
Abstract
Introduction:
Posterior urethral injuries in men commonly occur following pelvic and perineal trauma. Erectile dysfunction (ED), whether brought on by the severity of the initial trauma or the surgery itself, is one of the complications in these patients.
Materials and methods:
In this study, we divided candidates of posterior urethroplasty due to traumatic urethral injury into intervention and placebo groups; the former received continuous treatment with tadalafil (10 mg daily), and the latter received a placebo. Other services were provided equally to both groups. Before and after the intervention, both groups completed the International Index of Erectile Function version 5 (IIEF-5) questionnaire, and the findings were analyzed.
Results:
Forty patients were studied in groups of 20 with a mean age of 43.87 ± 15.70 years. The patient’s most common cause of urethral injury was a pelvic fracture. Before the intervention, the mean scores of IIEF for patients in the intervention group and placebo group were 14.85 ± 7.39 and 14.77 ± 6.48, respectively with no statistical significance (p = 0.962) and patients of the groups were similar in terms of the severity of ED. The mean IIEF score in the intervention group was 20.12 ± 4.94 and in the placebo group, it was 18.05 ± 4.88 at the three-month follow-up, with no statistically significant difference (p = 0.063). In both the intervention and placebo groups, the IIEF score was significantly increased by 5.27 ± 4.04 (p < 0.001) and 3.27 ± 2.97 (p < 0.001), respectively. The rate of IIEF increase in the intervention group was higher than in the placebo group during the follow-up at 3-month follow-up with statistical significance. (p = 0.022).
Conclusion:
The findings of this study suggest that tadalafil, in a 3-month treatment course, may improve erectile function in individuals with mild-to-moderate ED, significantly more than placebo. However, more studies, specifically with longer duration of follow-up and larger populations, are necessary for generalizing the current findings.
Keywords
Introduction
A urethral stricture is a scarring event that affects the surrounding corpus spongiosum and urethral mucosa, and partial loss of urethral mucosa is a sign that the scarring process has started. Posterior urethral stenosis may result from conditions of the bladder and prostate or traumas to the pelvis. 1 Some patients respond well to conservative therapies including dilation and endourologic operations, but treatment failure in severe instances with or without full blockage and complicated situations may necessitate surgical surgery. 2
A recent study on complications of urethral stricture due to pelvic fracture and urethroplasty listed the recurrence of the stricture, urinary incontinence, and erectile dysfunction (ED) as the most common complications. 3 Given that many pelvic injury patients are under 40 and have a long life expectancy and that ED is more common in patients with urethral damage who also have pelvic fractures than in patients who do not, this issue is crucial.4 –10
Additionally, in some studies, there was no discernible difference between ED following pelvic fracture urethral injury before and after posterior urethroplasty,11,12 which indicates that the main cause of this complication is probably not a surgical treatment, but the primary trauma itself.
Hormone-related causes (such as thyroid diseases, diabetes mellitus, or androgen deficiency), and non-hormonal causes (such as neurogenic, vasogenic, and psychogenic) are the two main etiologies for ED. The most probable cause of post-traumatic ED is vasogenic disorder.13,14
Phosphodiesterase type 5 inhibitors (PDE5is), which are sold worldwide and include Sildenafil, Vardenafil, and Tadalafil, are now the first-line therapy for ED.15,16 The effects of Tadalafil, alone and compared with other drugs have been previously studied.17,18
For ED, tadalafil has been used with on-demand and daily regimens, while the latter shows slightly better results, no statistical significance is founded. 19 Also, a study proposed a better outcome with a combination of vacuum devices and Tadalafil after urethroplasty. 20
In this study, we examine the prevalence of ED in individuals who have had open posterior urethroplasty and the effects of long-term tadalafil use in these patients. The primary objective of this research was to evaluate the impact of ongoing tadalafil use on patients with ED. We believe that the results of this study can help the patient and the treating physician in choosing the appropriate treatment and improve the patients, accelerating the treatment and preventing the failure of treatments.
