
Abstract
Purpose:
To evaluate the safety of one-day length of hospital stay (LOS) after pediatric percutaneous nephrolithotomy (PNL), and to study the predictors of LOS.
Methods:
A retrospective study included pediatric patients who PNL for renal calculi more than 1 cm between January 2016 and October 2019. PNL was performed in prone position. The nephrostomy tubes and ureteric catheters were removed on the second day and patients were discharged if there was no perforation or significant residual stones. The stone free rate, LOS and the surgical complications were reported. Bivariate and multivariate analysis were used to predict the LOS.
Results:
220 patients were identified. The median age (range) was eight (Range: 3–17) years. Stone free rate was achieved in 200 patients (91%) of patients, while residual fragments were detected in 20 patients (9%). Complications, they were reported in 50 (22.7%) patients. 184 (83.6%) of patients stayed at the hospital for only 1 day, while 36 (16. 4%) stayed more than 1 day. Of 36 patients who stayed more than one-day, 34 had complications (p value <0.001).
On multivariate analysis, surgical complications was found to be the only predictor of longer LOS (p value <0.001).
Conclusion:
Early nephrostomy tube removal and 1-day length of hospital stay could be a safe option after pediatric PNL. Surgical complications is a statistically significant predictor of longer LOS.
Introduction
Pediatric calculi are an important health problem with a marked rise in their prevalence in the recent years. Some studies reported a fivefold increase in the prevalence of pediatric renal calculi in the developed and developing countries. 1 Most pediatric calculi can be effectively managed with Extracorporeal Shock Wave Lithotripsy (ESWL). However, it is limited by the retreatment rate, the need for more than one sitting and the high rate of auxiliary procedures. Thus, long term safety and efficacy of ESWL is debatable. 2
Percutaneous Nephrolithotomy (PNL) is a safe and effective way of managing pediatric calculi. Nevertheless, concerns regarding the length of hospital stay (LOS) may exist. The reported average length of hospital stay (LOS) after pediatric PNL ranges from 2 to 6 days which is related to the presence of a nephrostomy tube in situ.3–5 Some centers introduced tubeless PNL to decrease the post-operative pain and the LOS. However, it is suitable for a highly selected group of patients.6–8
Up to our knowledge, no studies in literature analyzed the regimen of early nephrostomy tube removal and short LOS after pediatric PNL. Our study aims to analyze the safety of one-day LOS after pediatric PNL.
Patients and methods
This study is a retrospective analysis of the medical records of pediatric patients aged less than 18 years, who had PNL performed for renal calculi more than 1cm between January 2016 to October 2019. Children with bleeding tendencies, horseshoe kidneys, and ectopic kidneys were excluded. Children were classified into two groups according to the length of hospital stay (LOS); group 1 (LOS = day) and group 2 (LOS >1 day). The study was approved by the local ethical committee and conforms to the provisions of Declaration of Heisinki.
Patients’ evaluation
Patients were preoperatively evaluated at our outpatient clinic by urine analysis and culture, serum creatinine, complete blood count (CBC), coagulation profiles and radiological investigations as abdominal ultrasonography (US) and non-contrast pelvi-abdominal computed tomography scan (NCCT). Preoperative urinary tract infections (UTIs) were managed with antibiotics according to cultures and sensitivity results. Stone size was calculated by measuring the longest diameter by NCCT. In cases of multiple stones, the stone size was estimated as the sum of the longest diameter of all stones. Stone hardness was assessed by measuring the Hounsfield units by NCCT. The degree of hydronephrosis was classified according to the Society of Fetal Urology (SFU) grading system into mild hydronephrosis (SFU I-II), moderate hydronephrosis (SFU III) and severe hydronephrosis (SFU IV). 9
Procedure
Intravenous third generation cephalosporin was given at the time of induction of general anesthesia. A 4–6 French open tip ureteric catheter was inserted by cystoscopy in a dorsal lithotomy position. All patients were then positioned prone with padding of all pressure sites. Opacification of the renal collecting system was done by iodinated contrast in a retrograde fashion under fluoroscopy. An 18 gauge puncture needle was advanced into the selected calyx under fluoroscopic guidance. The nephrostomy tract was acutely dilated by Amplatz Teflon dilators up to 20 Fr (acute dilatation is defined as one-shot dilatation). 10 Pediatric nephroscope (18 French Wolf) and pneumatic disintegrator were used for all patients. At the end of the procedure, a 14 Fr percutaneous nephrostomy tube (NT) was inserted and sutured to the skin. In addition to that, the ureteric catheter was fixed to an indwelling Foley’s catheter. The operative time was calculated from the time of first renal puncture until skin suture.
