
Abstract
Objective:
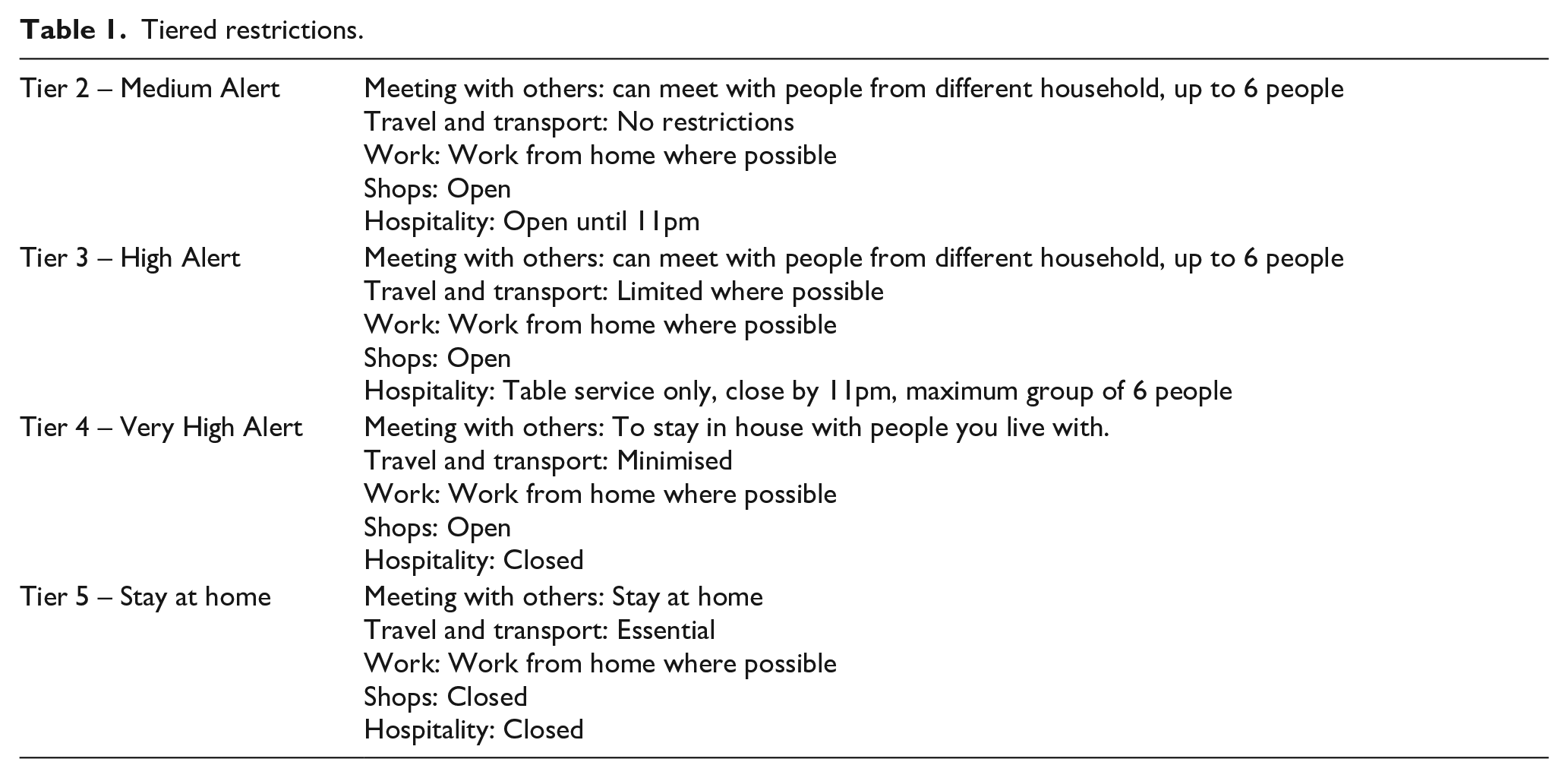
COVID-19 resulted in Regional tiered restrictions being introduced across the UK with subsequent implications for planned and emergency surgical care. Specific to Merseyside, Tier 4, Tier 2 and Tier 5 restrictions were introduced in late 2020 and early 2021. The purpose of this study was to examine the nature and workload of emergency urological procedures during three different national lockdown Tiers in the North West of England.
