
Abstract
Introduction:
This study aimed to evaluate the effect of coronavirus disease (COVID-19) on the patients’ referral in the pregnant population and also investigate each treatment approach’s advantages and disadvantages for acute renal colic in pregnancy.
Methods:
In this retrospective study, we included all pregnant women with ureteral stones referred to a referral center between January 2019 and March 2021.
Results:
Among 53 pregnant women, 18 (33.9%) were on conservative therapy, which passed the stone without any complications. Double J stent or nephrostomy tube insertion was done for 24 patients (45.2%). Seventeen of these patients (70.8%) presented post-surgical complications, including hematuria (29.2%), pyelonephritis (20.8%), and lower urinary tract symptoms (20.8%). Transurethral lithotripsy (TUL) was done in 11 patients (20.7%). Only one of these patients developed hematuria following TUL. Thus, in our population study, double J stent or nephrostomy insertion was associated with a higher chance of postoperative complications than TUL (p-value = 0.001). Thirty-six patients were referred within 13 months before the entry of COVID-19, while 17 were referred during a similar approximate duration after the COVID-19 entry into the country. Only the initial presentation had a significant difference between these two periods (p-value = 0.034).
Conclusions:
When conservative treatment fails, we recommend TUL as the second-line treatment over temporary procedures, such as double J stent or nephrostomy insertion. Of note, in a group of patients with an emergent clinical setting, including active infection, deteriorating renal function, signs of preterm labor, solitary kidney, etc., double J or nephrostomy tube insertion remains the preferred management method for its fast resolution of obstruction and infection. Besides, a decrease in visits with an increase in complicated cases after COVID-19 was observed, maybe due to a delay in referring.
Introduction
Symptomatic renal colic due to nephrolithiasis in pregnancy is a rare phenomenon that occurs once every 1500–3000 pregnancies.1,2 Although the probability of urolithiasis in pregnant women is the same as in non-pregnant ones, the pregnancy state makes the diagnosis and treatment more conflicting. 3 As pregnancy can mimic the signs and symptoms of renal colic, such as flank pain and microscopic hematuria, these signs and symptoms cannot be relied on, and imaging evaluation seems necessary. 4 While non-contrast computed tomography (CT) is the gold standard imaging tool for renal colic, ultrasonography is the preferred imaging modality for evaluating renal colic in pregnancy due to being non-invasive and free of ionizing radiation.5,6 Magnetic resonance imaging (MRI), with its high sensitivity and specificity, and low-dose CT, which is less preferable, are other options when ultrasonography is inconclusive.7,8
Treatment of acute renal colic in pregnant women requires special attention because it may result in preterm delivery, premature rupture of membranes, and pregnancy loss. 9 Conservative management using intravenous fluids and analgesics is the first-line treatment for pregnant women and can lead to spontaneous stone passage in up to 80% of patients. 10 Medical expulsive therapy using alpha-blockers and calcium channel blockers can also be used in these patients alongside antiemetics and narcotics if the first-line treatment fails. 11
In cases with pain refractory to analgesics, complete renal obstruction, worsening obstruction, solitary kidney, renal dysfunction, pre-eclampsia, persistent nausea and vomiting, stone size more than 1 cm, and sepsis, more aggressive treatment is indicated. 9 Surgical intervention to remove ureteral stones during pregnancy falls into two main groups: temporary and definite management. Temporary strategies are percutaneous nephrostomy drainage or ureteral stent insertion. They were preferred and considered the primary surgical approach during pregnancies based on their effectiveness and less invasiveness in the past decades. Thus, definitive surgical interventions, such as transurethral lithotripsy (TUL), were postponed until delivery. 12
The coronavirus disease (COVID-19) pandemic has affected urology practices as well as other medical aspects. A study by Maganty et al. 13 reported that the visits to one of their urology oncology clinics decreased by 38% during the COVID-19 period compared to the pre-COVID era. Besides, in another study by Steinberg et al., 14 38% and 44% visit reductions were seen during COVID-19 at their private and county hospitals, respectively, regarding kidney and ureteral stones.