Postoperative care
All patients had a CBC, serum creatinine, abdominal US assessment in the morning after surgery. In addition, plain X-ray or NCCT imaging were done in cases of radio-opaque or radiolucent stones respectively. Success was defined as patients who have no residual stones as detected by intra-operative endoscopy and X-ray or post-operative abdominal ultrasound and NCCT. The nephrostomy tube and the ureteric catheter were removed the second day provided that no intraoperative perforation and no significant residuals as detected by postoperative imaging. Patients were then discharged and were instructed to return to the hospital if they have a fever, vomiting, worsening pain or a persistent leakage from the nephrostomy tract for more than 2 days.
In the second follow up visit after 2 weeks, patients had repeated serum creatinine, CBC and the abdominal US. Patients were followed for 3 months for repeated imaging as indicated. Complications were categorized according to the modified Clavien–Dindo classification system.
Outcomes
The primary outcome is to study the complications associated with the short LOS.
The secondary outcome is to study the predictors of the LOS.
Statistical analysis
The statistical analysis was carried out with SPSS software (Statistical Package for the Social Sciences, version 26, SSPS Inc, Chicago, IL, USA). Frequency tables with percentages were used for categorical variables and descriptive statistics (median, and range) were used for numerical variables.
Mann–Whitney U test was used for data that wasn’t normally distributed. Chi-square (χ2) test and Fisher’s Exact Test were used for comparison of qualitative variables as appropriate. Binary logistic regression was used for the predictors of LOS. A p-value of less than 0.05 was considered statistically significant.