Methods
Study population
In this study, we assigned eligible patients for open posterior urethroplasty into Tadalafil or placebo groups using a random number table. We used a two-part questionnaire in which only the analyst had the access to the group categories. We categorized the patients based on trauma mechanisms into straddle injury (with or without sacroiliac joint diastasis), malgaigne fracture, simple pelvic fracture, and no pelvic fractures as the mechanism of injury. We also categorized them based on age groups and assessed their erectile function. We enrolled patients in the study before surgery and we assessed their erectile function with the Persian version of IIEF5 for the presence, and severity of ED.
Patients with no ED at the time of referral or after treatment or during the follow-up period, physical inability to have sex (severe penile deformity, neurological weakness, etc.), dissatisfaction with study participants, and patients with diabetes, hypotension, nitrate consumption, and chronic liver disease were excluded.
Intervention
The intervention was initiated 2 weeks after urethroplasty, after the removal of catheter(s) and edema. The questionnaires were filled 1 week before urethroplasty, 4 weeks after urethroplasty, and 3 months after urethroplasty; but due to relative contraindication of sexual activity in the first 2–4 weeks after urethroplasty, we used morning erection as an indicator of those who were sexually inactive, that were categorized as no morning erection; erection with minimal rigidity; and normal rigid morning erection.
Patients in the intervention group received tadalafil 10 mg, once daily, and the control group received a placebo pill once daily, which was similar to the tadalafil pill.
The scores of the standard IIEF5 questionnaire are based on five questions each has five points, and based on the sum of the points, we categorize them as Severe ED (5–7); Moderate ED (8–11); Mild-to-moderate ED (12–16); Mild ED (17–21); and Normal (22–25).
Statistical analysis
The analysis was performed using SPSS statistical analysis software, version 21. Using the appropriate tables and graphs, the results were presented as mean ± SD and frequency. In order to compare the intervention and control groups’ quantitative and qualitative data, the Student’s t-test and the Chi-Square test were applied. A p-value of less than 0.05 was considered statistically significant.
Results
In this clinical trial, candidates for posterior urethroplasty in the intervention and placebo groups were evaluated. Treatment with Tadalafil in the intervention group and placebo in the second group started 2 weeks after surgery. Patients were re-assessed at 4 weeks and 3 months after surgery. Forty patients were studied in two groups of 20. Patients’ mean ages ranged from 43.87 to 15.70 years (20–74 years). Patients in the intervention group had a mean age of 44.10 ± 16.33 years, whereas those in the placebo group were 43.65 ± 15.25 years. The groups did not vary statistically significantly (p = 0.899). The most common cause of urethral injury in the patients was trauma leading to pelvic fracture (72.5%).
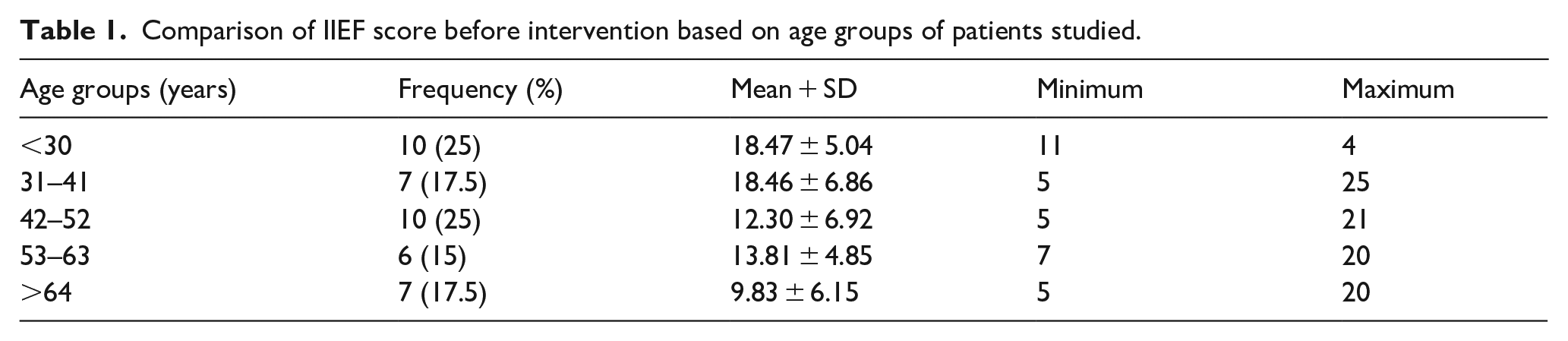
The mean IIEF score of patients before surgery in the intervention group was 14.85 ± 7.39 and in the placebo group was 14.77 ± 6.48. There was no statistically significant difference between the groups (p = 0.962) and the patients of the groups were similar in terms of the severity of ED. The comparison of IIEF scores before the intervention based on the age groups of the patients is shown in Table 1. According to the results, the highest score was related to the fourth decade of patients’ lives, and the lowest was related to the age group over 64 years (p < 0.001).
