
Abstract
Aim:
To evaluate the value of transrectal shear-wave-elastography(SWE) to differentiate benign and malignant tissues in patients with suspected prostate cancer.
Materials and methods:
Between January and May 2019, the study was designed as a prospective clinical study. The SWE value of 504 cores measured before biopsy and the pathology result of each core were used in the statistical analysis. The SWE values of benign and malignant cores were compared according to pathology results. ROC analysis was used to calculate the best cut-off SWE value for differentiating malignancy from benign tissues. Specificity, sensitivity, negative, and positive predictive values (NPV, PPV) were also calculated for cut-off value.
Results:
Prostate cancer was detected in 74 (14.7%) of 504 core biopsies. The mean SWE values were found significantly higher in malignant cores (71.1 kPa) than benign cores (42.3 kPa) (p < 0.001). Cores with gleason score 7 had a significantly higher SWE value than Gleason score 6 (p = 0.009). The cut-off value to differentiate malignancy and area-under-curve were calculated 35.85 kPa, 0.733, respectively. The sensitivity, specificity, NPV, and PPV were 83%, 49%, 78%, and 95%, respectively for 35.85 kPa value.
Conclusions:
The malignant tissues have significantly higher SWE values. Also high gleason score was shown to be associated with high SWE values. To predict the prostate cancer, the difference of SWE values of between benign and malignant tissues has high sensitivity. In the near future, to prevent unnecessary prostate biopsies, SWE will be part of the standard protocol for prostate imaging.
Introduction
Traditionally, ultrasound-guided systematic biopsies have been used to diagnose prostate cancer. The number of prostate biopsies dramatically increased by 70% after using the total PSA value as a screening test to detect prostate cancer. This significant increase in biopsy numbers causes more unnecessary biopsies, more complications (such as bleeding, infection, and pain), and so more cost to the health care system.1,2
New radiological techniques such as multiparametric magnetic resonance imaging (mp-MRI) and various ultrasonographic methods (such as sonoelastography) have been researched to reduce the number of unnecessary biopsies. 3
Mp-MRI has especially good sensitivity for the detection and localization of Gleason score ⩾7 cancers, when the diameter of the tumor is larger than 10 mm, although mp-MRI is identifies only less than 30% of Gleason score 6 when the tumor is smaller than 0.5 cc. Mp-MRI can be insufficient to identify especially low-grade prostate cancer.4,5
Shear-wave-elastography (SWE) is a relatively new ultrasonographic method. SWE is a non-invasive way to measure tissue elasticity (degree of stiffness) according to the response of the tissue to an applied acoustic force.6,7 Based on the principle that malignant and fibrotic tissues become stiffer, SWE is widely used to evaluate parenchymal tissue’s elasticity changes in solid organs such as the liver, breast cancer, or thyroid nodules. 8
With this study, we aimed to assess the effectiveness of transrectal SWE, which is a non-invasive way to differentiate benign and malignant tissues in the prostate, with negative mp-MRI findings, to prevent unnecessary biopsies, biopsy-related complications, and excessive cost burden on the health system.
Materials and methods
Study population
Ethical and institutional approvals (Research Ethical Committee number: 2018-12/149) were demonstrated, and an informed consent form was received from all patients after a detailed explanation of the procedures. Between January 2019 and May 2019, 54 patients who had elevated PSA (up to 4 ng/dl) and/or a suspicious digital rectal examination and Mp-MRI negative(PIRADS 1-2) were included in the study. Twelve of the patients with a history of dutasteride use or any surgical procedure for the prostate that might have affected the stiffness of the prostate tissue and PSA level and patients whose SWE parameters could not be measured according to the ideal study protocol were excluded from the study. After the exclusion, transrectal SWE measurement and the 12-core standard systematic prostate biopsy procedure were applied to all patients, respectively. All 42 patients’ data were used to statistical analysis.
Transrectal ultrasound, shear-wave-elastographic imaging
Transrectal SWE value of the prostate were measured with real-time SWE imaging using an ultrasound machine (Toshiba Aplio, TUS-A500, Toshiba Medical Systems Corporation, Otawara, Japan) and an endocavity transrectal (6 MHz) probe by an experienced urologist and a radiologist with 3 years of elastography experience.
