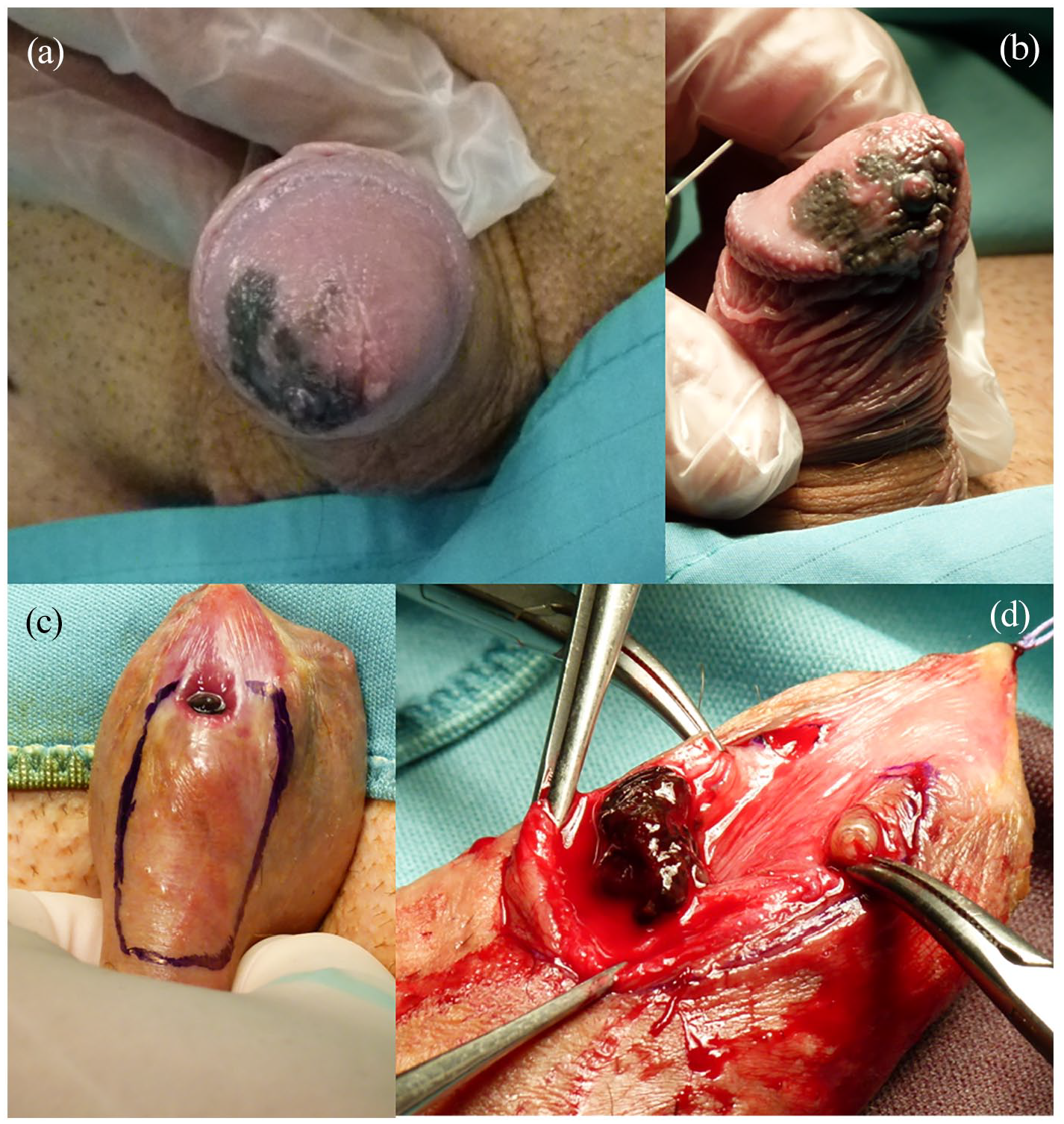
(a) Mucosal melanoma revealing variable pigmentation mucosal paler regions of regressive origin involving the ventral surface of the glans penis. (b) 5 mm amelanotic nodule was suspicious for vertical growth. (c and d) Clinical presentation showing urethral recurrence 76 months after diagnosis.