Comparison of IIEF score before intervention based on age groups of patients studied.
A comparison of IIEF scores before intervention based on the cause of patient trauma for the study is shown in Table 2. According to the results, the IIEF score was significantly lower in patients with pelvic fractures (severe ED) (p < 0.001).
Comparison of IIEF scores before intervention based on the cause of trauma in the patients.

Table 3 displays the patients’ follow-up outcomes in terms of morning spontaneous erections in the fourth week following their intervention. The frequency of no morning erections was shown to be considerably greater in the placebo group, while the intervention group had a higher frequency of normal erections during sleep (p = 0.007).
Comparison of morning spontaneous erection status between two study groups.

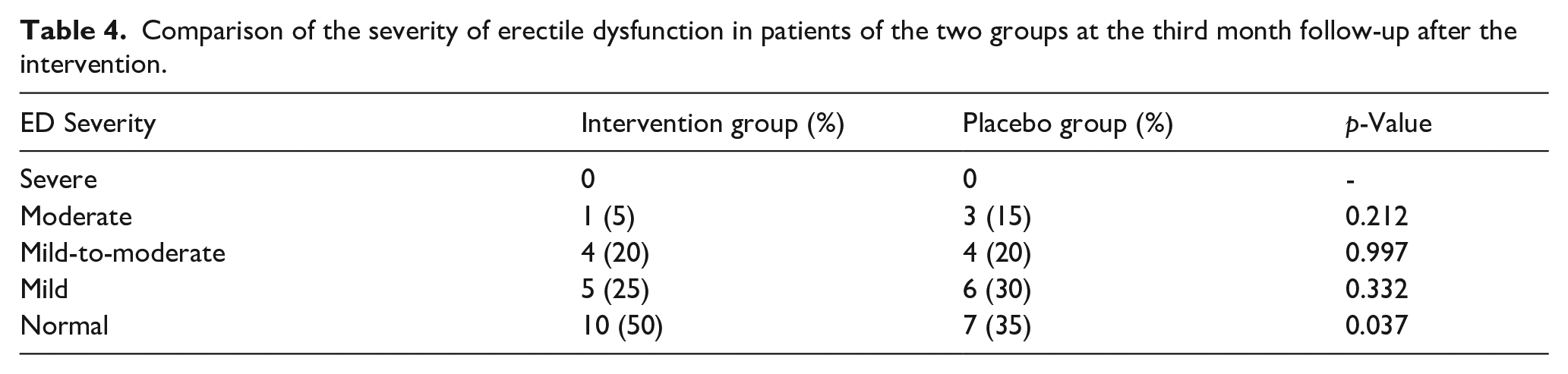
The mean IIEF scores in the intervention and placebo groups were 20.12 ± 4.94 and 18.05 ± 4.88, respectively at the third follow-up month following the intervention. There was no statistically significant difference between the two groups (p = 0.063). In Table 4, the severity of ED in patients is contrasted. Patients in the intervention group experienced normal erections substantially more frequently and the individuals in the intervention group experienced moderate ED less frequently (p = 0.037). IIEF scores were compared to see how they had changed at the follow-up, and it was found that the intervention group’s mean score had considerably increased by 5.27 ± 4.04 points (p < 0.001). In the placebo group, the mean score was also significantly increased by 3.27 ± 2.97 (p < 0.001). Statistically significantly (p = 0.022), throughout the follow-up, the mean IIEF score increased more in the intervention group than in the placebo group (Figure 1). An inverse correlation was observed based on the Pearson test in both groups in comparing the relationship between IIEF score and age in the third month of follow-up. The intervention group had a coefficient of 0.503 (p = 0.001) and the placebo group had a coefficient of 0.375 (p = 0.017). In this study, no serious side effects requiring discontinuation of treatment were observed in the patients studied.
