
Abstract
Background:
Cytoreductive radical nephrectomy (cRN) with immunotherapy is the treatment of choice in patients with metastatic renal cell carcinoma (mRCC). Limited data are available on the role of cytoreductive partial nephrectomy (cPN) in mRCC. This study is a systematic review and meta-analysis of the evidence regarding survival rates comparing cPN versus cRN.
Methods:
PubMed/Medline, Scopus, Google Scholar, EMBASE, and the Cochrane Library were reviewed in December 2021 according to PRISMA. Four articles including 2669 patients were selected to enroll in the study. The identified reports were reviewed and their methodological quality was subjected to total quality assessment. The outcomes were cancer specific survival (CSS) and overall survival rate (OS).
Results:
Totally 2669 patients, 542 in cPN and 2127 in cRN groups enrolled in final analysis. Of the preoperative data, there were significant differences in preoperative size of tumor between cRN and cPN patients (p < 0.001), however Fuhrman grades were comparable between groups (low grade: p = 0.51, high grade: p = 0.76). There were comparable results in 1-year (p = 0.07), 2-year (p = 0.08), and 3-year (p = 0.71) CSS rates between cPN versus cRN. There was no significant difference between cPN versus cRN in OS rate (p = 0.61).
Conclusion:
There are comparable results between cPN and cRN in CSS and OS rate. However, due to a lack of data, future study will need to do more extensive studies using prospectively recorded patient features to evaluate the cPN and cRN in the metastatic setting.
Introduction
Renal Cell Carcinoma (RCC) accounts for around 2%–3% of all adult cancers. 1 One-third of newly diagnosed RCC patients may acquire metastatic disease, whereas 20%–40% of individuals with clinically localized RCC develop metastatic cancer. 2 Although the introduction of immunotherapy increased progression-free survival and, in rare cases, sustained clinical responses in metastatic RCC,3,4 long-term findings revealed only a 10%–20% response rate and a less than 5% 10-year survival rate. 5
Founding a poor prognosis in advanced RCC has sparked a significant amount of study in the hopes of discovering methods to enhance long-term survival rates, such as immunotherapy and surgical combinations. The role of cytoreductive radical nephrectomy (cRN) in combination of interferon has been proved3,6 but lessons from outcomes of partial nephrectomy (PN) in localized RCC, create a new concept that whether cytoreductive PN (cPN) could be consider in management of mRCC. The necessity for additional potentially nephrotoxic treatments in metastatic condition makes the maintenance of renal function even more important. Aside from renal function preservation, further advantages of PN may include better postoperative performance status, elimination of paraneoplastic symptoms, and eradication of the source of future metastases. 7
Till now only few studies, evaluate the outcomes of cytoreductive partial nephrectomy in mRCC patients and the data are scarce. As our knowledge, this is the first systematic review and meta-analysis which conducted to shed the light on the role of cPN on mRCC patients.
Methods and materials
This systematic review and meta-analysis conducted in December 2021 in multiple databases. The Preferred Reporting Items for Systematic Reviews and Meta-analyses criteria (www.prisma-statement.org) was used for the study design, search strategy, data abstraction (Table 1). Only articles written in English were chosen to enroll.
Study design.