The patient was immobilized, and volunteer pressure was not applied to the prostate with the probe at lateral decubitus position. Using the endocavitary transrectal probe, the prostate was imaged, and SWE values were measured in the transverse plane at the base, middle, and apex levels for the right and left lobes of the prostate separately. SWE values were measured using 3–5 mm diameter circular ROIs (regions of interest) in each area where the standard 12-core biopsy was sampled in the peripheral zone (PZ). The SWE values of PZ (kilopascal, kPa) were recorded as yPZ (Figures 1 and 2).
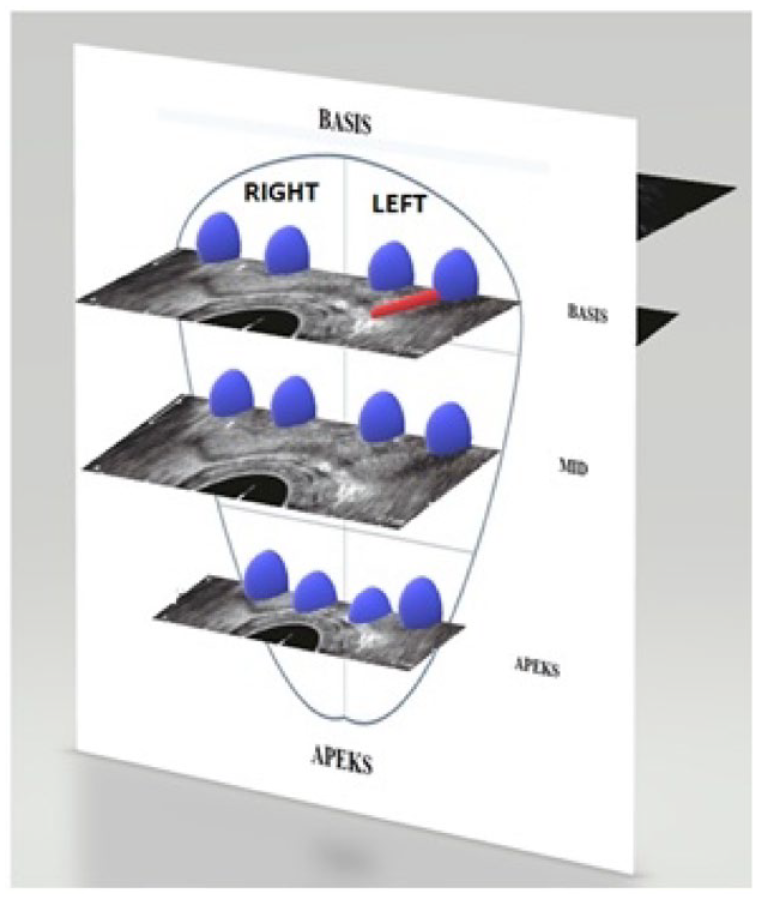
Locations of SWE measurement and biopsy cores: Measurement of SWE and location of the areas of standard 12-core biopsy on the prostate gland. Blue spheres where the SWE measurement will be made in the transverse plane with USG and the biopsy sample will be taken in peripheral zone and the path of the biopsy needle (red line).