Comparison of the severity of erectile dysfunction in patients of the two groups at the third month follow-up after the intervention.
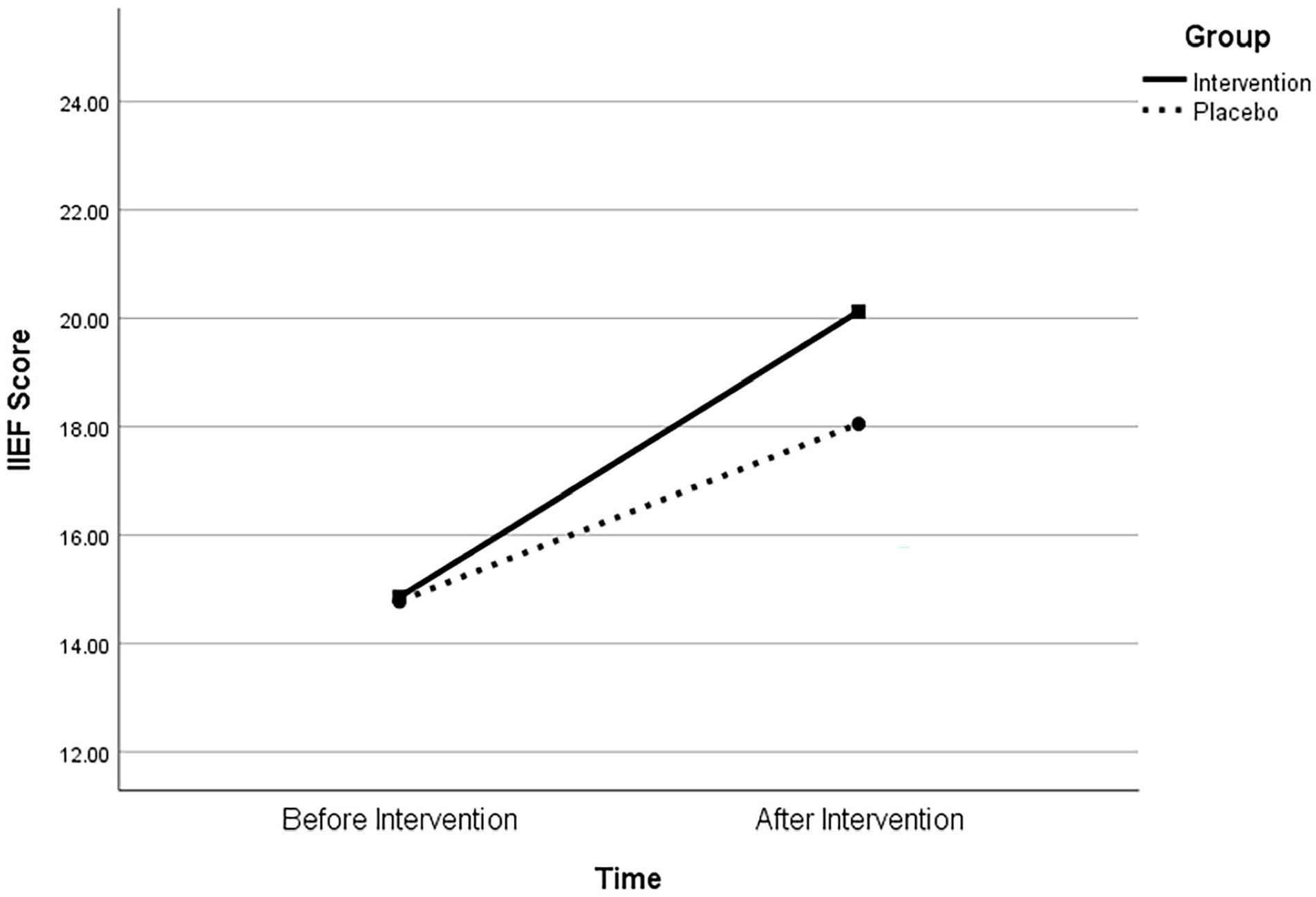
Comparison of changes in IIEF score before and after intervention between the two groups.