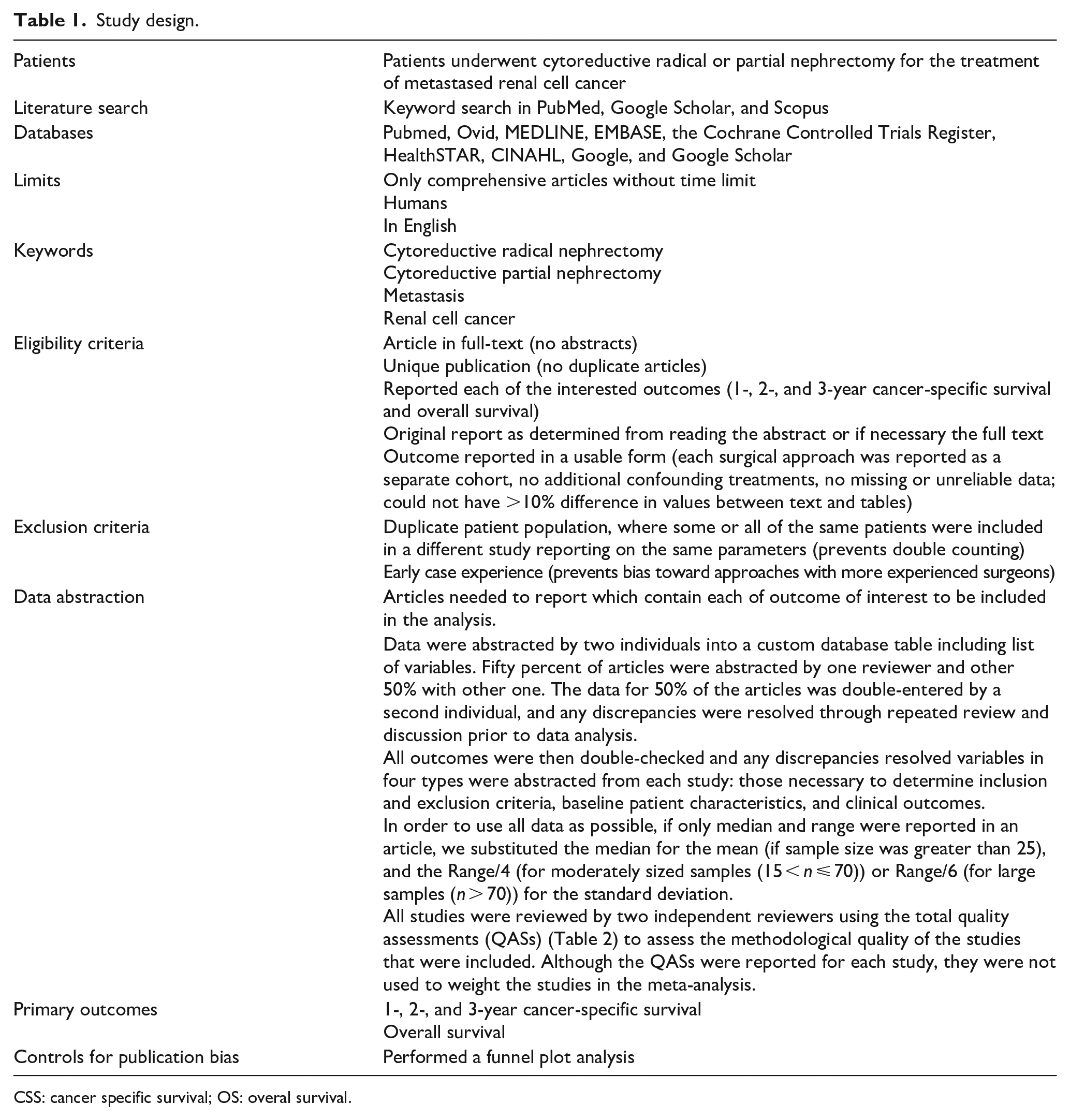
CSS: cancer specific survival; OS: overal survival.
Original articles reporting on cytoreductive treatment of renal cell carcinoma were selected and conference abstracts because of lack of data were not enrolled in peer review.
