
Abstract
Aims and objective:
Percutaneous nephrolithotomy (PCNL) is treatment of choice now a days in patients with spinal deformity with large kidney stones. Objectives of our present study to compare in which position it is better to perform and costs minimum complications after surgery.
Methods:
A total of 14 patients with spinal deformity having nephrolithiasis were selected randomly. No preferences for age, gender, size, location, and laterality of stone or BMI. All the patients were fit according to AUA guideline criteria for management by PCNL. Preoperative and postoperative data were collected in all operated patients. Descriptive statistics were performed as means, standard deviations, and ranges using Microsoft excel. For categorical variables percentage were used.
Results:
A total of 14 patients with spinal deformity having nephrolithiasis underwent PCNL. Seven patients operated in prone position and seven patients operated in modified supine position within approximately 2 years. As compared to prone position in supine position there were reduced operative time, little or no change in Hb concentration, shorter hospital stay, little intraoperative blood loss, and higher significant stone free rate were detected.
Conclusions:
Supine PCNL in spinal deformity patients with nephrolithiasis is an alternative to the standard prone PCNL. It provides an additional benefit of large operative field performing the procedure in a single position, reduces total operating time, less anesthesia related complications, less neuromusculoskeletal injury, and reduce physical strain on operating surgeon.
Keywords
Introduction
Patients with abnormal body habitus because of spinal deformities present a challenge for anesthesiologists and surgical procedures to perform. 1 In these patients, management of urolithiasis may be difficult because of restrictive lung capacity. Stone size not the only factor in deciding the best treatment plan. Patients with spinal deformities have systemic involvement including cardiac, genitourinary, pulmonary, and neurologic anomalies and the management of urolithiasis is challenging in these patients due to anatomic variations and cardio-respiratory dysfunction.2,3 In patients with spinal abnormalities open surgery, extracorporeal shock-wave lithotripsy (ESWL), percutaneous nephrolithotomy (PCNL), retrograde intra renal surgery (RIRS), and a laparoscopic approach are the possible interventions for the treatment of renal calculi. 4 Percutaneous nephrolithotomy as monotherapy has advantages in removing large stones and achieving excellent results with minimal morbidity even in difficult cases, such as those involving renal anatomic variation, children or morbidly obese patients, spinal deformity, previous renal surgery, solitary kidney, or renal failure.4,5
Supine position has advantages over prone position in improvement in anesthetic management, decreased intra renal pressure, decreased radiation exposure improved ergonomics of fluoroscopy, gain in extra operative field, improvements in patient positioning, shorter operative time, easier to do endoscopic combined intrarenal surgery or simultaneous bilateral endoscopic surgery, and improved endoscopic access to the upper pole from lower pole puncture tract.6 –8
There is still debate which position is better for PCNL in these patients. We performed PCNL in these patients in both prone and supine position and measures positive outcomes of supine position over prone position.
Materials and methods
This study was conducted in IPGME&R and SSKM hospital Kolkata, a tertiary care center in India between March 2020 and March 2022. Ethical clearance was obtained for this study from ethical standards of institutional research oversight committee on human experimentation with memo no. IPGME&R/IEC/2021/008. A total of 14 patients enrolled for this study having spinal deformity with nephrolithiasis. Out of 14 patients, seven patients were undergone prone position PCNL and remaining seven patients were undergone modified supine position PCNL. There were no preference for size, location, laterality of stones, or body mass index (BMI) of patients. All patients fit into the American Urological Association (AUA) guideline criteria for management of PCNL. All patients undergo clinical examination, basic biochemical tests and urine routine and microscopic examination and culture. All patients underwent initial radiological procedure as X-ray spine as shown in Figure 1, USG kidney, ureter and bladder (USG KUB) and contrast enhanced computed tomography of kidney, ureter, and bladder (CECT KUB) as shown in Figure 2. Seven patients were operated as standard percutaneous nephrolithotomy in prone position with dilation of tract up to 21 French and sheath size 22 French and remaining seven in modified supine position with dilatation of tract up to 21 French and sheath size of 22 French.