Discussion
Due to its deep location in the pelvis, association with the pelvic bone and ligaments, and proximity to complex anatomical structures, including the prostate and the urinary sphincter, surgery of the posterior urethra is one of the most difficult reconstructive scenarios in the lower urinary tract. 2 One of the significant problems identified in research assessing individuals with urethral strictures following reconstructive operations is ED. According to some research, urethroplasty has a negligible impact on erectile function,8,11,21,22 while one meta-analysis suggests that transient ED may occur after posterior urethroplasty, which will be resolved after 6–12 months after the surgery. 23
PDE5i is considered the first-line medical treatment of patients with ED after posterior urethroplasty. 24 In the study by Madeira et al., 25 which examined the efficacy and safety of oral administration of PDE5i for treating ED, 184 studies were reviewed. The results showed that the use of all PDE5i has significantly higher efficacy than that of the placebo. Tadalafil 10 and 20 mg also had an efficiency of 73% and 76%, respectively, in improving the IIEF score. They concluded that sildenafil and tadalafil should be used as the first-line ED treatment. 25
Daily use of PDE5i after posterior urethroplasty has been studied in limited studies, and results were comparable to on-demand use of the same drugs. 26 We chose tadalafil due to better psychosocial outcomes and less necessity for planned sexual intercourse. 18
Bayraktar and Albayrak 27 used tadalafil and aspirin for treating ED. In line with our study. The rates of improvement of the IIEF score in groups 1, aspirin 100 mg/day, 2, tadalafil 5 mg/day, 3, tadalafil 5 mg + aspirin 100 mg, and 4, placebo were 7.2 ± 4.4, 7.3 ± 4.3, 7.5 ± 4.4, and 2.0 ± 4.6, respectively. Possible reasons for the higher improvement in the above study compared to ours can be the longer duration of their treatment and the use of aspirin with tadalafil. 27 Furthermore, because of its anti-inflammatory qualities, aspirin can lessen the adverse effects of tadalafil, such as headache, back pain, myalgia, limb pain, and flushing. 28
We found no significant negative effects in people using tadalafil in our research. Different tadalafil adverse effects and patients who discontinued therapy owing to side symptoms have been described in the scientific literature. Seftel et al. 29 found that the overall rate of adverse effects recorded in individuals taking tadalafil 5 mg was 38.2%, with headache accounting for 8.8% and dyspepsia accounting for 4.7%. Back discomfort (1.9%), myalgia (2.2%), nasal congestion (2.8%), and limb pain (2.5%) were also significant adverse effects.
In the study by Buvat et al., 30 it was reported that the total rate of side effects in patients treated with 5 mg tadalafil was 31.1% and 1.9% of patients had left treatment due to side effects. In this study, the most common side effects observed were headache (4.5%), dyspepsia (3.5%), myalgia (3.1%), upper abdominal pain (3.1%), and back pain (1.9%). However, Bayraktar and Albayrak 27 showed that they used a combination of tadalafil and aspirin. In other words, in this study, aspirin use may have reduced side effects and prevented treatment abandonment. 27
Our study was implemented in several covid-19 peaks and our most important limitation was decreased number of participants due to the pandemic and the semi-elective nature of urethroplasty, which limited our study population. Although we observed improvements in some cases, there was no statistically significant difference between the two groups.
Conclusion
According to the findings of this study, continuous use of tadalafil in patients with mild-to-moderate ED after a 3-month treatment period may improve patients’ ED. In addition, despite a statistically significant increase in IIEF score in the tadalafil group versus the placebo group, the difference in IIEF score before and at 3 months between the groups was not statistically significant. Further research is required to examine the effects of daily use of tadalafil for longer periods of follow-up and larger populations so that the possibility of putting tadalafil into clinical practice can be assessed.
Footnotes
Authors’ contributions
Hamedreza Nourian Kafshgari: Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing. Danial Farhadi: Data collection, Data analysis, Manuscript writing. Sajjad Pourasghary: Manuscript writing and Data analysis. Morad Kohandel Gargari: Manuscript writing and Data analysis. Fateme Tahmasbi: Data collection, Manuscript editing/writing. Farzin Soleimanzadeh: Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing.
Ethic approval
This study was approved by the code (IR.TBZMED.REC.1399.829) in the ethics committee of Tabriz University of Medical Sciences and was registered with the code (IRCT20201111049350N1) in the Iranian clinical trial registration system.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.