Results
The study included 220 pediatric patients with a median (range) age of eight (Range: 3–17) years. Baseline patients’ demographics and stone criteria were presented in (Table 1).
Baseline stone and patients’ criteria.
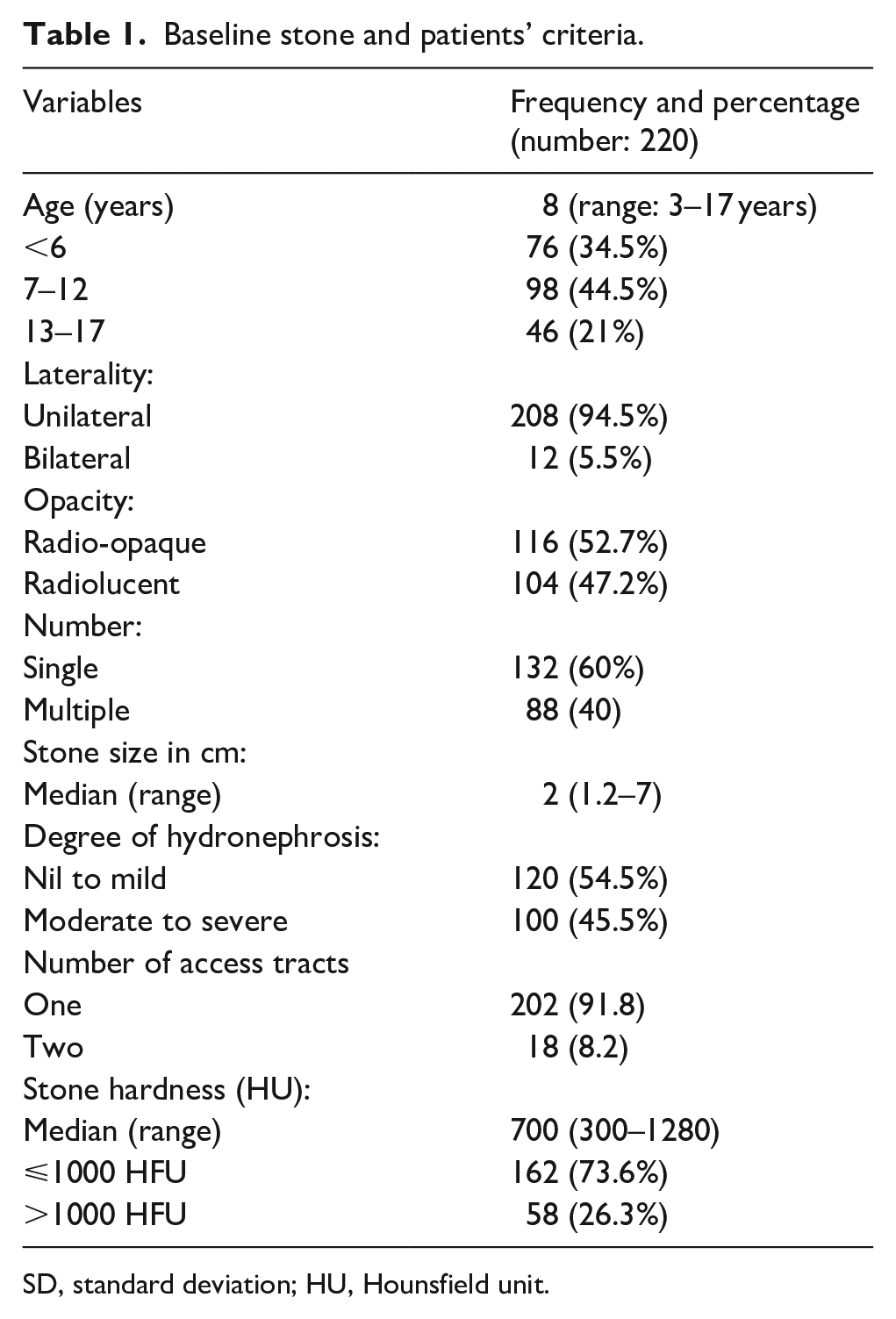
SD, standard deviation; HU, Hounsfield unit.
Outcomes
PNL was performed for 220 renal units. Stone free rate was achieved in 200 patients (91 %) of patients, while residual fragments were detected in 20 patients (9%); stones passed spontaneously in 8 patients, ESWL was performed for 10 patients, while ureteroscopy was needed in two patient due to migrated retained stones in his ureter associated with pain and hydronephrosis. The median operative time was 35 min (Range: 14–76).
Regarding the complications, they were reported in 50 (22.7%) patients. Minor complications (grade 1 and 2) were detected in 42 (19.1%) patients, while grade 3 complications were reported in 8 (3.6%) patients. Concerning the minor complications, 20 (9.1%) patients suffered hematuria and a slight drop in their Hemoglobin level. Twelve (5.5%) patients had a fever of more than 48 h which was controlled by antibiotics. Six (2.7%) patients needed a blood transfusion due to intraoperative bleeding. In addition to that, four (1.8%) patients complained of urine leakage from the site of the nephrostomy tract which was resolved after 2 days. Concerning major complications, intraperitoneal perforation was encountered in eight (3.6%) patients for whom intraperitoneal drain and double J insertion were performed. Drains were removed within 1 week while double J stents were removed 4 weeks postoperatively (Table 2).
Perioperative complications according to Clavien–Dindo classification system.