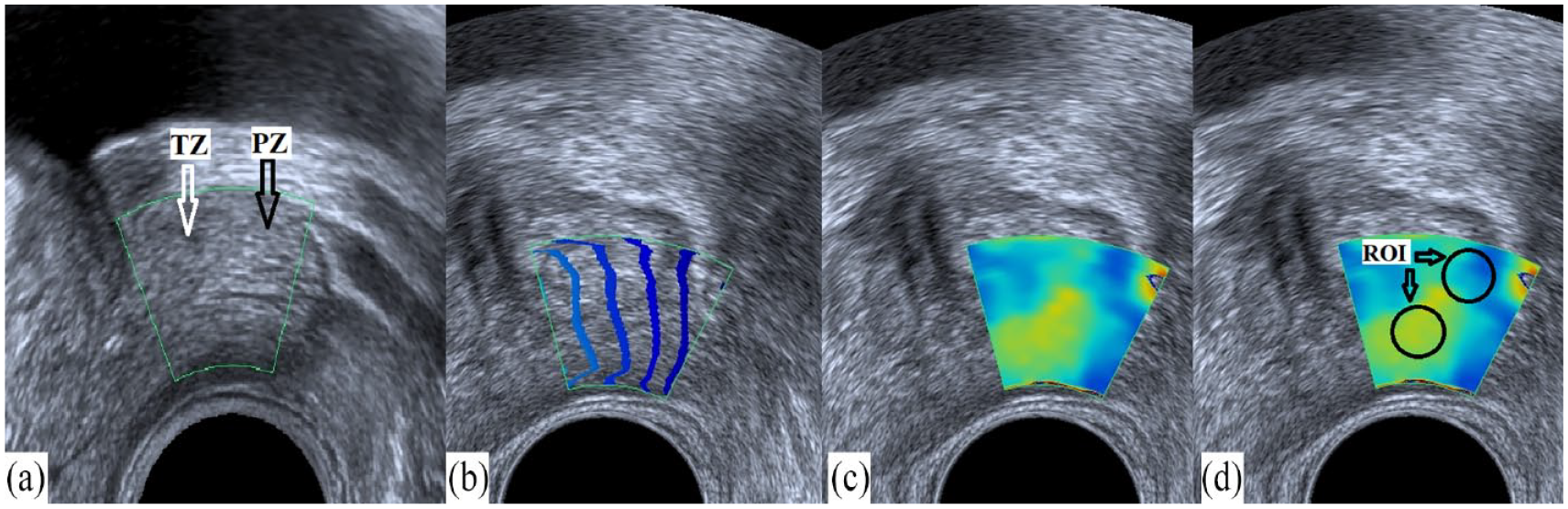
SWE measuring: A 67-year-old patient, 69 cc prostate gland, normal image of the left prostatic lobe at midline; USG examination (B mode, SWE). (a) B mode view, peripheral zone (PZ) (black arrow), transitional zone (TZ) (white arrow); (b) propagation window, waves must be parallel to each other for artifact reduction; (c) SWE mode view, elastography window (yellow and red colors indicate stiffer tissue, blue color softer tissue); (d) Elastographic calculation of stiffness with a 3 mm circular ROI (recorded as yPZ, kPa) at the biopsy point at the PZ.
Prostate biopsies
The standard 12-core prostate biopsy procedure was performed after SWE imaging. Cores with a total Gleason score of six and above were considered malignant, and the other pathological types were recorded as benign.
Data analysis
SPSS 22.0 software package program was used to analyze. The primary results were the reliability of SWE in differentiating benign and malignant prostate tissues. The SWE values of PZ were compared between the benign and malignant tissues.
The T-test and Mann–Whitney-U test were used to analyze the numerical measurements between patient groups. Using SWE values, the cut-off value and area under curve (AUC) were calculated with receiver operating characteristic (ROC) analysis.
To calculate the ideal cut-off value, the Youden index (sensitivity – (specificity − 1)) was calculated using the specificity and sensitivity values of each value obtained from the ROC analysis. The Young’s modulus value, which provides the highest Youden index value, was accepted as the ideal cut-off value in our study. The specificity, sensitivity, negative and positive predictive values were calculated for this ideal cut-off value. The p-value was accepted as <0.05 at a 95% confidence interval.
Results
The mean age of the patients was 63. The mean total PSA value was 11.8 ng/dl, and the prostate volume was 56.7 cc. According to the biopsy results, 13 (31%) of 42 patients were diagnosed with prostate cancer. There was no significant difference in the age, total PSA, and prostate volume of the benign and malignant patients (p = 0.34).
Due to artifacts in SWE imaging, a reliable measurement could not be performed in eight cores. Data obtained from the only 496 artifact-free SWE images of the cores were used in all statistical analyses.
The mean yPZ value of all cores (n: 496) was 46.2 kPa. The mean yPZ values of benign (n: 428) and malignant (n: 68) cores were 42.3 kPa and 71.1 kPa, respectively. The mean yPZ value of malignant cores was higher than benign cores(p < 0.001) (Table 1) (Figure 3).
yPZ values of ROIs measured with SWE at the peripheral zone.