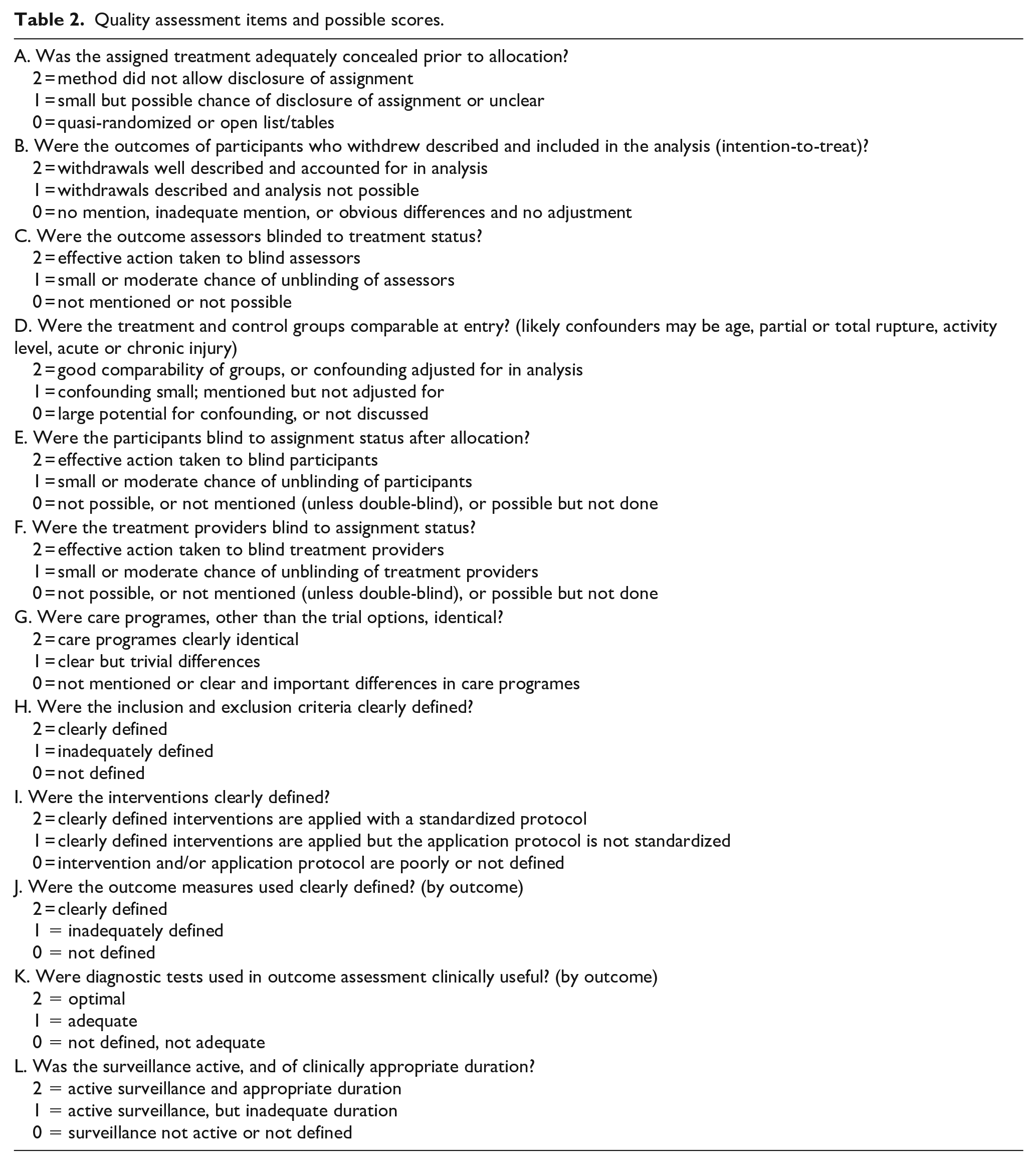
Total quality assessment (QAS) was used to assess the methodological quality of the studies, by two independent reviewers. However, QASs scores, were not used to weight the studies in the meta-analysis (Table 2).
Quality assessment items and possible scores.
All the data extracted by two independently authors and agreement reached after discussion. For any disagreement, consultation with the senior authors performed. The data collected from all manuscripts regarding treatment groups included the cytoreductive nephrectomy surgical approach (partial vs radical), publication year, duration of follow-up, patient characteristics (number, age, gender, tumor size, Furman grade, histology), cancer specific survival (CSS), and overall survival rate (OS).