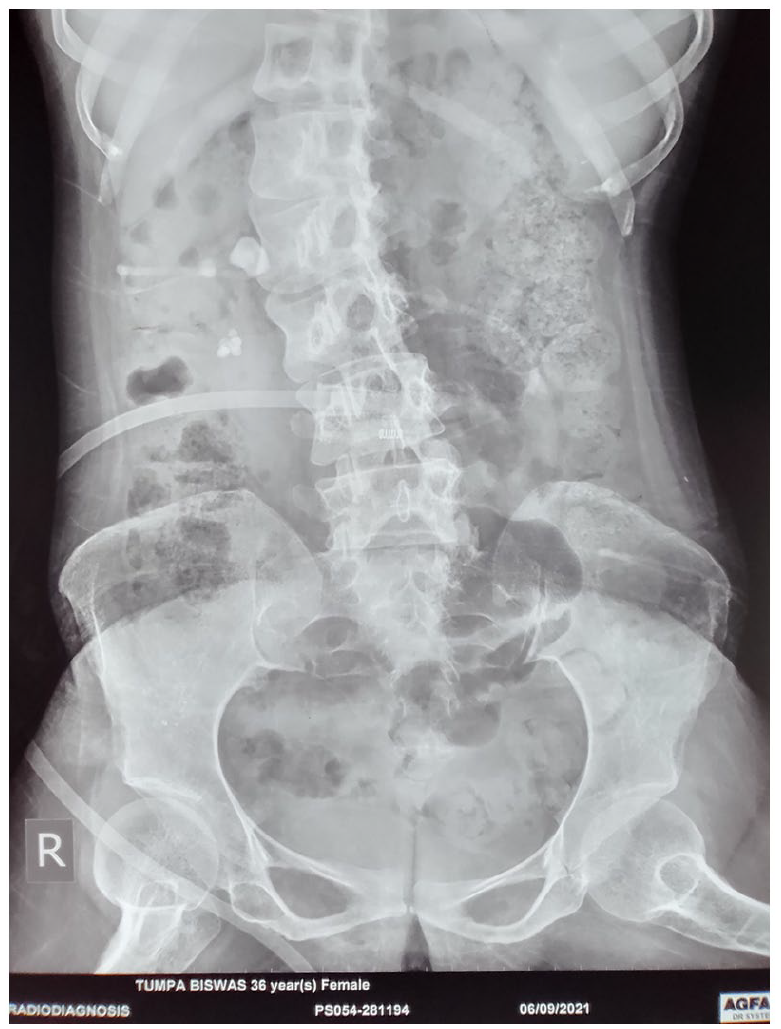
X-ray KUB showing right sided nephrolithiasis with PCN in patient of kyphoscoliosis.
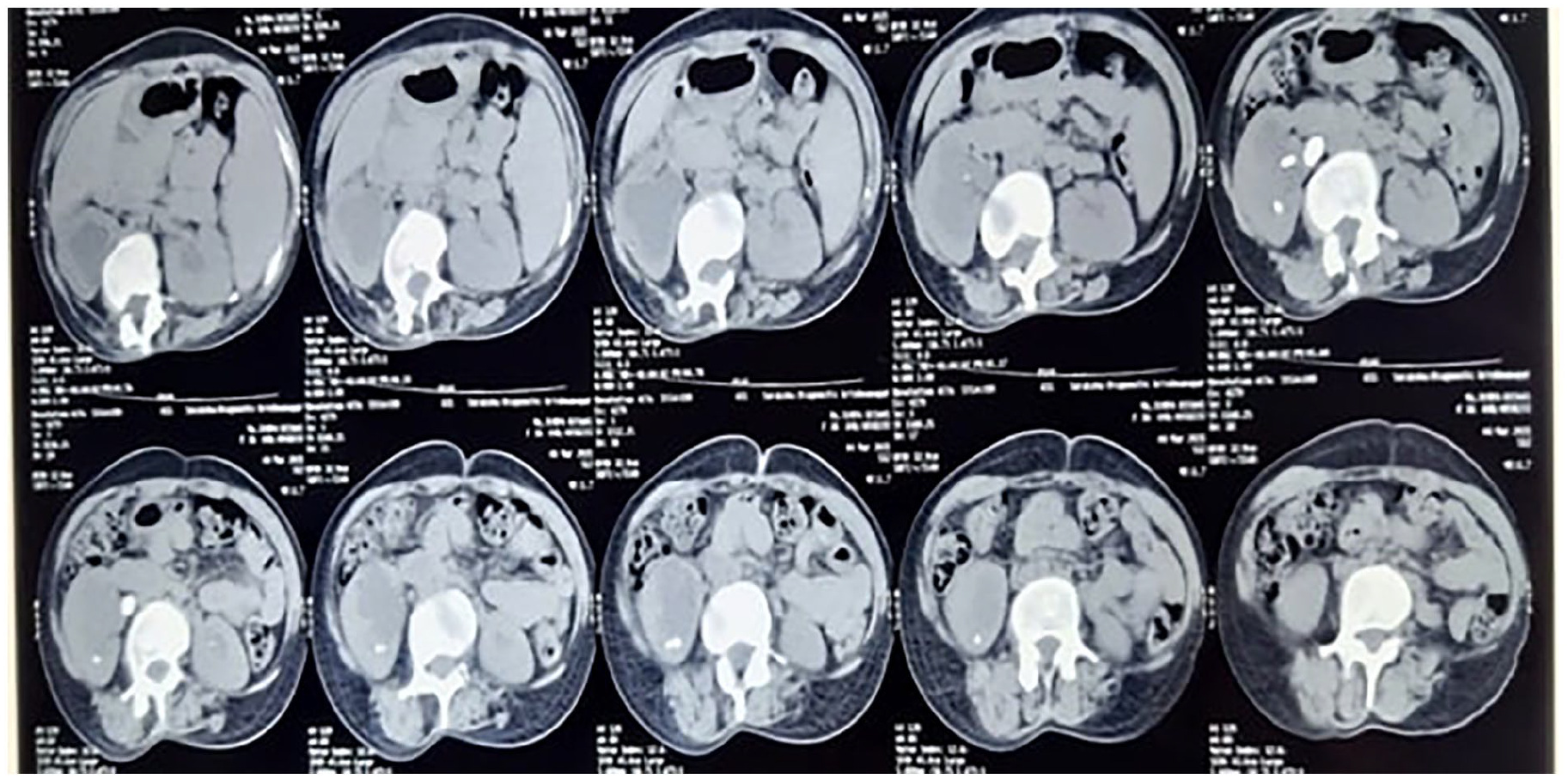
Axial section of CT scan showing rt. sided pelvic and lower pole calculi.