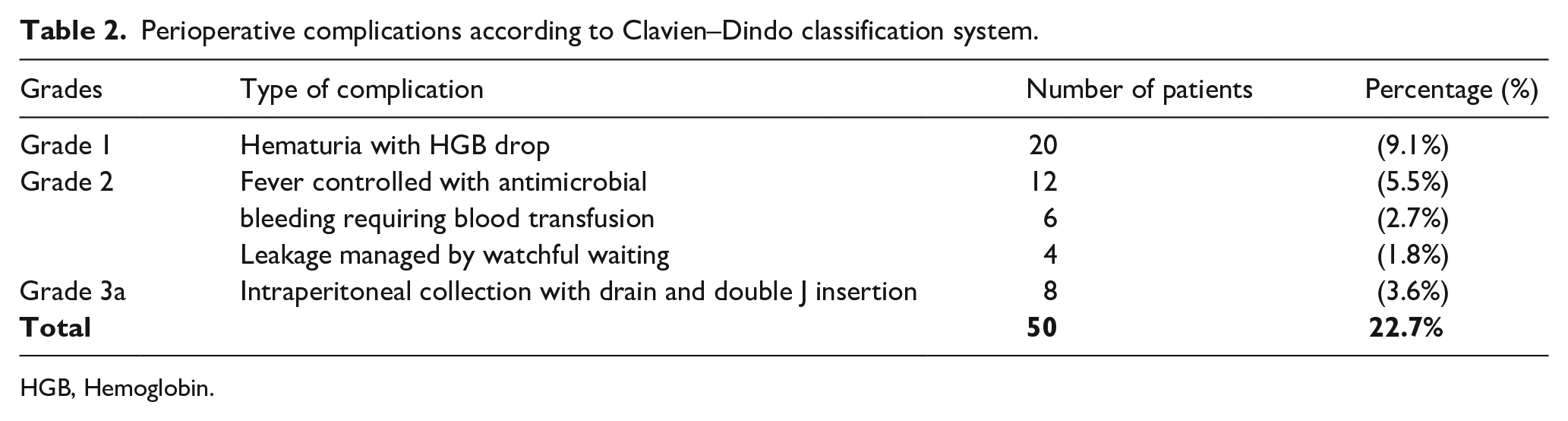
HGB, Hemoglobin.
In Table 3, 184 (83.6%) of patients stayed at the hospital for only 1 day, while 36 (16. 4%) stayed more than 1 day. Of 36 patients who stayed more than one-day, 34 had complications (p value <0.001). Other variables that could predict longer LOS are; younger patients’ age, larger stone size, stone multiplicity, the number of access tracts and the initial stone free rate (p values =0.002, <0.001, <0.001, <0.001, and 0.03 respectively). On multivariate analysis, there was a strong evidence the longer