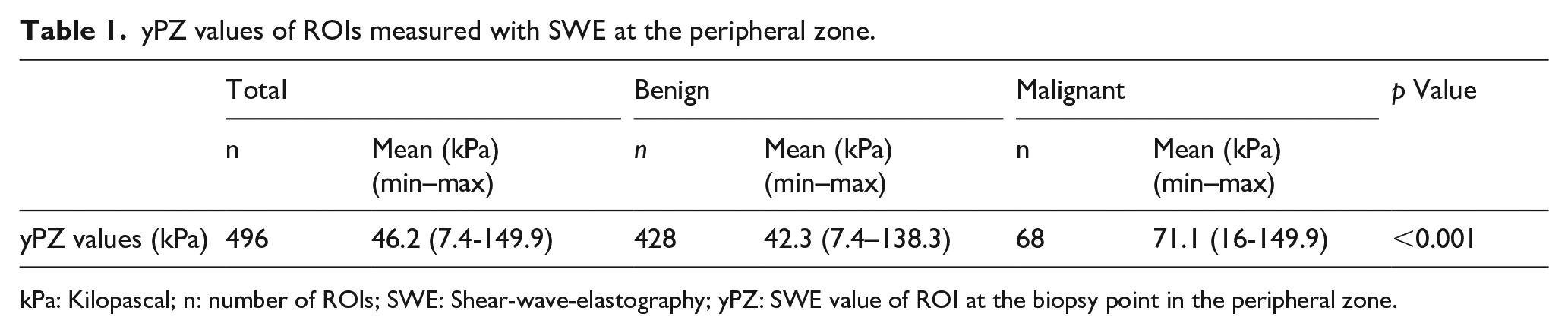
kPa: Kilopascal; n: number of ROIs; SWE: Shear-wave-elastography; yPZ: SWE value of ROI at the biopsy point in the peripheral zone.
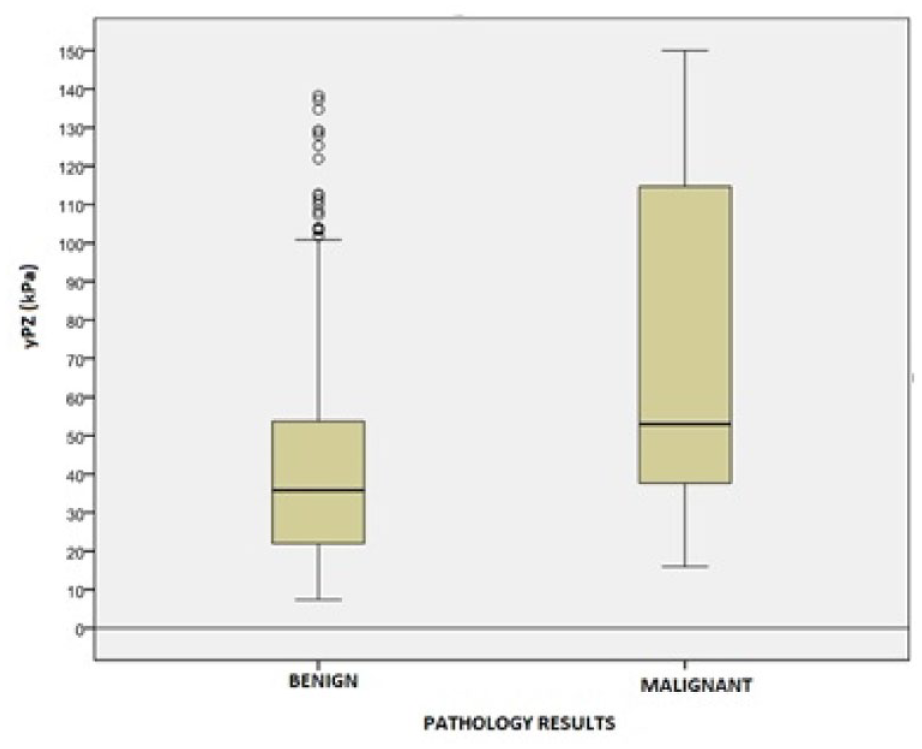
yPZ values (kPa) of benign and malignant cores in the elastographic evaluation of the peripheral zone.
The mean yPZ value of cores with a Gleason score of 6 (n:34) was 54.2 kPa and Gleason score ⩾7 (n:34) was 79.7 kPa, respectively. Cores with a Gleason score ⩾7 had a significantly higher SWE value than those with a Gleason score 6 (p = 0.009).