Statistical methods
The meta-analysis done with the Review Manager version 5.2 (downloaded from http://community.cochrane.org/tools/review-production-tools/revman-5). Mean and standard deviation (SD) was considered for continuous data and proportions or risks and the treatment effect which reported as odds ratios (OR) with a 95% confidence interval (95% CI) were used for dichotomous data. If only median and range were reported in an article, the median was substituted for the mean when the sample size was greater than 25. For SD, range/4 (for moderately sized samples (15 < n ⩽ 70)) or range/6 (for large samples (n > 70)) were used. 8
Chi-squared test and I2 statistic were used to assess the Heterogeneity between studies and p-value of <0.1 and an I2 value >50% were considered as statistical heterogeneity, prompting a random-effects modeling estimate. A non-significant chi-squared test result (p ⩾ 0.1 and I2 ⩽ 50%) suggested that there was no evidence of heterogeneity and a Fixed-Effect model was used. Publication bias also showed in Funnel plots, and the more asymmetric the funnel plot was, the higher the potential bias was.
Results
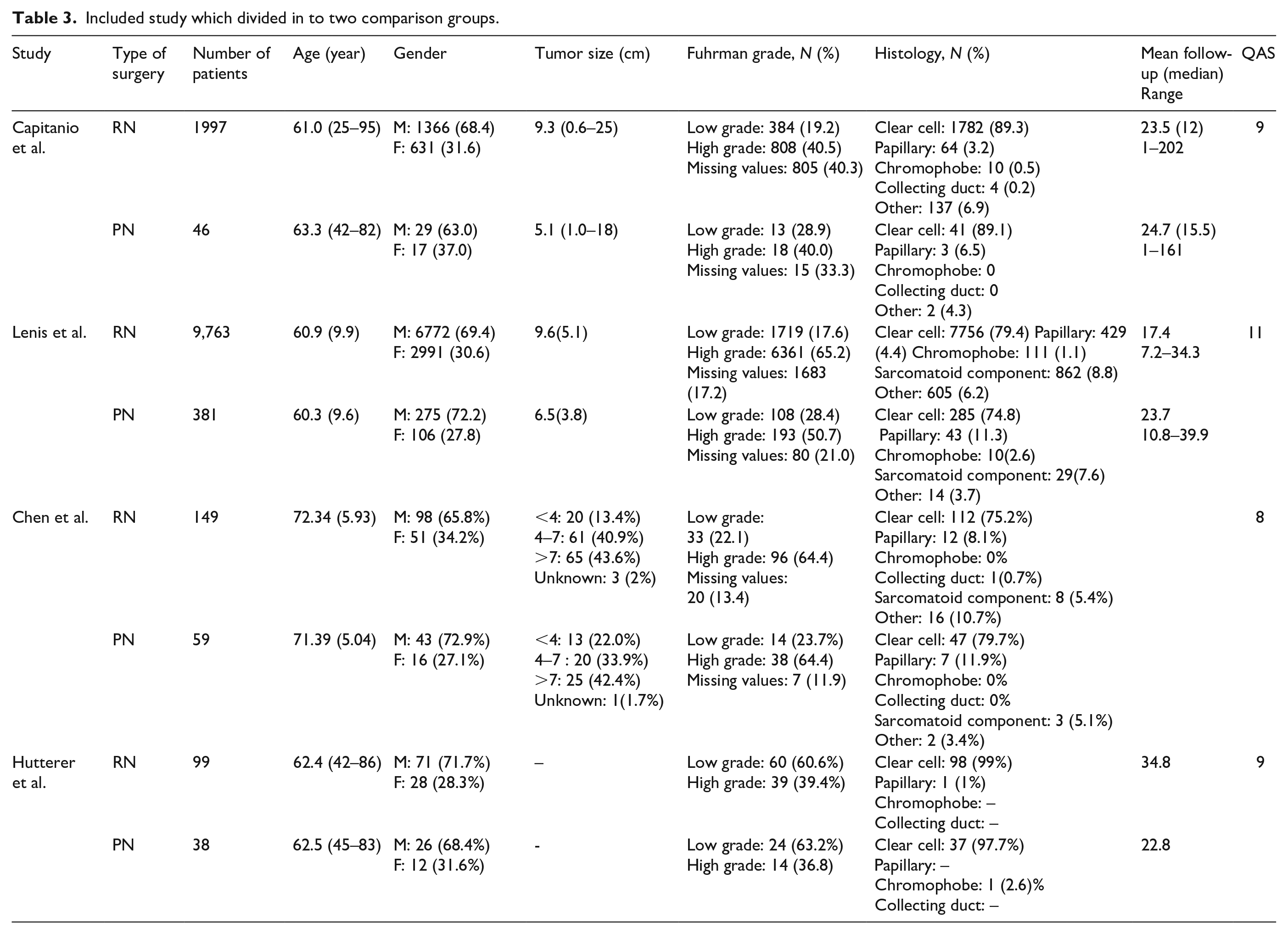
This systematic review and meta-analysis four articles included 2669 patients, 542 undergoing cPN, 2127 undergoing cRN (Table 3). Of the preoperative data, there were significant differences in preoperative size of tumor between cRN and cPN patients (p < 0.001), however Fuhrman grades were comparable between groups (low grade: p = 0.51, high grade: p = 0.76). Clear cell carcinoma was the commonest post-operative pathology with no significant difference between groups (p = 0.83)
Included study which divided in to two comparison groups.