Methods
A MEDLINE, Cochrane Library, and National Center for Biotechnology Information PubMed search for relevant published articles was performed by combining the following key words: “urethra,” “glans,” “penis,” “penile,” and “melanoma.” For the MEDLINE search, we used the following filters: languages (English), species (humans), text availability (full text availability). No filters were applied for the date of publication (review conducted in March 2020). Subsequently, the references of the retrieved articles were also used to identify any other relevant studies. Each article and abstract was reviewed for its appropriateness and relevance to the topic of this review.
Two reviewers (F.P. and A.F.) independently screened all abstracts and full-text articles. Disagreements were resolved by discussion, and where no agreement was reached, a third independent reviewer (G.G.) acted as an arbiter.
To be included, studies had to explicitly report adequate patient data (Figure 2). Reports on patients with cutaneous melanoma, melanoma metastasis, or regarding female urethra were not included.
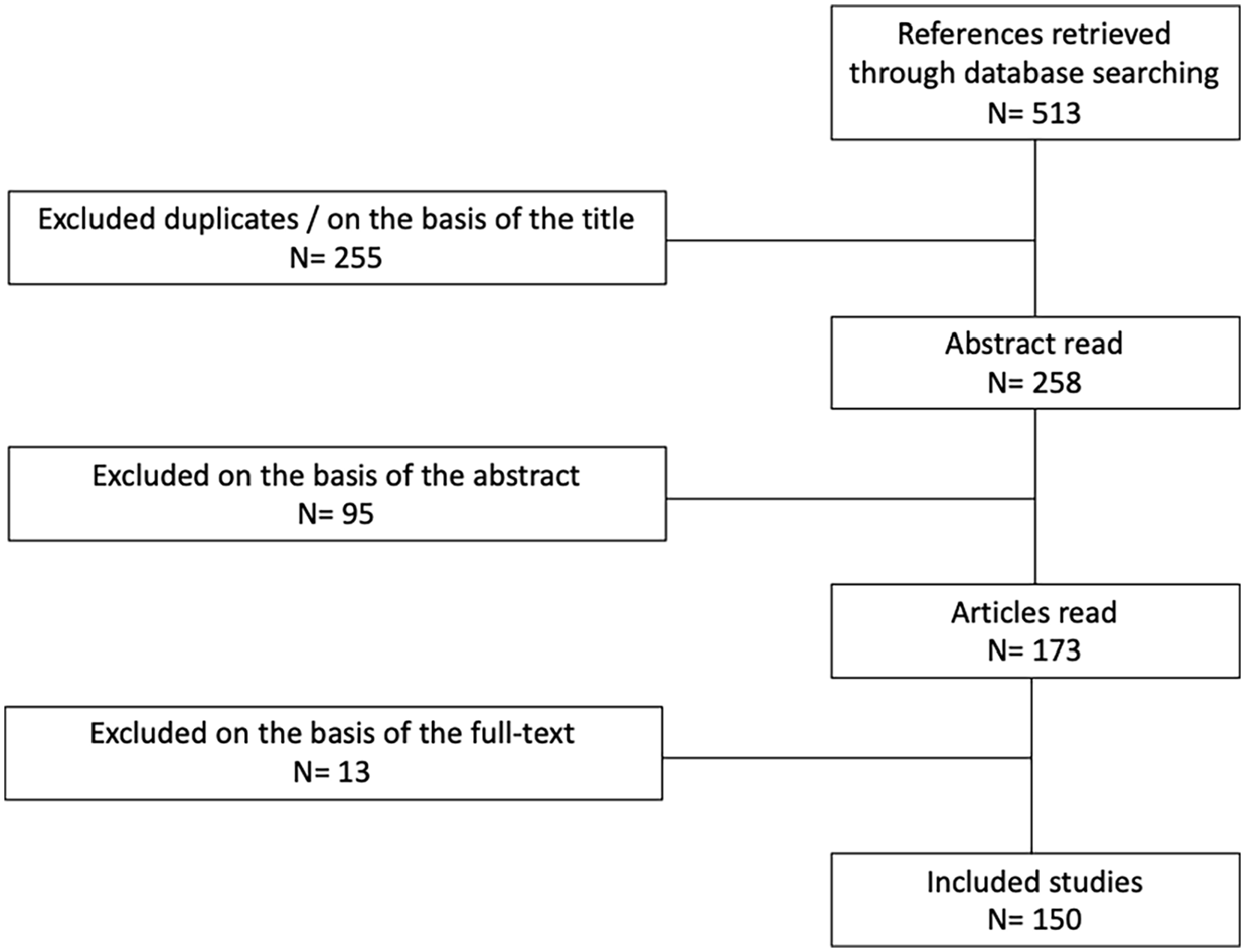
Flow diagram of the search results.