COVID-19 infection and pregnancy are a hot-topic issue during this pandemic. The most common symptoms of the infection include cough, fever, myalgia, headache, and dyspnea, which are not different from the normal population, but one major point, which has been discussed in the literature, is the high susceptibility of pregnant patients to developing severe COVID-19 infection, especially in those with high body mass index (BMI), advanced age, pre-existing comorbidities, pre-eclampsia, and gestational diabetes.15,16 As COVID-19 infection is an anxiety-provoking experience in this vulnerable population, referral reduction may be more significant in urolithiasis during pregnancy. However, To the best of our knowledge, the impact of COVID-19 on urolithiasis during pregnancy has not been discussed in the literature.
Herein, we compared patients before and after the entry of COVID-19 into the country to evaluate the effect of COVID-19 on the referral of pregnant cases. Also, with each interventional approach having its benefits and complications, we designed and conducted this study to help surgeons decide the best option for managing acute renal colic during pregnancy due to ureteral stones.
Material and methods
This was a retrospective, cross-sectional study. The medical records of 53 pregnant women who were referred due to ureteral stone to the urology emergency room and outpatient clinic of our center from January 2019 to March 2021 were reviewed. All patients were included in this study. Patients with physiological hydronephrosis in pregnancy but without any stones have not entered the study. Ultrasonography was used as the diagnostic tool in all patients. The patients were managed either conservatively until stone passage or surgically. The patients who were managed surgically underwent TUL or double J stent or nephrostomy tube insertion. Management was multidisciplinary in our study population; a team consisting of a urologist, obstetrician, and anesthesiologist discussed the best management for every patient, and after a final consultation with patients, the best management for each patient was chosen.
Three types of management were used in our study population. (A) Conservative: conservative treatment was considered for patients with a lower pain scale and those who refused intervention due to concern about the potential effect of these procedures on the fetus. Antibiotics (third-generation cephalosporines) and analgesics (paracetamol, pethidine) were used for conservative treatment. (B) Temporary (double J or nephrostomy tube insertion): Patients with urinary tract infections (UTIs) due to increased risk of postoperative complication, 17 those who were in the first trimester of pregnancy- concerning the potentially hazardous effect of general anesthesia on the fetal outcome-, 18 as well as those who did not accept general anesthesia, underwent temporary management. (C) Definite (TUL): For the rest of the patients, TUL was done under general anesthesia (intubation); the type of anesthesia (e.g. general anesthesia for TUL) was chosen according to the consultation of the anesthesiologist with patients. We used zebra guidewire for ureteroscopy and stenting, and fluoroscopy was not used.
All data were collected by searching patients’ medical records. We filled out collection forms for all cases. Each form contained patients’ unit number, age, gestational age, chief complaint, stone size (based on ultrasonography), post-surgical complications, readmission to the hospital due to complications, and patients’ referral time based on the COVID-19 entry into the country. The date of the entry of COVID-19 was considered February 2020, as the first case in the country was confirmed in February 2020. 19 Also, admitted patients were screened for COVID-19 in the COVID-19 era. An 11-point (0–10, with 10 as the highest perceived pain) numeric pain rating scale (NPRS) score was used to assess the perceived pain.
Statistical analysis
IBM SPSS Statistics software version 26 was used for analysis. We used frequency, percent of frequency, and mean ± standard deviation (SD) for descriptive analysis and Pearson Chi-Square for bivariate analysis. Besides, Wilcoxon signed-rank tests, independent t-test, Mann-Whitney, or analysis of variance (ANOVA) were used for continuous variables as appropriate. The binary logistic regression model was applied to assess the independent association between type of surgical intervention and complication rate. The unadjusted odds ratio (OR) and its 95% confidence interval (CI) were estimated. A p-value < 0.05 was considered statistically significant.