Surgical technique
We performed prone PCNL in seven spinal deformity patients by standard technique by using standard nephroscope and post operatively placed double J stent and clamped nephrostomy tube as tamponade effect for hemostasis.
We performed supine PCNL in seven spinal deformity patients as follows:
Under general anesthesia, the patient was placed in modified supine position lateral 15° tilt as shown in Figure 3. After positioning of patient we performed cystoscopy with 21 French/30° lens to insert ureteric catheter of 5 French followed by retrograde contrast study. Without changing the position of patient, a puncture of renal collecting system by initial puncture needle of 18G was performed under fluoroscopic guidance. We selected the middle pole calyceal puncture for middle pole calyceal stone and lower pole calyceal puncture for lower pole calyceal stone and upper pole calyceal stone as it is usually easy to access without any intra-operative complication. We introduced a guidewire of 0.032 inch through the initial puncture needle and tract was secured. Then tract was dilated serially up to 12 French by fascial dilators. Then alkine cannula over guidewire passed. Metallic guide rod was passed over guidewire and again tract was dilated by serial metallic dilatation up to 21 French, then 22 French amplatz sheath was followed over it as shown in Figure 4. After gaining the access to the collecting system a 20.8 French wolf nephroscope was introduced, stones were located and fragmented with help of an pneumatic lithotripter. Fragmented stones removed by tri prong forcep and remaining residual fragments were cleared by retrograde technique that is pushing water jet through ureteric catheter and also by shaking the sheath up and down and allowed fragments of stones to fall under gravity. Complete stone clearance was obtained. The C-arm was used to look for any residual fragments and confirmed that no residual fragments left. In all patients, double J stent of 5 French, 26 cm inserted in an antegrade technique. A nephrostomy tube was placed in all patients and clamped post-operatively as tamponade effect for hemostasis. Patients were followed up after 1 month with urine routine microscopy and culture report and X-ray KUB for confirmation of no residual stone left and for DJ stent removal as shown in Figure 5.
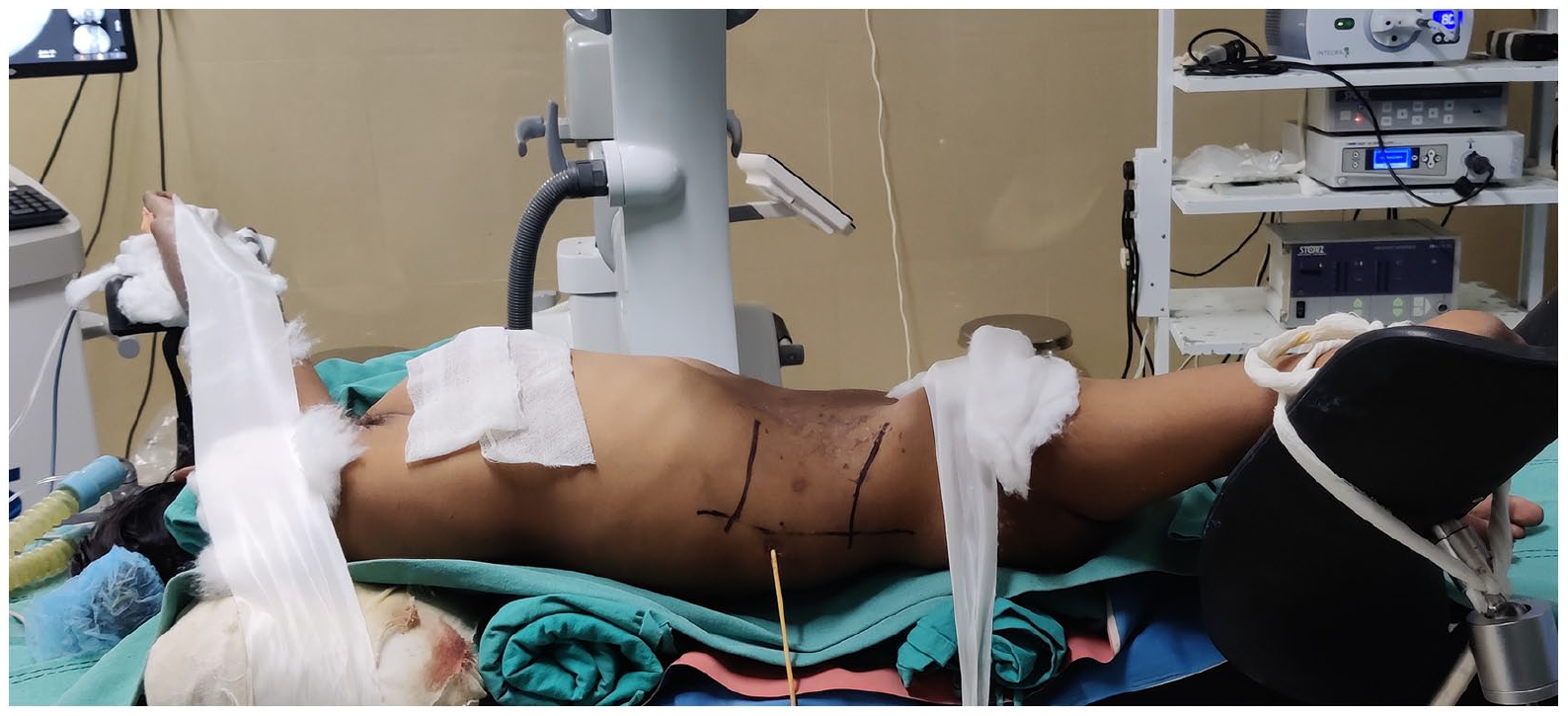
Intra operative modified supine position of patient during PCNL.
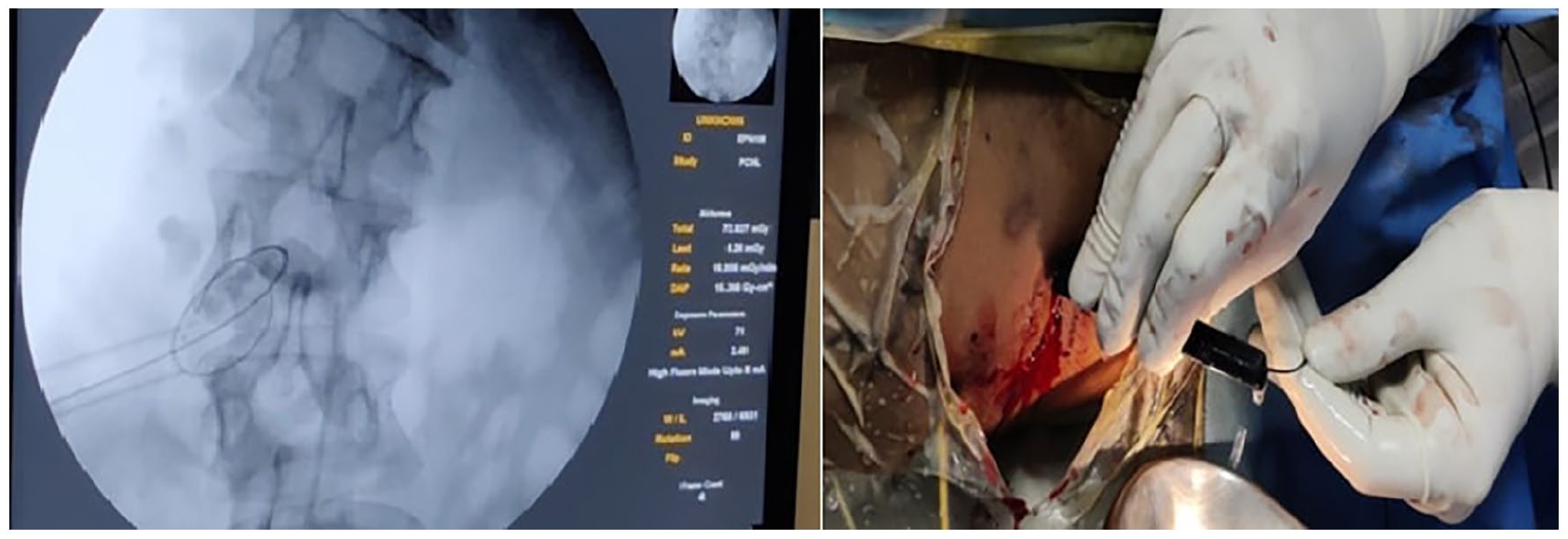
C arm view and surface view showing amlaz sheath with guidewire in lower calyx.