It was determined that 75% of the cores (n = 6), whose anatomical borders of the prostate gland could not be clearly evaluated by gray scale ultrasonography and dense artifact was observed in the SWE measurement, were malignant.
The ideal cut-off yPZ value between benign and malignant tissues at the peripheral zone was calculated as 35.85 kPa using the ROC analysis (AUC:0.733). For this 35.85 kPa value, the sensitivity, specificity, negative, and positive predictive values were 83%, 49%, 78%, and 95%; respectively (Figure 4).
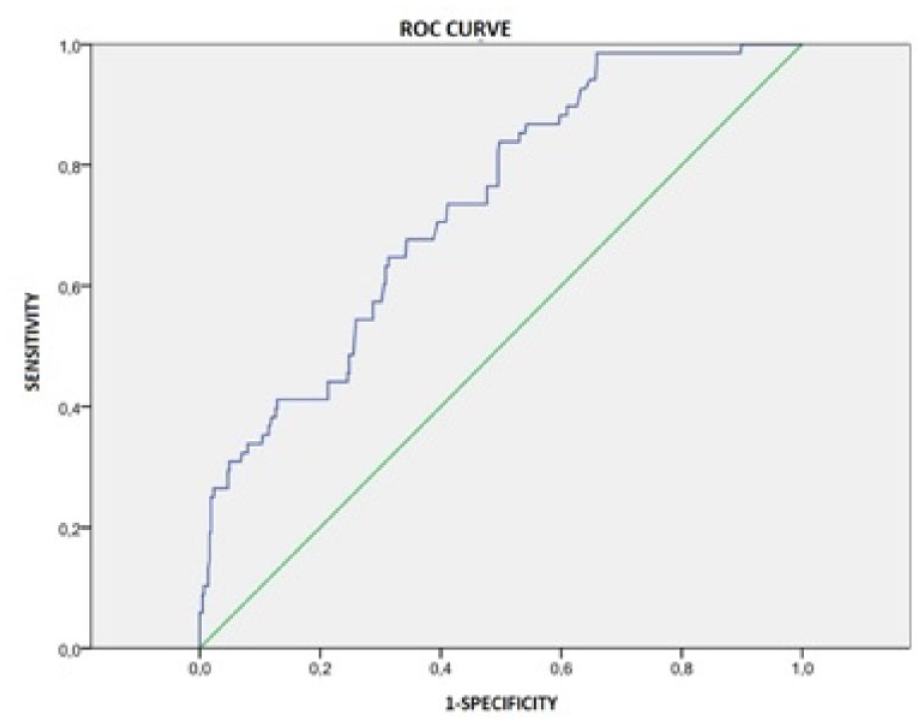
ROC curve of yPZ values; area under the curve (AUC): 0.733. (ROC: receiver operating characteristic).
Discussion
Shear wave elastography, a recent technique compared to conventional ultrasound examination, was found more successful at detecting prostate cancer in various studies. With this study, we also assessed the effectiveness of the transrectal SWE value to identify the benign and malignant tissues in the prostate gland.
According to a recently published a review, the sensitivities and specificities of studies ranged from 0.43 (95% CI = 0.32–0.55) to 0.96 (95% = CI 0.80–1.00) and 0.43 (95% CI = 0.31–0.56) to 0.96 (95% CI = 0.93–0.98), respectively. Among the studies, the cut-off values for distinguishing malignant from benign prostatic lesions ranged from 28.5 to 82.6 kPa. These wide ranges were caused by the variation in the methodological quality of the studies. Hence the standardization of using elastography in detecting prostate cancer is still unclear. The cut-off SWE value to predict malignancy of the prostate has a very wide range between 35 and 82.6 kPa.9 –16 In our study, the cut-off SWE value was found as 35.85 kPa (AUC: 0.733) and for this value; the sensitivity, specificity, negative and positive predictive values were calculated as 83%, 49%, 78%, and 95%; respectively.