Results
In our study, 53 pregnant women with ureteral stones were investigated. Thirty-six patients (67.9%) referred before the COVID-19 entry (February 2020), while others (32.1%) referred after that. Only three admitted patients had a history of COVID-19 after the COVID-19 entry; their tests were negative at the time of our screening. Also, we had a case of diabetes mellitus, whose blood sugar was controlled.
Among the patients, 18 (33.9%) with a mean age of 27.8 ± 6.6 years, a mean stone size of 6.0 ± 1.9 mm, and a mean gestational age of 17.2 ± 7.6 weeks could pass the stone with conservative management. These patients were referred with the only chief complaint of flank pain and had no complications following stone passing. Among the patients who could pass the stone, 13 (72.2%) were referred to our center before the COVID-19 entry, and five (27.8%) were referred after that. The average expected time to pass the stone was 4–6 weeks in this group.
Double J stent or nephrostomy insertion was done in 24 patients (45.2%) with a mean age of 29.4 ± 6.6 years, a mean stone size of 9.6 ± 2.3 mm, and a mean gestational age of 19.5 ± 7.9 weeks. These patients were referred due to flank pain (n = 17, 70.8%), pyelonephritis (n = 3, 12.5%), or both (n = 4, 16.7%). Seventeen (70.8%) of these patients had postoperative complications, including pyelonephritis (n = 5, 20.8%), lower urinary tract symptoms (n = 5, 20.8%), and hematuria (n = 7, 29.2%). Eight (47.1%) patients with postoperative complications were admitted to the hospital for complication management. The NPRS score for assessing pain was done in these patients before (mean = 7.2 ± 1.8) and after (mean = 2.9 ± 1.1) double J or nephrostomy insertion, which showed significant pain relief in these patients (p-value < 0.001). Among these patients, 15 (62.5%) were referred before the COVID-19 entry, while nine (37.5%) were referred after that. Besides, the mean NPRS score before double J or nephrostomy insertion was not significantly different before (mean = 7.6 ± 1.8) and after (mean = 6.7 ± 1.9) the COVID-19 entry (p-value = 0.305).
TUL was done in 11 patients (20.7%) with a mean age of 26.0 ± 5.5 years, a mean stone size of 8.0 ± 1.4 mm, and a mean gestational age of 17.8 ± 2.2 weeks. Urinary stones in all these patients presented with flank pain. The operation was done at a mean gestational age of 19.1 ± 1.6 weeks. Only three cases (27.3%) needed double J insertion, which was removed within the first week of operations. Only one of these patients (9.1%) developed hematuria after TUL, which was conservatively managed. Also, eight (72.7%) of these 11 patients were referred before the COVID-19 entry.
As demonstrated in Table 1, stone size, initial presentation, and complication rates differed significantly between the groups when dividing the patients based on the treatment approach. Stone size was considerably larger in the cases with temporary and definite management compared to the conservative therapy (p-value < 0.001). Also, the initial presentation in patients who underwent temporary treatment was pyelonephritis in seven patients (29.2%)—four accompanied with flank pain; this was expected because temporary management was indicated in cases with UTI. Also, when comparing definite treatment with temporary treatment concerning complications, the patients who underwent double J stent or nephrostomy insertion had a significantly higher rate of postoperative complications than those who underwent TUL (p-value = 0.001) (Figure 1). The regression model showed that double J stent or nephrostomy insertion increases the chance of postoperative complications compared to TUL (OR: 24.286, CI: 2.595–227.246, p-value = 0.005). This result was also approved when adjusted for the initial presentation (flank pain, pyelonephritis, or both) (OR: 46.667, CI: 4.215–516.613, p-value = 0.002).
Patients’ information classified by the type of treatment.