Post operative X-ray KUB showing right DJ stent in patient with severe kyphoscoliosis.
Results
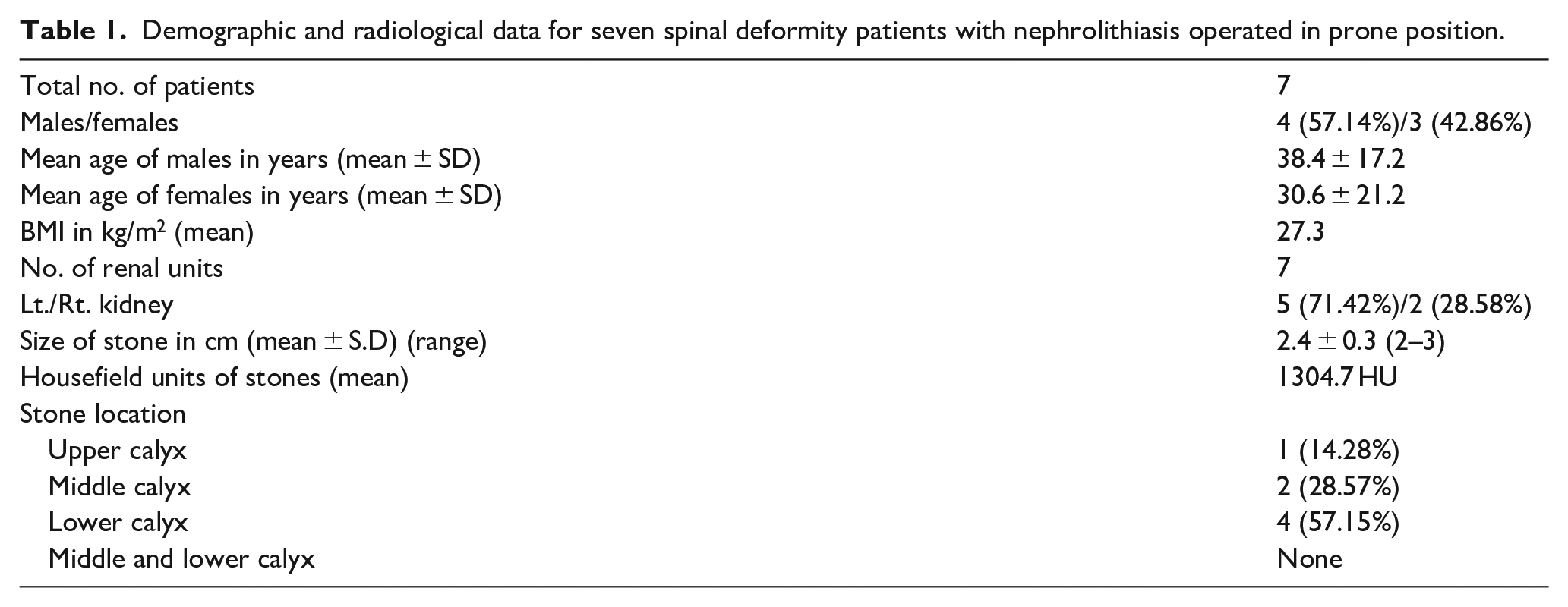
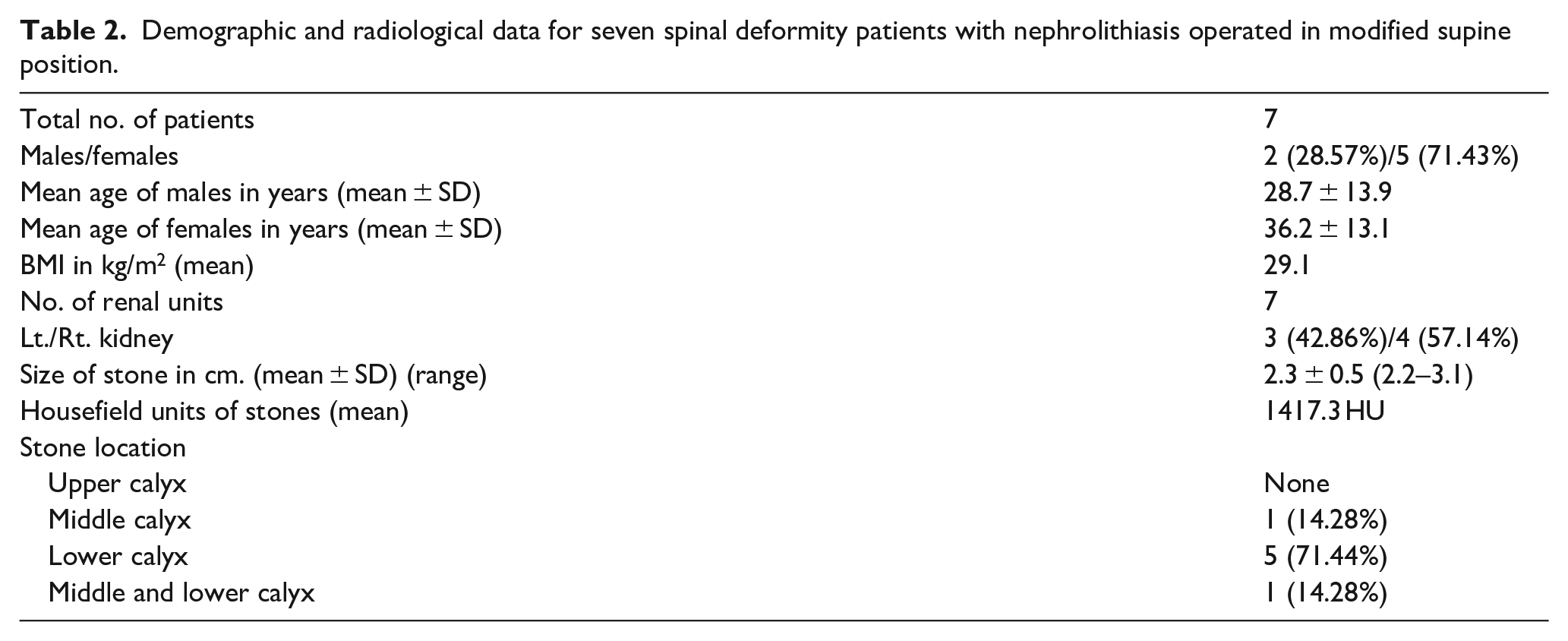
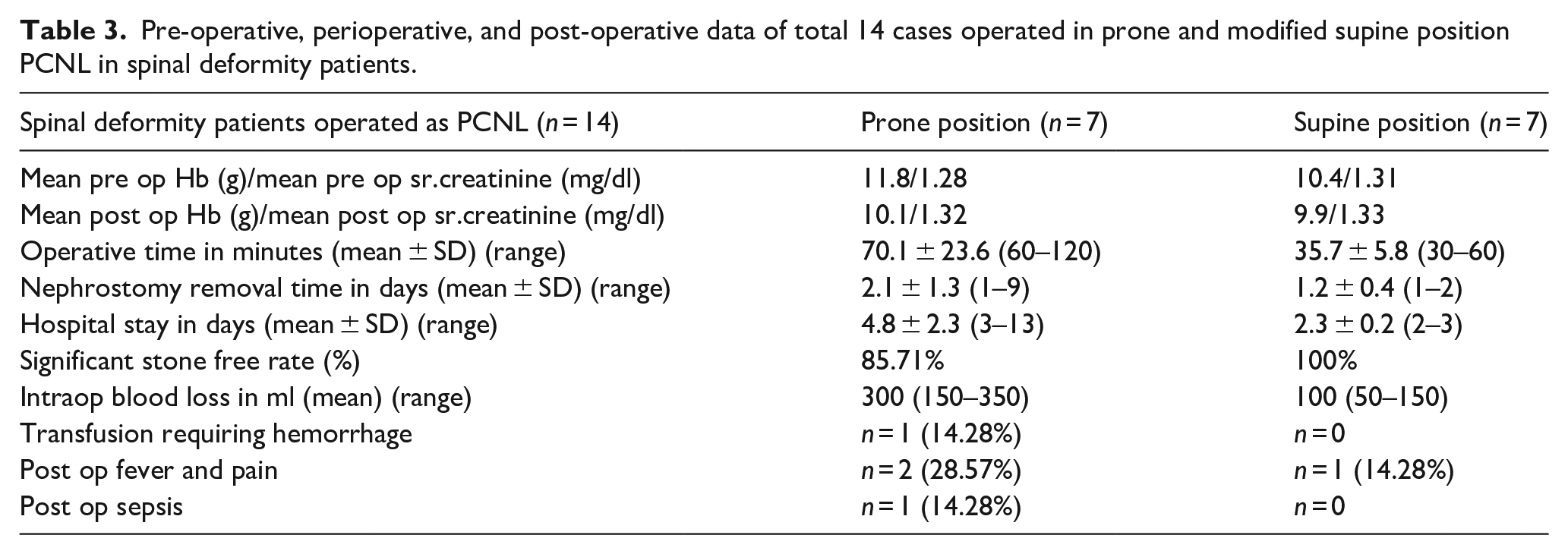
A total of 14 patients with spinal deformity underwent PCNL. Out of 14 patients, seven patients operated in prone position and another seven patients operated in supine position. A total male patients operated in prone position were four (57.14%) and female patients were three (42.86%). A total male patients operated in supine position were two (28.57%) and female patients were five (71.43%). Mean age of male and female patients operated in prone and supine position were 38.4, 30.6 years and 28.7, 36.2 years respectively. Mean BMI of patients operated in prone position was 27.3 kg/m2 and for supine position was 29.1 kg/m2. Mean stone size was 2.4 cm (SD ± 0.3) for patients operated in prone position and for supine position was 2.3 cm (SD ± 0.5). In prone position PCNL 71.42% operated on left kidney and 28.58% operated in right kidney. In supine position PCNL 42.86% operated on left kidney and 57.14% operated in right kidney. All patients underwent preferred calyceal puncture access as per location of stone. We generally avoid superior calyceal puncture in supine position and if stone in superior calyx decided to access superior calyx by inferior calyceal puncture only. In patients operated in prone position, upper calyceal puncture was done in 14.28%, middle calyceal puncture was done in 28.57%, and lower calyceal puncture was done in 57.15% patients. In patients operated in supine position, no upper calyceal puncture was done, middle calyceal puncture was done in 14.28%, and lower calyceal puncture was done in 71.44% and two simultaneous punctures in middle and lower calyx was done in 14.28% patients according to location of stone as shown in Tables 1 and 2. Mean operative time for prone position PCNL was 70.1 min (SD ± 23.6) and for supine position PCNL was 35.7 min (SD ± 5.8). There was 300 ml mean intra-operative