Method:
A 3-month prospective study examining all emergency urological activity was conducted from November 2020 when Tier 4 restrictions were introduced and included Tier 2 restrictions in December and then concluded at the end of January 2021 when Tier 5 restrictions were in place. Data was obtained by identifying patients using the electronic theatre listing system.
Results:
A total of 71 emergency cases were performed (24 in November (Tier 4), 28 in December (Tier 2), 19 in January 2021 (Tier 5)) with 15 different types of procedures performed. The most frequently performed procedure was stent insertion (36), followed by scrotal exploration (10). The least commonly performed procedure was suprapubic catheter insertion under general anaesthesia (1). One patient required transfer to a different hospital. In total 6 calls were made by general surgery and 3 by gynaecology for urgent urological assistance in theatre. Three urology patients returned to the theatre as emergencies following elective procedures.
Conclusion:
Unlike the Spring lockdown, acute urological presentations requiring operative intervention still presented daily. Of the 71 cases performed, most occurred in Tier 2. Stent insertion was the most commonly performed procedure, with the majority of the cases performed by registrars.
Introduction
The World Health Organization (WHO) formally announced in early 2020 an outbreak of a respiratory virus in Wuhan, China, was caused by named COVID-19. 1 In March 2020, a pandemic was declared by the WHO due to the spread of the Coronavirus involving more than 118,000 cases and 4000 deaths in 114 countries. 2
In the UK, a national lockdown was announced in March 2020. 3 The Government ordered citizens to work from home and placed limitations on social contacts to prevent the National Health Service from becoming overwhelmed. 3 During the first wave of the COVID-19 pandemic in the North West of England, the exponential rise of cases placed the region at the top of the leader board, following London. 4
A significant decrease in elective and emergency surgical cases was registered in different countries.2,5,6 As a result, duties were distributed to all hospital specialities to cope with the growing demand for patients with COVID-19.6,7 The resultant demands placed on Intensive care, nursing and Anaesthetic capacity led to a lack of availability of staff for elective surgical work.
COVID-19 affected all aspects of surgical care, from outpatient consultation to non-emergency surgery and diagnostics.7 –9 The pandemic affected urological practice, ranging from treatments provided to patients to the teaching opportunities available to trainees.7 –10
For acutely hospitalised non-COVID-19 patients, the aim was prompt, safe discharge as per British Association of Urological Surgeons (BAUS) recommendations. 9 Alterations included the earlier discharge of patients with urosepsis once parameters improved rather than proceeding with observation for 24 h. 9
During the initial lockdown, all routine appointments and diagnostic procedures were postponed and new methods of consultation were applied, that is, telephone or virtual consultations.7,9 –11 BAUS published alternative approaches for managing cancer.9,12 For major uro-oncological procedures, new modifications were applied in order to maintain the continuous provision of surgical services.4,13
Procedures such as cystoscopy, prostatic biopsies, and intravesical therapy for low or intermediate tumours were postponed.7,14
Uro-oncology services adapted quickly. Cognisant of the medico-legal implications of late diagnoses, specifically for malignancies like bladder cancer, units developed an electronic register that proved invaluable in detecting surveillance delays. 15
Non-urgent stone procedures such as ESWL were deferred.11,16 Emergency surgical cases were permitted with guidelines issued to avoid laparoscopic procedures.4,7 –9,17
The decision of which operative intervention to perform remained the responsibility of the Consultant Urologist. During the First wave, the decision was made by the department chair or committee of the surgical division. 8 Some hospitals applied specific COVID-19 Urology surgical Triage Algorithms, 5 or priority groups as per NHS England guidance (Level I-IV)4,12 The Cleveland Clinic recommended a 4 Tier classification. 9 Non-invasive procedures such as ESWL for acute stone presentations or nephrostomy insertion for acutely obstructed kidneys were recommended if available.7,18
Although the first wave of the COVID-19 eased, the second surge in the Autumn developed quickly. 19 As the pandemic progressed, regional Tiered restrictions were introduced. 19 Specific to the North West UK, three different Tiers were applied between November 2020 and January 2021 (Table 1). This resulted in varying levels of permissible social mobility with specific implications for the hospitality industry and retail. Specific to our Trust, there was a drive to continue some elective surgical work with all oncological cases remaining a priority. Elective reconstruction and core work were curtailed in January 2021, due to a lack of theatre staff as they had been (a) redeployed or (b) ill with COVID-19. As the study progressed, we noticed that patients continued to regularly present with non-COVID-19 related emergencies.