Results
One hundred fifty articles reporting on 251 patients (252, including the present case) with primary melanoma of the glans penis and urethra were identified in the literature research. Patients’ data are reported on Table 1.
Clinical presentation of glans penis and male urethra melanoma according patient’s age and anatomical site: review of the literature.
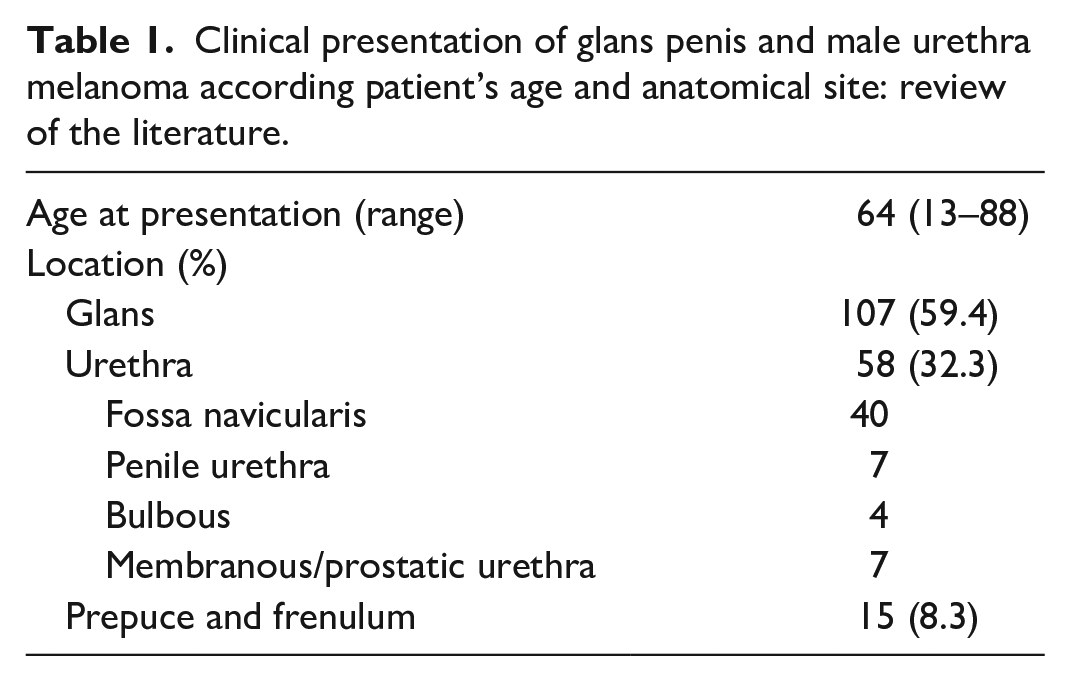
In case of glandular lesions, a meatal or coronal involvement is reported in 24.2% and 9.3% of cases, respectively, meanwhile glans penis and fossa navicularis as primary site includes the 81.6% of all lesions considered.
Features of the reported cases revealed to be difficult to estimate; for example, Jabiles et al. 6 report contradictory data in two different tables regarding a melanoma of the glans penis afflicting a 17-year-old patient, while Turnbull et al. 7 do not accurately report the age of patients presented in their case series. Only one systematic revision of the literature has been performed 1 ; since then, 31 additional cases have been reported (Table 2).8,9
Male patients with glans or urethral melanoma reported in literature between January 2012 and March 2020.