blood loss operated in prone position patients (range 150–300 ml) and in operated supine position was 100 ml (range 50–150 ml). Average hemoglobin drop in prone position patients was by 14.45% and in supine position patients was by 4.80%. Average creatinine raised in prone position patients was 3.1% and in supine position by 1.52%. In postoperative period, one patient operated in prone position required one unit blood transfusion. There were in two patients (28.57%) developed fever in immediate postoperative period operated in prone position and one patient (14.28%) went into sepsis. Patients operated in supine position, only one patient (14.28%) had fever in immediate postoperative period relieved by medications but none went into sepsis. Stone free rate in prone position was 85.71% and in supine position was 100%. Patients operated in prone position had mean hospital stay 4.8 days (SD ± 2.3) (range 3–13 days) while patients operated in supine position had mean hospital stay 2.3 days (SD ± 0.2) (range 2–3 days) as shown in Table 3.
Demographic and radiological data for seven spinal deformity patients with nephrolithiasis operated in prone position.
Demographic and radiological data for seven spinal deformity patients with nephrolithiasis operated in modified supine position.
Pre-operative, perioperative, and post-operative data of total 14 cases operated in prone and modified supine position PCNL in spinal deformity patients.
Discussion
Spinal deformity is one of the challenge in medical field in anesthetic and surgical point of view. 1 Spinal deformity that is scoliosis, kyphosis, or kyphoscoliosis caused by idiopathic, congenital, or pathological disease of the thoracic, lumbar regions of the spine as shown in Figure 6. More than 80% of scoliosis cases are idiopathic and occurs in otherwise healthy people. Spinal deformities are generally associated with ankylosis of hip and tilt of pelvis. In addition, cardio-pulmonary function can be markedly affected in these.1,2 In the case of spinal deformity, restrictive lung disease