LOS is strongly related to the complications (p value <0.001). There was no strong association between the LOS and other variables (Table 4).
The association between stone criteria, patient criteria, outcomes and the length of hospital stay (number 110).
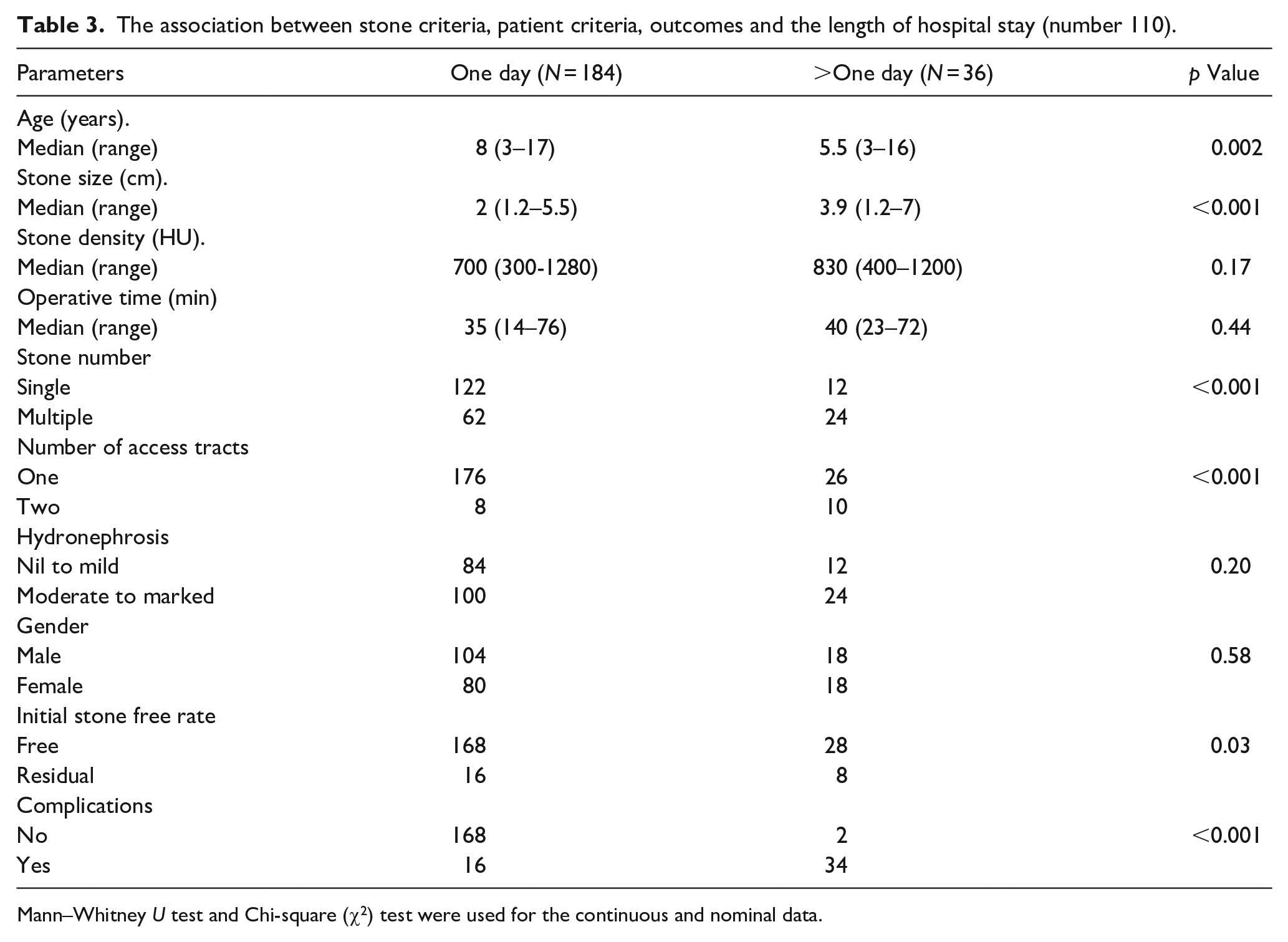
Mann–Whitney U test and Chi-square (χ2) test were used for the continuous and nominal data.
Logistic regression for the predictors of length of hospital stay.
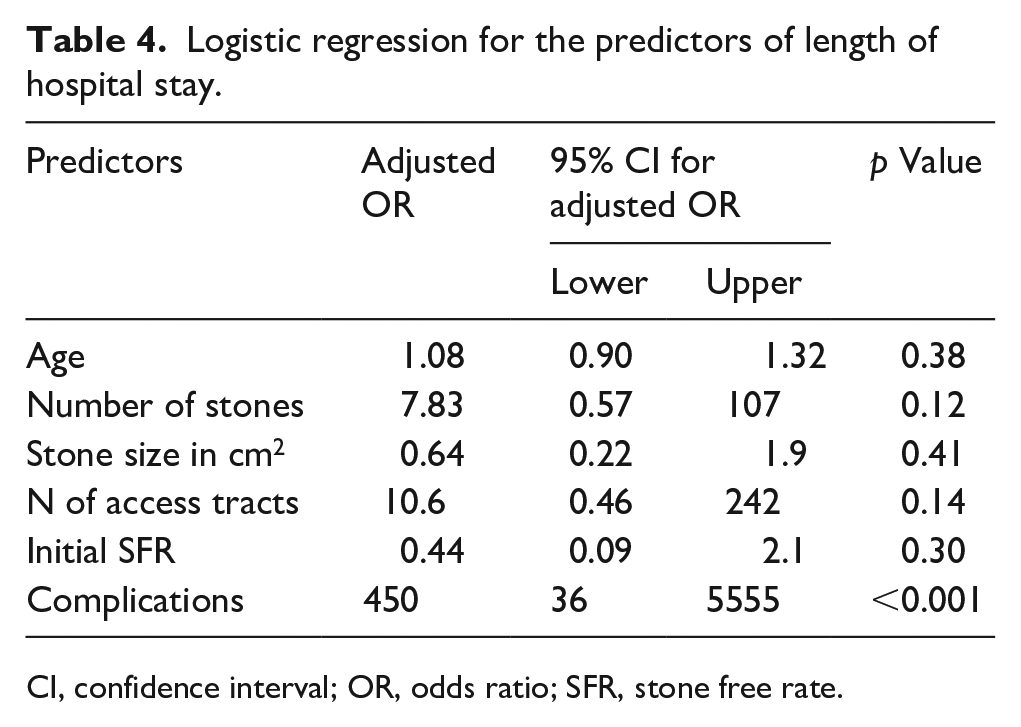
CI, confidence interval; OR, odds ratio; SFR, stone free rate.