Tiered restrictions.
Methods
A 3-month prospective study examining all emergency Urology procedures was performed by the Department of Urology in Whiston Hospital, Merseyside. The study’s primary aim was to determine the volume and nature of emergency work performed by the department of Urology during three different tiers of the pandemic between November 2020 and January 2021 (Table 1). A secondary aim was to determine if the national message of ‘Stay at home and protect the NHS’ still resulted in decreased emergency presentations to a large urology unit in North West of England during tiered restrictions as during the initial wave, emergency activity reduced significantly. A third aim was to examine the grade of the practitioner performing the procedure. Training opportunities had been severely affected by the mandatory reductions in elective theatre activity during the first wave and we were eager to record the exposure of trainees to emergency work when tiered restrictions were in place. Data was obtained daily using the electronic theatre listing system with additional input from the urological registrars collected during their on-calls.
All patients requiring emergency urological procedures following an acute admission under urology were included. Additionally, acute presentations that required transfer to other Hospitals for ITU management were included. Referrals made to the urology team for urgent intraoperative assistance from the general surgical, obstetrical or gynaecology teams were recorded. Urgent one-off non-invasive procedures, such as ESWL (Extracorporeal Shock Wave Lithotripsy) were also included and selected catheter-related issues that required General anaesthetic input. Any patient that returned to theatre on an emergency basis following an elective procedure was also included. Grade of operator was also recorded in all cases. A data base was maintained during the 3-month study, which was updated and analysed on a daily basis by the study lead with the above details recorded.
Results
A total of 71 procedures were carried out over three different phases of national restrictions introduced in response to the changing regional levels of COVID-19 between November 2020 and January 2021 (Figure 1). Detailed analysis revealed that 15 different procedures were undertaken during the second wave of the COVID-19 pandemic with the regional Tier system restrictions in place (Figure 2).
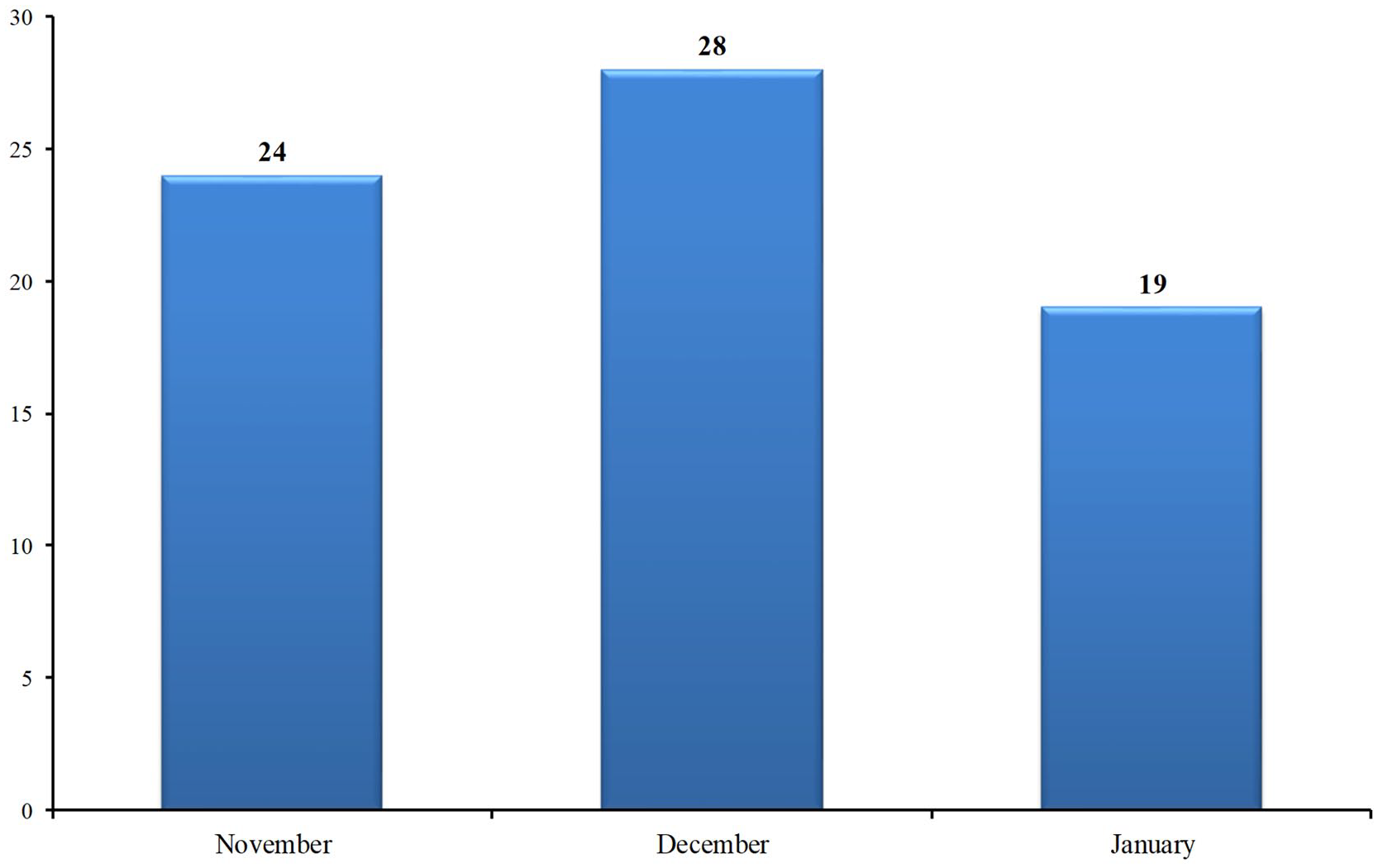
Volume of procedures performed during the three different Tiers (2020–2021).
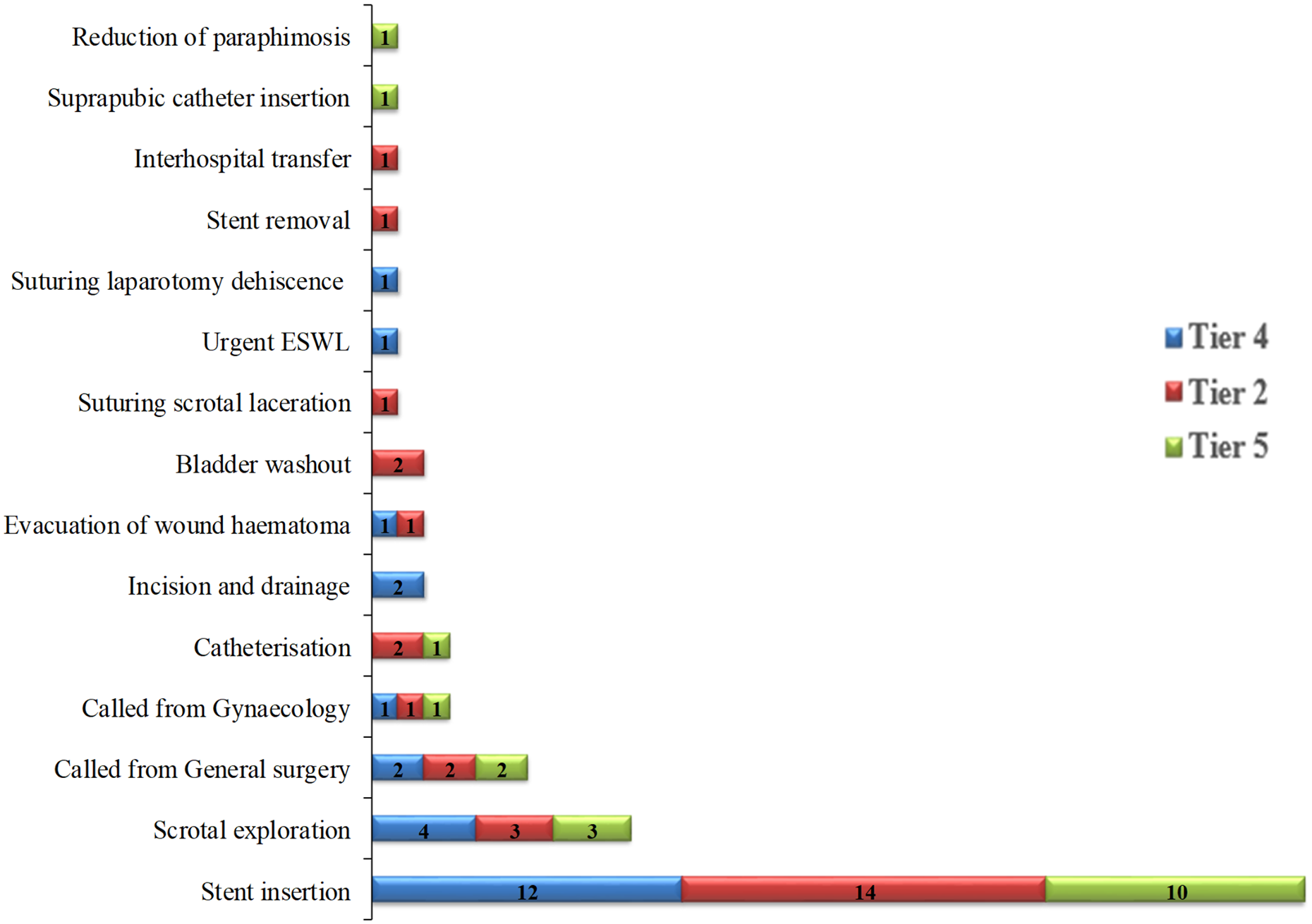
All procedures performed during the three different Tiers (2020–2021).
During the first month of the study (November 2020) 24 cases were performed during level 4 restrictions. An increase in procedures performed was noticed when the Tier 4 restrictions eased in December 2020 to Tier 2 with 28 cases performed and a significant drop in cases was observed when national lockdown was introduced in January 2021 (Tier 5) with only 19 cases performed (Figures 1 and 2).