develops with reduced lung volume, reduced total lung capacity and vital capacity of lung and so, impaired ventilatory function of lung develops which leads to ventilation-perfusion mismatch and atelectasis. Additionally in these difficulties with tracheal intubation were observed.2,3 Due to abnormal renal anatomy, recurrent urinary tract infections, restricted mobility, and urinary stasis the risk of urolithiasis is significantly increased in patients with spinal deformity.4,5

Female patient of poliomyelitis having severe kyphoscoliosis.
There are various options available for the treatment of renal calculi in spinal deformity patients like open surgery, ESWL, PCNL, RIRS, and laparoscopic procedures. Additionally, the effect of extracorporeal shock wave lithotripsy on hard stones (>1000 HU) or those size of >2 cm is unsatisfactory and also there are multiple sessions of RIRS required to achieve complete clearance in patients with stone size >2 cm in diameter.6,7 The management of kidney stones by PCNL has rapidly become the standard treatment of choice for size >2 cm over the last two decades. The position of the patient is crucial to perform PCNL, because the area of access is limited in prone position, especially in patients with abnormal body habitus. Furthermore, because of the spinal curvature, often associated with tilt and ankylosis of hip, it may get difficult for positioning the patient on the operating table. Sometimes it is necessary to keep patient to its natural decubitus while operating to avoid musculoskeletal trauma that is in the supine or lateral decubitus position.8,9
In this study we underwent PCNL in total 14 renal units with spinal deformity patients having nephrolithisis, out of which seven patients underwent by prone position and seven patients underwent by supine position. As compared to prone position in supine position there were detected reduced operative time, little or no change in Hb concentration, shorter hospital stay, minimum acceptable intraop blood loss, and higher significant stone free rate.
