
Abstract
Dear Editor,
We read thoroughly the review “Current and future applications of machine and deep learning in Urology: a review of the literature on urolithiasis, renal cell carcinoma, and bladder and prostate cancer.” 1 We found it very interesting because it provided an exhaustive overview of the main application of “Radiomics” to the most common urologic diseases, delineating what the near future of urologic Radiology could be.
Radiomics is a field of growing interest in Radiology, representing new forms of diagnostics that will potentially revolutionize Radiology and wider healthcare, allowing doctors to predict and more accurately diagnose disease and to develop personalized treatments.
Radiomics consists of the quantitative analysis of routine medical imaging data (US, CT, or MRI), which allows extracting clinical information with a high predictive value in terms of prognosis and therapeutic response. In other words, it is possible to identify the so-called “imaging biomarkers.” This is based on the hypothesis that a pathological tissue is characterized by distinct imaging phenotypes in comparison to healthy tissues, and that these differences can be captured by the extraction and the analysis of features from medical imaging data. Imaging biomarkers, along with other clinical information, have the advantage to be used in combination to develop predictive models for clinical decision support systems. Therefore, it will become possible to create dynamic algorithms of artificial intelligence to the conventional imaging techniques, which analyze a huge quantity of data and facilitate the identification of intricate pathological patterns. Artificial intelligence, combined with radiomic analyses, is candidate to play an important role in the future of Radiology, helping improve efficiency and diagnostic capacity.
In the following text, we will describe recent applications of Radiomics and artificial intelligence in the main urological diseases, such as urolithiasis, renal cell carcinoma, bladder cancer, and prostate cancer, focusing on their efficacy to predict patient outcomes.
Despite novel instrumental advancements in urinary stone surgery, decision-making, and patient counseling remain a challenge for clinicians. Through the application of artificial intelligence model based on radiomic features, it was possible to obtain highly accurate clinical biomarkers in terms of predicting kidney stone type (97.1%), stone free-rate (98.2%), and success-rate after a single-session shock wave lithotripsy (92.3%). 1
Another important application of Radiomics is the differential diagnosis between benign and malignant renal masses, and defining their prognosis. The accuracy in discriminating between angiomyolipoma (AML) and clear cell RCC (ccRCC), and papillary RCC (pRCC) was 90.7%–100%. 1 Other studies have shown that artificial intelligence models constructed from CT imaging texture features can accurately distinguish between ccRCC high and low grades, with accuracy ranging from 73% to 93%. 1
A further application of Radiomics to renal cancer was represented by the “radiogenomics,” which is the combination between radiomic and genomic features. Kocak et al. evaluated the potential of quantitative CT scan texture analysis to predict the presence of PBRM1 mutations, which is the second most commonly identified mutation in ccRCC. This algorithm correctly classified up to 95% of ccRCC, 1 representing a promising results for developing non-invasive imaging biomarkers of histopathologic subtypes, prognosis, and treatment response, with comparable performance to percutaneous renal biopsy.
MRI-based radiomic analysis has shown to be accurate in the preoperative discrimination between low- and high-grade BCa, with 83% accuracy detection. 1 This may aid to the main limitation of cystoscopy in discriminating between areas of malignancy and healthy urothelium given the multifocal nature of the disease and inconspicuous but significant lesions such as carcinoma in situ. Another advantage could be the decrease in the number of unnecessary biopsies.
Also in bladder cancer algorithms have been employed to create recurrence and survival predictive models, and the early assessment of chemotherapeutic efficacy or failure to reduce unnecessary morbidity, improve patients’ quality of life, and reduce costs. 1
The main application of Radiomics in the field of prostate cancer (PCa) is represented by distinguishing between patients with low and high cancer risk, to avoid unnecessary biopsy and the potential complications in the low-risk patients. In a recent study, an intelligence artificial algorithm was able to prevent 48% of patients without PCa from undergoing prostate biopsy, missing only 16% of PCa and 6% of GS ⩾7; NPV was 76% for any PCa and 94% with GS ⩾7. 1 Another application is the development of various radiomics models based on pre- and post-intensity-modulated radiotherapy (IMRT) MRI data for individualized treatment response prediction in PCa patients, to detect early IMRT response with reliable performance. 1 Similarly, a novel method of processing automated performance metrics was able to evaluate surgical performance and predict clinical outcomes after robot-assisted radical prostatectomy, such as hospital stay, operative time, Foley catheter duration, and urinary continence, with over 85% accuracy. 1 Finally, in a recent study, an algorithm for the prediction of early biochemical recurrence showed an AUC >0.95. 1
Artificial intelligence technologies have been attracting substantial attention in Urology; however, their real-life implementation still faces obstacles. Several limitations exist in most studies applying Radiomics and artificial intelligence to urological diseases. First, the variability in study design, algorithms employed, training features used, and observed endpoints make it difficult to perform quantitative analysis. Second, most algorithms in these studies were validated with their dataset; therefore, they lack external validation and the generalizability of their results across other datasets is not applicable. Third, further algorithm development and research are particularly required in the field of urolithiasis to outperform conventional statistical methods as observed in uro-oncological investigations to reduce procedural costs and maximize patient outcomes.