The commonest procedure performed was stent insertion (36, 51%), followed by scrotal exploration (10, 14%) across all three tiers. The general surgical team required urological input on six occasions (9%) and the gynaecology team on three occasions (4%). Over half of the procedures were performed by the specialist registrars unsupervised (44, 62%), while 10 procedures were performed by Consultants (Figure 3).
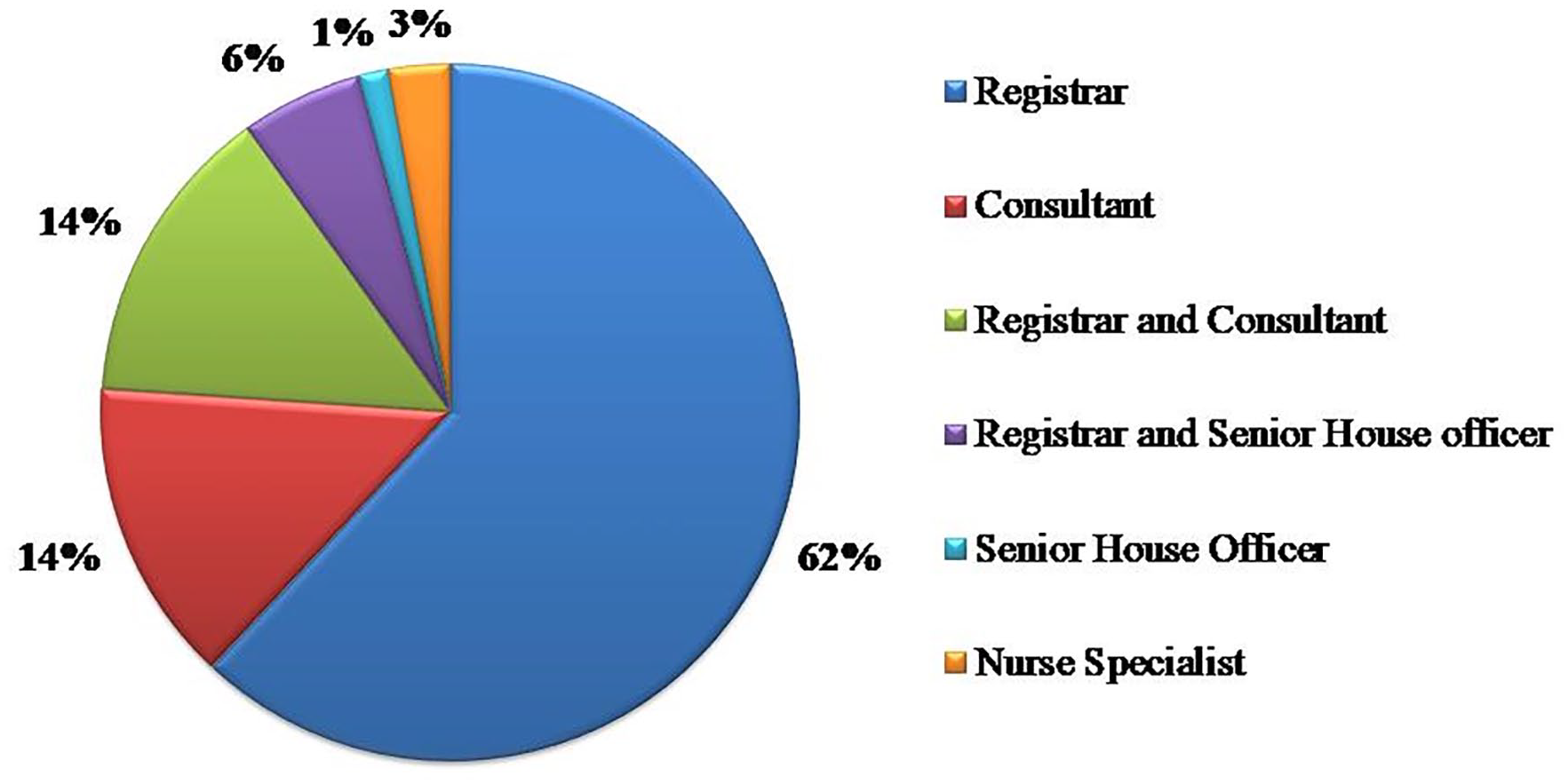
Grade of operator.
The monthly breakdown revealed that in November 2020 when Tier 4 restrictions were in place a total of 24 procedures were undertaken (Figures 1 and 2). In November, eight different procedures were performed, with stent insertion being the commonest (12, 50%), followed by scrotal exploration (4, 17%). The urology team was called for assistance from the general surgical team twice and once from the gynaecology team. One patient returned to theatre following an elective Burch Colposuspension. A single patient required inpatient Extracorporeal Shock Wave Lithotripsy (ESWL), which was in operation in the Trust during Tier 4 restrictions in a very limited capacity, led by urology nurse specialists. Half of the procedures were performed by specialist registrars independently, while Consultants supervised five of the specialist registrars’ procedures. In only four cases, the Consultant performed the emergency procedure.
Detailed analysis of December 2020 when Tier 2 restrictions were introduced in Merseyside, 20 revealed that 28 emergency procedures were performed that month. Ten different procedures took place, of which stent insertion was again the most frequently performed procedure (14, 50%), followed by scrotal exploration (3, 11%). Urological input was required twice from the general surgical team and once from the gynaecology team. One patient required an immediate return to theatre for suspected post-operative bleeding following an elective Burch Colposuspension. One patient required urgent transfer to a different hospital for ITU and dialysis management. Half of the procedures (14, 50%) were performed by specialist registrars without supervision, and in four cases, there was a supervising Consultant present. On six occasions, direct involvement of the Consultant Urologist was required.
A national lockdown was introduced in January 2021 as ‘alert level 5’ in response to a significant increase in COVID-19 cases following the Christmas Holiday period. 21 It was advised that citizens stay and work from home if possible, schools were closed, and people were only allowed to leave the house for basic necessities or medical assistance. 21
In total, 19 emergency urological procedures were performed during January 2021 during the imposed national lockdown (Tier 5). Detailed analysis demonstrated that only seven different procedures were performed. Stent insertion was again the procedure most frequently performed (10, 53%), followed by scrotal exploration (3, 16%). Three calls were made to the urology team for assistance: two from the general surgical team and one from the gynaecology team. Two bladder washouts under general anaesthesia occurred. One patient required urgent suprapubic catheter insertion under general anaesthesia due to a dislodged catheter and pain concerns with previous catheter placement under local anaesthesia. Three urgent catheter placements performed by the urology team for different medical teams were recorded during the study.