A PCNL study done by Izol et al. on spinal deformity patients with nephrolithiasis in prone position showed that in their study, the mean age of the patients was 30.7 ± 17.2 (5–62) years and the mean stone burden was 609.6 ± 526.9 (100–1800) mm2. The mean operative time was 76.6 ± 35.1 (35–150) minutes. At the end of the surgery, 13 (81.2%) of the patients were stone free. The overall success rate was 93.7% with the inclusion of two patients with clinically insignificant residual fragments. Complications (31.2%) included hemorrhage requiring a transfusion in two patients, prolonged urine leakage requiring double J catheter insertion in one, infection in one, and nephrectomy due to bleeding in one. Mean hospitalization time was 4.6 ± 2.4 (3–13) days. 10 As compared to their study in our study PCNL operated in supine position, patients had mean age of 32.45 years (SD ± 13.4), mean stone size was 2.3 cm (SD ± 0.5) (range 2.2–3.1), mean operative time was 35.7 min (SD ± 5.8) (range 30–60 min), at the end of surgery nearly 100% patients were stone free (excluding non significant fragments that was <3 mm). Mean intraoperative blood loss was 100 ml (range 50–150 ml) postoperative fever in 14.28% patients. No single patient required blood transfusion or developed sepsis.
Another study done by Goumas-Kartalas and Montanari performed four prone and four supine position PCNL in spinal deformity, In their study, mean operative time was 103 min (range 90–240 min) and hospital stay mean was 13.2 days (range 4–32 days). Overall blood transfusion required in 20% patients. One patient was converted to open surgery because of severe bleeding and one patient required angioemboilization. 11 Drawbacks of their study is that they could not mention about the which position was safe and effective to operate. As compare to their study in our study patients performed in supine position had mean operative time was 35.7 min (SD ± 5.8) (range 30–60 min) and mean hospital stay was 2.3 days (SD ± 0.2) (range 1–2 days). In our study no single patient needs blood transfusion operated in supine position and only one patient develops sepsis which was operated in prone position.
Another study done by Kara et al. in which they performed prone PCNL in scoliosis patients with nephrolithiasis. In their study operated in five patients, two were men and three were women and the mean age was 36.8 years (range 32–44) and the mean stone burden was 475 mm2 (range 400–1350). Operative and fluoroscopic mean time was 62.2 min (range 50–90 min) and 3.1 min (range 2–5 min) respectively. Of the five patients, three were stone free after PCNL. Auxillary procedures were required in two patients and second re-look PCNL in one and ureteroscopy in one. All five patients were rendered completely stone free after the final procedures. No severe complications either from anesthesia or the surgical procedure related were observed in the patients. Drawbacks of their study was sample size which was too small and not mentioned demographic and radiological data of stones. As compared to their study in our study PCNL performed in supine position had less total operative time, complete stone clearance in single setting and not required to do relook PCNL.
Till date there is limited studies has been done on spinal deformity patients with nephrolithiasis performed in supine position. We can conclude by this study is supine PCNL is safe, alternative treatment option with low complications rate, low morbidity to patients, and ergonomically better procedure to perform for surgeons compared to standard prone PCNL in spinal deformity patients with nephrolithiasis. Limitations of our study is that there is low sample size, no randomization was done, use short time to follow up, and lack of stone analysis and metabolic work up to prevent stone recurrence.
Conclusions
In spinal deformities patients having renal stones PCNL can be perform safely and effectively. Supine position is a better option to perform PCNL in spinal deformity patients with nephrolithiasis as compared to the prone position. PCNL in modified supine position provides benefit of performing the procedure in a more physiological position, which reduces the total operating time, less anesthesia related complications, less neuromusculoskeletal injury. Additional benefits of modified supine position is reducing physical strain on operating surgeon by increasing the working space of operative field which generally hampered in case of spinal deformity patients.
Footnotes
Author contributions
Concept—Sunirmal Choudhury, D. K. Pal; Design—Sunirmal Choudhury, Atar Kasim, D. K. Pal; Supervision—Sunirmal Choudhury, D. K. Pal; Materials—Sunirmal Choudhury, Atar Kasim; Data Collection and/or Processing—Atar Kasim; Analysis and/or Interpretation—Sunirmal Choudhury, Atar Kasim; Literature Search—Atar Kasim; Writing Manuscript—Atar Kasim; Critical Review—D. K. Pal.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Yes, approved.
Informed consent
All subjects provided written informed consent for inclusion in the study/for undergoing the procedures described.