The gleason score of malignant tissues can affect the SWE values. Patients with clinically-significant PCa (Gleason score ⩾7) have a higher SWE value than the low-risk group in the current literature. In our study, the yPZ values of tissues with a Gleason score ⩾ of 7 had a higher value than gleason score of 6 (p < 0.05).9,11
Prostate cancer was diagnosed in approximately 20% of the other prostatic zones than PZ. The mean Young’s modulus values of prostatic zones were found to be different between PZ and TZ. It was shown that average SWE value of TZ was higher than PZ in both malignant and benign patients in current literature. The difference between the PZ and TZ’s values was thought to occur from having higher glandular content in the PZ than TZ. Similarly, SWE values of ventral prostatic tissues had higher values than dorsal tissues and medial tissues had higher values than the lateral tissues of the prostate gland. According to current literature, due to insufficient penetration depth, SWE values of TZ cannot be considered sufficient and there is not enough data about the performance of SWE in the diagnosis of PCa in the other prostatic zones than PZ.17,18
There is heterogeneity at the location, number and size of ROIs used in SWE measurements. Contrary to expectation, sensitivity was found to be significantly lower when more than one ROI was used (43% vs 86%, p = 0.04). In our study, only one 3–5 mm diameter-circular ROI was used per biopsy core to measure the yPZ value. 19
Transrectal SWE value measuring is superior to other techniques by providing quantitative data, although it has some limitations. Elastographic measurement is based on the response of compression of tissues. Compression types are different between elastographic techniques. Unlike strain elastography, SWE, is independent of the user, provides objective data resulting from the type of compression technique. Although manual compression of the transducer is not used in the SWE technique, involuntary compression to the prostate may occur especially in large-volume prostates.
Because there is a significant difference between the sagittal and axial imaging planes, the ideal measuring plane is not known yet. This difference is thought to be due to tissue anisotropism and involuntary compression force intensity.
The acoustic wave forces, which are used in SWE, give successful technical results at approximately 3–4 cm depth in the tissue. Therefore, the peripheral zone and the transducer are adjacent during SWE measuring, and acoustic forces can reach all parts of the peripheral zone. Measurement of SWE is not effective enough to evaluate anterior prostatic tissues, especially in large-volume prostates due to the insufficient acoustic forces at tissues that are distant from the transducer. 20
Artifactual image formation is frequently observed during elastographic measurement. In our study, 75% of the cores that could not be measured due to dense artifact, were found to be malignant. The stiffness of malignant tissues above the measurable limits or the high heterogeneity of malignant tissue might have caused this artifact formation, however, there is no data to prove it yet.
Our study had some limitations. The zonal anatomy of the prostate, selection of patients, size of ROIs, and locations were different in the literature. Similarly, there was no clear data on the ideal imaging plane of the prostate (such as a sagittal or axial plane). SWE was not a standard method used in the current literature to detect prostate cancer. In some cases, only the areas inside the measurement window could be measured due to the narrow area of the measurement window in especially transitional zones of large-volume prostates. Additionally, the depth of the tissues increased when the measurement quality decreased in the transitional zone. As a result, we planned our study similarly to previous studies to assess only the peripheral zone.
SWE will be used in determining the biopsy target if new prospective studies can demonstrate that the transrectal SWE value of the prostate has good performance in detecting PCa. Measuring the SWE value for each biopsy core will be a simple way to determine the biopsy target especially in the cognitive targeted biopsy technique. Therefore, SWE may play an important role in targeted biopsy procedures in the near future.
In conclusion, transrectal SWE values were significantly different between benign and malignant tissues in the peripheral zone. Moreover, tissues with high Gleason scores had higher values. The transrectal SWE value had significantly high sensitivity in predicting prostate cancer, therefore, a clear cut-off value could not determined due to the heterogeneity of study protocols in the current literature. We believe that SWE will soon become a standard tool for prostate imaging and biopsy protocols, preventing unnecessary biopsies and differentiating malignant from benign tissues.
Footnotes
Authors’ note
This study was presented orally in 11th Internatioanal Eurasian Urooncology Congress in Turkey at 2021.
Author contributions
![]() .
.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval for research involving human participants
The study was approved by the local ethics committee (protocol number: Research Ethical Committee (REC) number 2018-12/149 at 2018) at University of Health Sciences Dr. Abdurrahman Yurtaslan Oncology Training and Research Hospital. All procedures performed in our study involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
A formal written informed consent was obtained from all individual participants included in the study. The data of patients who did not consent was not used.