Future research should focus on the construction of larger medical databases and further development of these techniques. Specialized software for image-guided, real-time, intraoperative decisions will require appropriate regulatory approvals to function with robotic platforms and expand to operating rooms worldwide. Issues remain regarding the trustworthiness of a computer’s diagnosis and that programming biases do not interfere with diagnoses. Human intuition, experience, and common sense will remain to play a crucial role in future developments to ensure that these systems are operating as intended and to deal with undesired consequences in a timely fashion.
Although the shared decision-making will not be replaced by these models, it may complement the information patients obtained from traditional methods.
Another new technique that may play an important role in the field of urological Radiology is represented by the introduction of diffusion-tensor imaging (DTI). It is a new non-invasive sequence of Magnetic Resonance Imaging, which has provided a deeper understanding of the anatomical features of periprostatic neurovascular fibers (PNF) in several recently published studies. This technique is based on the “anisotropic diffusion” of the water protons, by measuring how much the diffusion is oriented in one of the three gradient-directions in the axons. In the biological tissues such as nervous central and peripheral fibers with a strictly orientated texture, water protons diffusion is not casual or “Brownian,” but it occurs mainly along the longitudinal direction of the myelinated fibers (anisotropic diffusion). This phenomenon can be quantitatively assessed throughout the measurement of a specific parameter, that is fractional anisotropy (FA) for every single voxel in at least six non-collinear and non-coplanar directions. By integrating FA values of every single voxel, DTI is able to depict the direction of nerve fibers in all three dimensions of space, giving both quantitative and qualitative anatomic information.
In the last years, several studies have been published about the visualization of peri-prostatic neurovascular fibers (PNF) using DTI 2 (Figure 1). This new technique has been demonstrated able to describe the anatomical features of PNF and modifications induced by surgery after radical prostatectomy, which consists of a decrease of FA values.3,4 Further studies have also demonstrated how these modifications are related to surgical complications as erectile dysfunction. 4 Other authors have also demonstrated the usefulness of DTI in supporting the staging of prostate cancer in assessing early infiltration of the prostatic capsule, demonstrating that the decrease of FA values suggest an early infiltration of peri-prostatic capsule. 5
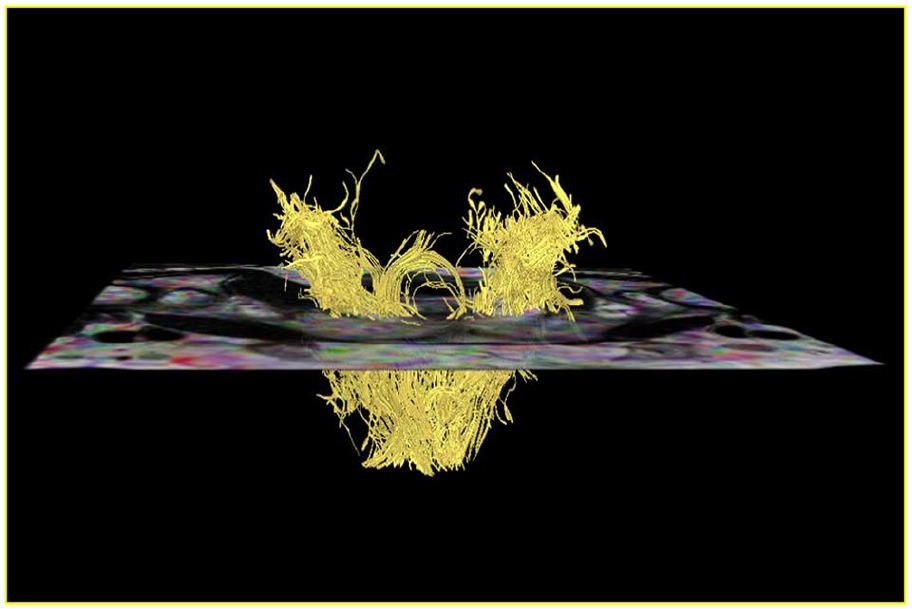
3D tractographic reconstruction of the periprostatic neurovascular fibers by means of diffusion tensor imaging (DTI).
The limitations of DTI studies of PNF are mainly represented by the absence of a gold-standard anatomical correlation as a reference for the depicted residual fibers. Further studies with the comparison with pathological specimens could be useful to validate the technique. Secondly, potential nerve fibers miscount may occur because linear non-nerve structures such as fibromuscular tissue, arteries, and veins can concur to generate fiber tracts. We believe that an improvement of the technical parameters for fiber software reconstruction and the spreading of 3-Tesla MRI scanner may support this need to perform a more selective and effective depiction of PNF, without the confusing effect of other kinds of structures.
Thank you very much for the possibility to express our view on the future of diagnostic imaging in urologic diseases.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.