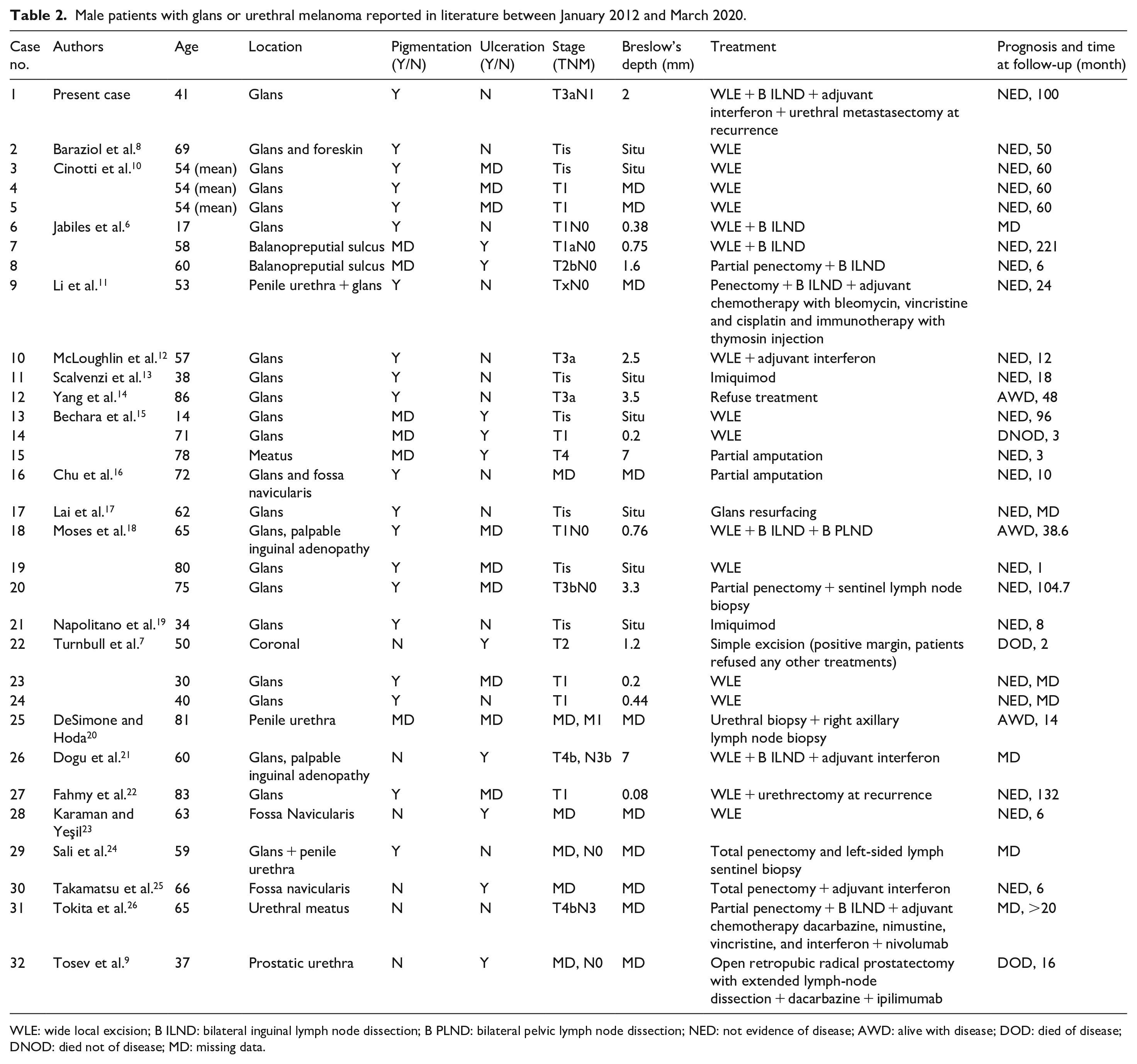
WLE: wide local excision; B ILND: bilateral inguinal lymph node dissection; B PLND: bilateral pelvic lymph node dissection; NED: not evidence of disease; AWD: alive with disease; DOD: died of disease; DNOD: died not of disease; MD: missing data.
Overall median Breslow depth reported is 2.1 mm. Of melanoma located on glans, nine in situ lesions have been reported, six of which (66.6%) published in the last 7 years. 8
At the time of diagnosis of melanoma of the glans penis or urethra, the disease was in a non-localized stage in 21.4% and 11.7% of cases, respectively.