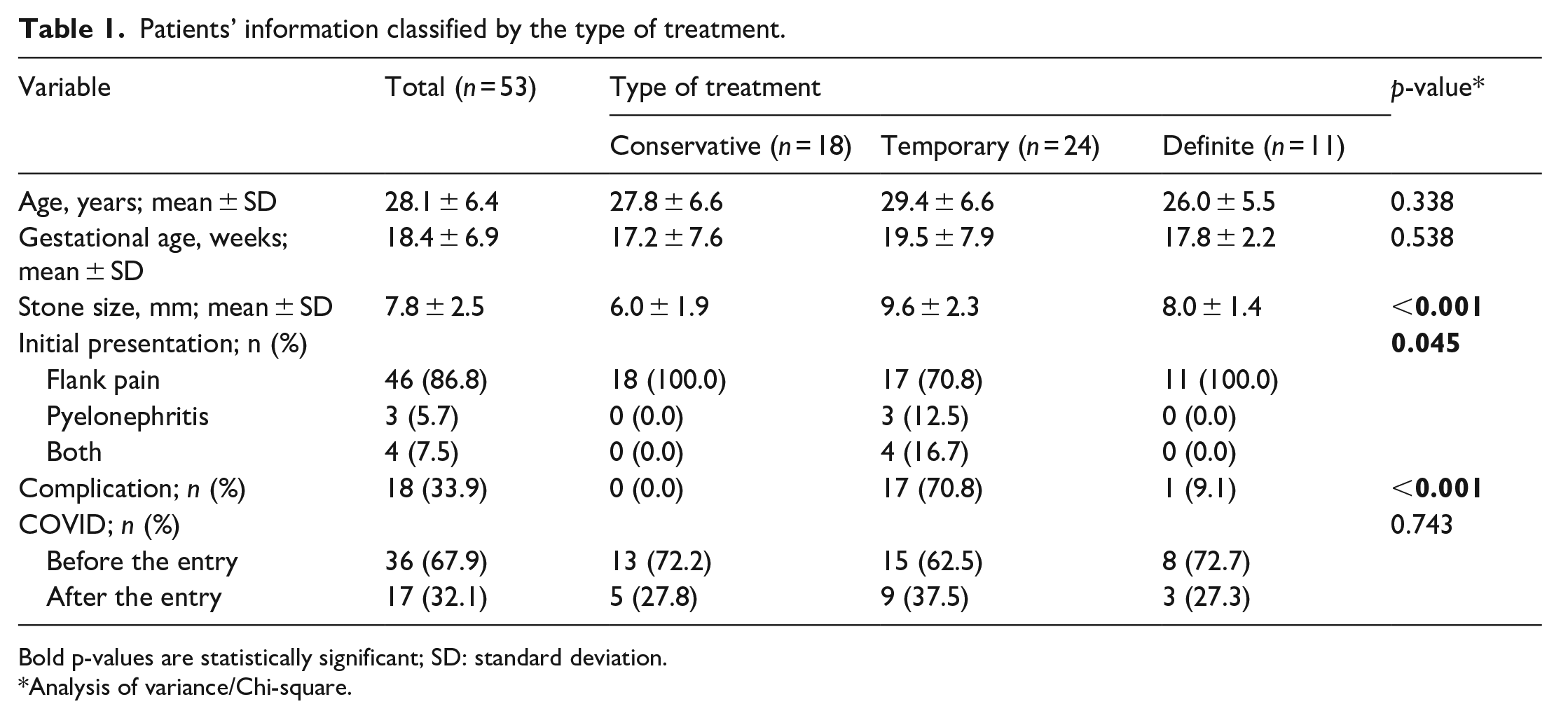
Bold p-values are statistically significant; SD: standard deviation.
Analysis of variance/Chi-square.