Although lockdown prevented face-to-face consultations in primary care20,21 and limited social interactions outside permitted family bubbles, during the 3-month study there were no Fournier’s gangrene or penile fracture cases. Additionally, due to the national restrictions on team sport no sport related Urogenital injuries presented. One trauma case did present during the 3 months: a scrotal laceration which required suturing.
Overall, out of 71 procedures performed stent insertion and emergency scrotal exploration remained the two most frequently performed procedures during the three different Tiers of lock down with 36 stents inserted and 10 scrotal explorations recorded. The four least commonly performed procedures were suprapubic catheter insertion under general anaesthesia (1), urgent ESWL (1), stent removal (1) and reduction of paraphimosis (1). Specialist registrars performed a total of 62% of cases without supervision and 14% of cases were performed by Consultants in a supervisory or training capacity with a registrar. Therefore, trainees were involved in 76% of all emergency cases. Only 14% of call cases were performed by Consultants with no trainees.
Discussion
The emergence of the COVID-19 pandemic in the Spring of 2020 brought unprecedented changes to all facets of healthcare delivery across the globe. Specific to the UK, the initial lockdown led to a cessation of elective surgical work as citizens adopted the mantra of ‘Stay at Home and Protect the NHS’. In Tandem, outpatient services and diagnostics ceased, emergency procedures and presentations diminished and new modifications and realignment of the services were applied as per the new COVID-19 restrictions and guidelines.7,9,11,22 Diagnostic measures such as cystoscopy were postponed.14,23,24 Application of safety measures were applied to avoid the spread of COVID-19 cases. 25 Consequently, new cancer diagnoses and other pathologies requiring surgical intervention were limited.
As COVID-19 developed, the associated effects of delayed services were apparent and new guidelines were introduced as Government directions changed and encouraged citizens to use the NHS if unwell for all conditions. Additionally, BAUS published new recommendations for the re-introduction of procedures, especially in the more vulnerable patient groups emphasising the need for continuous risk assessment. 24 Moreover, new efforts were put in place for the reinstatement of elective services. 9
Separately the pandemic led to a rapid increase in the published literature devoted to the effects of COVID-19 on many aspects of urological practice, including service delivery, recommendations for ongoing uro-oncological care provision and innovative ideas for patient care that emerged during the crisis .2,4 –8,13,15,16,26
As elective surgical activity reduced, this had major implications for ongoing surgical training. Several papers have commented on the impact of the COVID-19 pandemic on trainees and indicative training numbers.10,27
Nevertheless, new approaches were developed to maximise teaching opportunities through webinars,10,13,27 virtual journal clubs and on-line lectures. 27 Some face-to-face meetings were replaced with videoconferences.10,27 Additionally, all professional examinations and courses were postponed. 10
In our Trust stringent efforts were made to continue all uro-oncological and semi elective benign work. In Tandem, emergencies continued to present that require urgent operative management. One of the innovative ideas developed in our trust was a risk stratification system for procedures. A Prioritisation system (P1–P5) was devised and utilised at time of listing a patient for a Urological procedure. New listing sheets were printed to reflect this new classification. Urgent time sensitive procedures such as radical orchidectomy were stratified as P1 implying surgery required within 2–3 weeks. Procedures such as vasectomy or excision of scrotal skin lesions were classified as P5 resulting in surgery within 3–4 months.
Specific to this study we aimed to examine the volume of emergency urological procedures performed over 3 months and to examine in detail who performed them. This study has shown that despite Tiered restrictions introduced during the second wave of the COVID-19 pandemic, emergency urological procedures continued as required for acutely admitted cases.