The 2 and 5-year survival for glans melanoma, considering the available data, is 62.5% and 38.4%. In light of this, higher rates were observed in the 2012–2020 period: 76% and 58.8%, respectively. Two-year survival for urethral melanomas is 66.7%, while 5-year survival is 12.5%.
In this context, cases with follow-up of at least 5 years are very rare. In detail, 22 patients survived over 5 years: a recurrence has been documented in 27.3% of cases with a median time of 35.5 months.1,6,10,15,18,22 In addition to this, the reported Breslow’s depth was always less than 3.3 mm.
Discussion
Etiology and risk factors
Melanomas are malignant tumors arising from melanocytes from neural crest. Although melanoma is mostly of cutaneous origin, it can also occur in various extracutaneous sites where pigment cells are present, such as ocular, leptomeningeal and mucosal regions. Mucosal melanoma is a rare subtype of melanoma, comprising 4% of all melanoma cases. 27 Etiological risk factors for genitourinary mucosal melanoma are poorly understood compared with cutaneous melanoma. In particular, ultraviolet radiation, strong risk factor for the development of cutaneous melanoma, has not been involved in the etiopathogenesis of melanoma of glans and urethra. In this context, this risk factor has been considered only in the case of in situ melanoma affecting the penis of a naturist reported by Lai et al. 17 The case we report was affected by neurofibromatosis type 1; in this regard neurofibromin protein mutations have been associated with an increased risk of neural crest tumors, where melanocytes originate, but no convincing evidence for an increased risk of malignant melanoma has been found. 28 In a study comparing cutaneous melanoma to those with genital and anorectal melanoma, family history of melanoma was a risk factor strongly associated with development in a mucosal site. During follow-up, 6% of patients diagnosed with mucosal melanoma subsequently developed cutaneous melanoma. 29 Nevertheless, poor prognosis has been highlighted for NF1 mutated melanomas. 30
Genetic profile
Mucosal melanomas show aberrations of the MAPK pathway, including frequent mutations in NRAS, BRAF, NF1, and KIT. Alterations to SF3B1, KIT, and NF1 are relatively common compared to cutaneous melanomas, while mutations to BRAF and NRAS are less frequent in mucosal melanomas. Many somatic mutations have been identified among cutaneous melanomas, most commonly in BRAF, represented in up to 62% of all cases, NRAS (10%–28%) and NF1 (14%). In contrast, approximately 55% of mucosal melanomas show wild-type patterns for these genes. Up to 39% harbor c-KIT mutations, 12% NRAS mutations and 9%–19% BRAF mutations.31,32
More recently, mutations resulting from ultraviolet radiation exposure were identified in some melanomas from facial mucosal sites while confirmed to be absent from lower body mucosal sites, suggesting the need to differentiate the different types of mucosal melanomas according to the anatomical regions involved. 31
Clinical presentation
Glans melanomas appear as macular lesions or nodules; usually their pigmented or amelanotic appearance guides the differential diagnosis, ranging from melanosis, melanocytic nevi, submucosal necrosis, lymphomas, angiokeratomas.33–35 In this context, dermoscopy and confocal microscopy have been proposed as useful tool in early diagnosis and during follow-up. 13
The clinical presentation of urethral melanomas includes hematuria, urethrorrhagia and other lower urinary tract symptoms and must be differentiated from the most common urothelial and prostate cancers. The development of this type of neoplasm in a not visible area could be one of the causes of the worse prognosis of urethral melanomas as compared to the glans melanomas. 1
Staging
In staging glans and penile melanoma, most investigators use the three-stage system proposed by Bracken and Diokno 36 :
Stage I—disease confined to the penis,
Stage II—disease spreading to the regional lymph nodes,
Stage III—disseminated disease.