Cancer specific survival rate
There was no significant heterogeneity between studies in 1-year CSS (I2 = 0%; p < 0.51, Figure 1), but in 2- and 3-year CSS significant heterogeneities between studies were found between cPN and cRN methods (I2 = 84%, 81%; p = 0.01, 0.02); thus, fixed effect for 1-year CSS and random effect were used to analyze 2- and 3-year CSS. There were comparable results in 1-year (OR: 0.1; 95% CI: −0.01 to 0.21; p = 0.07; Figure 2), 2-year (OR: 1.61; 95% CI: 0.94–2.75; p = 0.08; Figure 2), and 3-year CSS rates between cPN versus cRN (OR: 1.28; 95% CI: −0.34 to 4.88; p = 0.71; Figure 2).
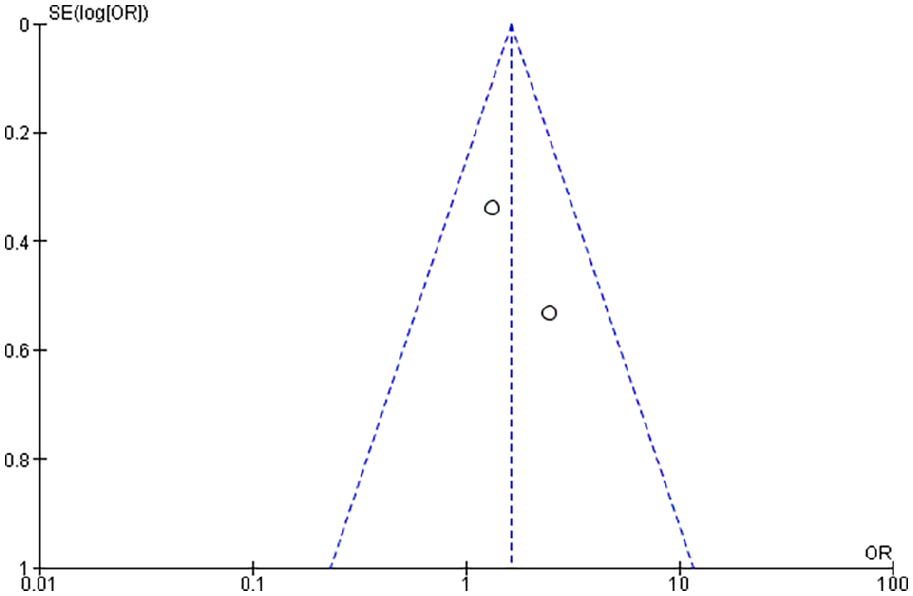
Funnel plot of 1-year cancer specific survival rate showed no significant heterogeneity between cytoreductive partial versus radical nephrectomy.