During Tier 4 and Tier 5 restrictions, there was a noticeable decrease in emergency urological cases, especially during the national lockdown in January 2021. In December 2020, when restrictions eased to a Tier 2 restriction the volume and the nature of procedures increased with nine additional procedures performed in Tier 2 compared to Tier 5. However, acute urological presentations requiring surgical intervention still occurred despite local and national restrictions, unlike the first lockdown in March 2020.
Gallioli et al. during the first lockdown in Italy, reported that emergency urological admissions were remarkably reduced in comparison with the admissions the year before the COVID-19 pandemic. 28
Regarding non-surgical specialities: although there was a significant increase in patients admitted with a ‘Respiratory diagnosis’, 28 specific medical conditions such as Acute Exacerbation of COPD (AECOPD) were reduced in both periods of lockdown during the COVID-19 pandemic. 29 Unsurprisingly, during the second wave, there was an increase in admissions in comparison with the first wave but not as pronounced as the pre-COVID data. 29
Italy was markedly affected during the COVID-19 pandemic and was the first European Country to implement measures to avoid a further increase in cases. 30 The same considerations applied to Urology as a speciality regarding the treatment of uro-oncology patients.28,31 Systems and guidelines were installed for patients with Non-Muscle Invasive Bladder Cancer (NMIBC).28,31,32 Cancer-risk assessment and factors for perioperative complications associated with the ‘immunocompromised cancer-related state’ were considered with COVID-19. 33 However, a delay in delivery of cancer care was noted, by means of reduced numbers of transurethral resections (TURBT) performed.28,31,32
ESWL is recommended by both the American Urological Association/Endourological Association and European Association of Urology as an effective alternative method for ureteral stones as it avoids general anaesthesia7,16 During this study, it was utilised only once. This was a reflection of the fact that during the pandemic, many nurse specialists (performing ESWL) were redeployed to COVID-19 wards or ITU in our Trust.
From a training perspective, most of the procedures were performed by specialist registrars with 76% of all emergency cases recorded as having registrar involvement. Procedures performed by senior house officers under supervision were minimal; 4 (6%) under the supervision of a specialist registrar and 1 (1%) unsupervised. The COVID-19 pandemic had a negative effect on training for core surgical trainees in urology.10,27 Moreover, in a separate survey assessing the effects of the first wave of COVID-19 on specialist urological training, results showed decreased surgical exposure and that ‘Consultant only’ was preferred in the operating theatre, especially over the peak of COVID-19 cases during the first lockdown.10,13 In a different study conducted during the first wave of the COVID-19 pandemic similar findings were reported; core trainees were predominantly negatively affected by decreased theatre exposure and reduced experience in outpatient settings. 10 The senior trainees were more likely to be allocated theatre time due to experience in order to reduce operating time.9,10,16 Specific to this study, we have shown that specialist registrars carried out most emergency procedures and this is an important finding from this study.
This study has some limitations. Firstly, only patients requiring emergency urological procedures were included and there was no record of all the urological patients needing admission during this period, such as those presenting with orchitis, pyelonephritis or retention. Another limitation is that an accurate comparison of the rate of emergency procedures during the second period of regional lockdown restrictions to that experienced in the first wave in Spring 2020 was not performed as this study aimed to deal with the emergency procedures performed during the second wave only. Regrettably, we did not record ‘wait times’ for urology emergencies in accessing the emergency department of our hospital compared to the first wave or in the non-pandemic era, which is another limitation of this study. Admittedly, the complexity of the urgent procedures performed is also minimal as stent insertion and scrotal exploration remained the two most commonly performed procedures during the 3-month study. This study was conducted over a short period of time when the Tiered restrictions were implemented and as a result a small cohort of patients were included and this is a major limitation of this study. The reduction of social interaction and cessation of team sports as alluded to earlier meant that less frequent emergency cases such as Fournier’s gangrene and penile fracture did not feature during the period studied. A separate study is planned to looked at post pandemic recovery in urology.
Conclusion
This 3-month study has demonstrated the impact of the Tiered restriction system on the emergency urological procedures performed in a large UK Hospital. A total of 71 cases were performed, with more occurring in Tier 2. Increased restrictions had a definite impact on emergency case presentations. We have further demonstrated as a result of this work that (a) unlike the Spring lockdown emergency cases requiring surgery still presented and (b) trainees continued to have exposure to emergency operations during the pandemic with Consultant supervision.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.