For urethral melanomas, a staging system proposed by Levine 37 has been widely used:
Stage A—tumor confined to the submucosa,
Stage B—tumor infiltrating the corpus spongiosum in men and the periurethral muscle in women,
Stage C—tumor extending beyond the corpus spongiosum in men or periurethral invasion including vagina, bladder, labia, or clitoris in women
Stage D—tumor with metastasis to lymph nodes
In addition to this, some authors use the VIII edition American Joint Committee on Cancer staging system that is based on the TNM system (tumor size, lymph nodes, and metastasis); on the other hand, this may not be considered sufficiently accurate since the skin melanoma staging system does not necessarily take into account the particular anatomical structures of these regions. 38
Standard Breslow staging based on invasion depth is not used for primary urethral melanomas. Testing of the primary melanoma for oncogenic mutations (e.g. BRAF, NRAS) is not recommended in the absence of metastatic disease. 4
Treatment and prognosis
A recent metanalysis revealed a cancer specific mortality for mucosal melanoma 2.25 times higher than that of cutaneous disease. 39 Papes et al. 1 reported a 5-year survival for glans penis and urethral melanoma of 22.5% and 10%, respectively; while factors that have been shown to adversely impact on prognosis include Breslow depth > 3.5 mm, presence of ulceration and microsatellites, and tumor diameter > 15 mm. 40 Our contemporary review of the literature shows slightly higher survival rates: this may be due to early diagnosis, considering the higher number of in situ melanoma cases published in more recent years, and to the improvement of treatment strategies over time.
Since decades, surgical approach has been the mainstay of melanoma treatment. Although the American Academy of Dermatology clearly state that their guidelines are not addressed for mucous forms of melanoma, surgical margins recommendations to be observed in relation to the tumor thickness are indicated as follows 4 :
Situ–0.5/1 cm
⩽1.00 mm–1 cm
>1.0 mm to 2.00–1/2 cm
>2.00 mm–2 cm
In the genital regions, these margins can be modified for functional and anatomical reasons, especially when an organ-sparing surgery is considered. Positive excision margins lead to an increased risk of local recurrence, although this is not quantifiable exactly with the available evidence.
As non-surgical option, topical imiquimod 5% cream may be used as second-line treatment for in situ melanoma, when surgery is not possible at the outset (primary setting) or when optimal surgery has been performed (adjuvant setting), while radiation therapy should be used only in case of non-surgical cases. 4
Although lymphadenectomy has been used extensively in the various revised reports, the real benefit of this procedure remains uncertain, while it is well known that is associated to a significantly comorbidity. The sentinel lymph node biopsy for staging reasons should be performed in cases with Breslow’s depth < 1 mm, but in case of positivity the real benefit of lymphadenectomy is still questionable even in cutaneous forms of melanoma. Furthermore, in urethral forms the challenge of having clear-cut information on the thickness does not help in the decision-making process for the sentinel lymph node biopsy.
To date, no recommendation can be made for or against the routine use of neoadjuvant therapy for adults with resectable regional or distant metastatic cutaneous melanoma. 3
Systemic treatment of melanoma has changed rapidly since the introduction of ipilimumab in 2011. 41 In less than 10 years, nine new drugs have been approved for adjuvant treatment of metastatic melanoma. Newer therapies approved for melanoma include immunotherapy, targeted therapy for mutation-bearing tumors, and injectional therapy for cutaneous or palpable lesions. Overall survival rates for melanoma are improving rapidly, with dramatic increases in long-term survival observed with administration of these new therapies. 42 In 2020, the American Society of Clinical Oncology clearly suggested that patients with mucosal melanoma may be offered the same therapies recommended for cutaneous melanoma. 3
Male mucosal melanoma is a rare disease; given the recent introduction of new therapies, it is at the moment impossible to draw definitive conclusions about their real effectiveness in this disease. New efforts in Clinical Practice Guidelines development and implementation by the ERN eUROGEN 5 are currently in the pipeline. Thanks to these efforts, the next future will bring new light and guidance for the highly needed improvements in treatment strategies in this field.
Conclusion
Melanoma of glans penis and urethra is an aggressive rare neoplasm with high mortality rate, whose management comes from low-quality evidence based on reports or small case series. Surgical treatment remains the mainstay for early-stage male mucosal melanomas, whereas topical imiquimod seems to be a valid non-surgical alterative for melanoma in situ. The use of immunotherapy and targeted therapy should only be considered in an adjuvant setting; however high quality data based guidelines are mandatory for proper management of this rare disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.