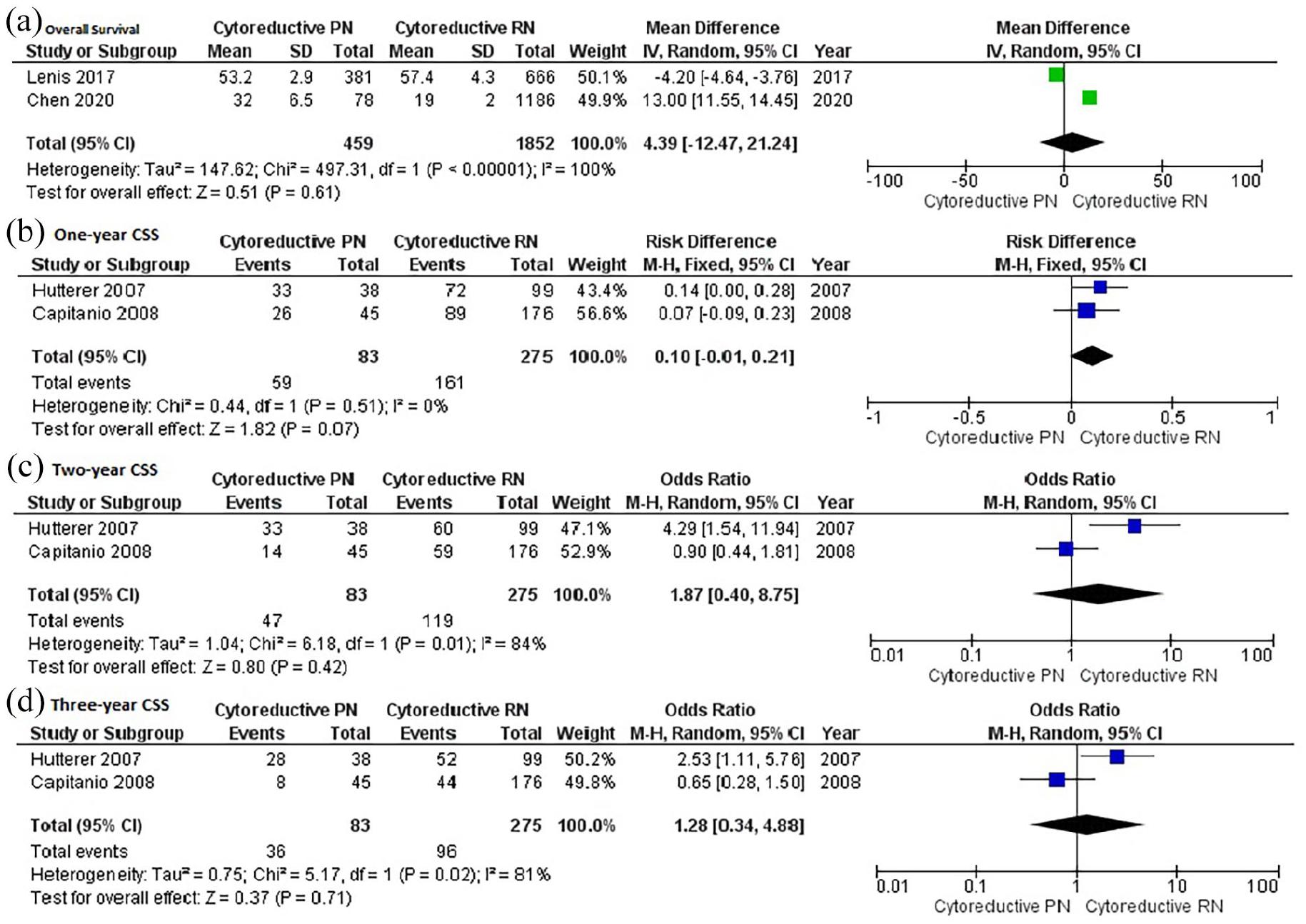
Forest plot of overall survival (a), 1-year (b), 2-year (c), and 3-year (d) cancer-specific survival rates showed no significant difference in patient underwent cytoreductive radical versus partial nephrectomy in treatment of metastatic renal cell carcinoma.
Overall survival rate
There was significant heterogeneity between studies in OS rate (I2 = 100%; p < 0.001). Therefore, random effect was used to analyze. There was no significant difference between cPN versus cRN in OS rate (OR: 4.39; 95% CI: −12.47 to 21.24; p = 0.61; Figure 2).