Discussion
This study demonstrated the safety of one-day LOS after pediatric PNL. The nephrostomy tubes were removed and the patients were discharged the second day in most of our patients. There was a strong evidence that the longer LOS is associated with the surgical complications.
Surgical management of urinary tract stones has been revolutionized during the last two decades after the introduction of minimally invasive techniques. Whereas ESWL is often used as a first-line treatment for pediatric calculi, it is not suitable for large stone size or dilated obstructed urinary tract. Therefore, percutaneous nephrolithotomy could be considered the contemporary method of treatment for pediatric calculi. We believe that one of the major advantages of ESWL is that it is a 1-day procedure compared to an average of 2–6 days LOS in PNL. Other studies used tubeless PNL to reduce hospital stay and post-operative pain. However, this is suitable for selected patients with simple PNL procedures.6–8
We studied the feasibility of a short hospital stay after pediatric PNL. We adopted this strategy because of its economic impact and to decrease the risk of hospital-acquired infection. Besides, early nephrostomy tube removal can have the same advantages of tubeless PNL, as well as the other benefits of nephrostomy tube like better drainage, tamponade of the nephrostomy tract, healing of extravasation and the feasibility for second look PNL. In 2012, Alyami and Norman 11 studied the feasibility of overnight hospital stay after adult PNL. They documented the safety of early nephrostomy tube removal. Surgical complications and stone free rate were statistically significant predictors of LOS in their study. In our study, surgical complications were the only predictor of longer LOS.
Despite the association between longer LOS and the surgical complications, younger patients’ age, larger stone size, stone multiplicity, the number of access tracts and the initial stone free rate on bivariate analysis, the surgical complications were the only predictor on multivariate analysis. Other factors may be related to the risk of complications. The percentage of the overall complications in our study was 22.7%. Complications rate of 10% to 36.3% had been reported by other studies, which included minor complications in (8%–20%) versus severe complications in (2%–16%) of patients.12,13 Predictors of complications were studied by a previous multicenter retrospective analysis. That study reported that the operative time, sheath size, mid calyceal puncture, and partial staghorn stones were statistically significant parameters affecting the complication rates. 14
In the literature, different studies analyzed the predictors of individual complications. For instance, a multicenter study that was done in Turkey documented that younger age, right-sided PNL, staghorn stones, mini-PNL, longer operative time and blood transfusion were risk factors for febrile urinary tract infection. 15 The use of multi-tract was found to be an independent factor of complications in a study that was done by Gonen et al. 16 Moreover, another study focused on the predictors of bleeding during pediatric PNL. They reported that the body mass index, stone size, stone position, operation time and the degree of preoperative hydronephrosis were statistically significant parameters. 17 In an interesting study, the stone kidney index (SKI) was found to be a statistically significant predictor of SFR and the overall complications rate. SKI was calculated by dividing the length of the stone along its longest axis by the length of the kidney along its longitudinal axis. 18
Stone free rate in our study was achieved in 89% of our patients. This was comparable to that reported in other studies.12,19 Even though, some studies reported a lower SFR. 20 The predictors of the stone-free rate after PCNL were studied in literature. To illustrate, Shahror, K, et al. reported that the stone size, number, location, and pelvicalyceal system anatomy were significant predictors of SFR. Furthermore, the complexity of the stones and the usage of a single tract were also considered as predictors of low SFR in another study. 21 We should emphasize that the average stone size in our study is relatively smaller compared to the literature.
It worth mentioning the limitations of our study which are its retrospective design and the lack of control group.
Conclusion
Early nephrostomy tube and 1-day length of hospital stay could be a safe option after pediatric PNL. Surgical complications are the only indications for longer hospital stay. Randomized control trials are recommended to study this regimen.
Footnotes
Acknowledgements
I would like to acknowledge my patients for their contribution in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.