Discussion
This systematic review and meta-analysis is the greatest collection of thorough research on cytoreductive partial versus radical nephrectomy to date. Because of the lack of randomized clinical trials, variations in patient characteristics between surgery cohorts may explain disparities in results between treatment groups. Statistical techniques cannot adequately correct these disparities. Furthermore, unidentified discrepancies in the characteristics of the patients and physicians, as well as the therapies used, may contribute to the varied outcomes between trials. Caution is suggested when interpreting the findings of this meta-analysis in light of the above factors.
Traditionally, cRN with immunotherapy was the treatment of choice for mRCC patients. Nowadays, the concept of cytoreductive partial nephrectomy has gain a power in status of metastasis. The efficacy and safety of cPN have been called into doubt due to concerns about its technical difficulties, risk of complications, and unclear survival benefits over cRN.
The main goal in treatment of cancer is disease control. Our study showed cPN has a comparable result in CSS compared to cRN during 3-year follow-up. We supported the findings of Capitanio et al, 9 and Hutter et al. 7 studies. However, Hellenthal et al. 10 noted the patients who underwent cPN had a 0.49 reduced chance of dying from RCC than those who had cRN. This discrepancy might be due to limitations of their study respectively. The patient in cPN group had a significantly smaller tumor and this decreased overall tumor burden in cPN group which is known to impact survival rates in mRCC patients could affect the survival rate. 11 It is predictable that patients with a single and resectable metastasis are expected to have higher cancer-specific survival than those with many and unresectable metastases, and possibly, patients treated with cPN may have had a more favorable metastatic profile than RN patients. Furthermore, the lymph node status is a substantial predictor of failure to achieve either an objective immunotherapy response or an increase in survival when immunotherapy is employed as an adjuvant treatment. Therefore, to investigate the absolute equivalency of PN and RN in the metastatic patient, additional extensive evaluations with prospectively documented patient data are unquestionably required.
Considering the preservation of renal function, and as consequence expecting higher overall survival rate, cPN has got more preference in the treatment of mRCC. Our findings showed no difference between OS rate between cPN compared to cRN. In contrast, Lenis et al. 12 showed that patients who underwent cPN had a 19% lower risk of dying from any cause than those who received cRN. However, when they stratified the data by tumor size, they found this benefit to be isolated to small renal tumors (less than 4 cm). Chen et al. 13 also showed survival advantage of patient who underwent cPN versus cRN. After subgroup analysis they also confirmed that OS was superior only in male patients with ⩽7 cm tumor, N0 and isolated metastasis and even in the N1 stage, cPN results was worse than cRN. Recently published study 12 showed the treatment in high-volume center, papillary and chromophobe histology, and more recent year of treatment were all associated with higher chance of receiving a cPN. Conversely, age ⩾80 years, no medical insurance, high tumor grade, and 4–7 cm tumor were all associated with decreased odds of receiving acPN. Therefore, this discrepancy between our findings and above studies might be because of heterogeneity and selection bias between the studies. Furthermore, mostly the benefit of cPN in OS is in small sized tumor and because of the lack of data we couldn’t analyzed the survival rates in order of size of tumor and other independent factors like as performance status and laboratory results (hemoglobin, LDH, calcium). 14
This meta-analysis contained the biggest sample size of comprehensive studies that evaluated the two surgical procedures for treatment of metastatic RCC in terms of survival rate results. Nevertheless, there were some limitations. The only English literatures were included. Studies that did not identify the mean and SD approximated them using the median and range, which may have deviated somewhat from the true numbers. Due to lack of data, we were not able to do sub-group analysis in order to tumor size, grade, performance status, comorbidities, prior systemic therapy, and laboratory results which all may affect the survival rates.
Conclusion
The results of this meta-analysis should be considered with care in light of the concerns previously mentioned. The quality of the papers included influences the quality of the outcomes of systematic reviews and meta-analyses. As the quality of the studies included in the current analysis was assessed using a questionnaire, it was discovered that some studies were of poor quality, and a well-powered study with a large number of candidate articles is recommended to better compare the outcomes of the two surgical approaches. Future trials with more extensive analysis and prospectively documented patient data are undoubtedly necessary to assess the PN and RN in the metastatic situation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.