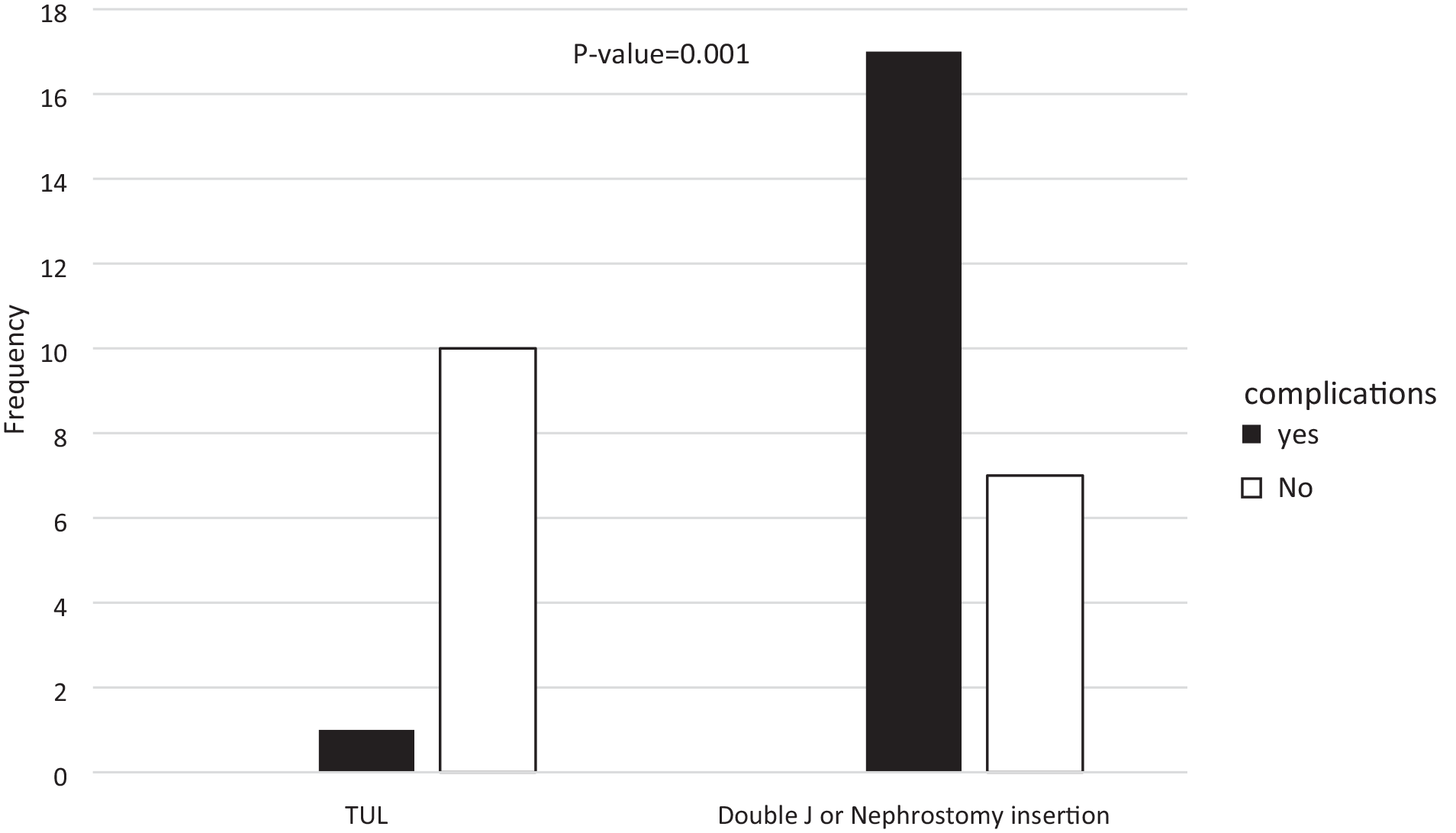
Complication rate of transurethral lithotripsy (TUL) versus double J or nephrostomy insertion.
Table 2 shows the patient’ information when classified by the time of referral based on the entry of COVID-19 into the country. Thirty-six patients were referred within 13 months before the entry of COVID-19, while 17 were referred during a similar approximate duration after the COVID-19 entry into the country (before: after COVID-19 = 2.12). Among the variables, only the initial presentation showed a statistically significant difference between before and after the COVID-19 entry into the country (p-value = 0.034). At the same time, age, gestational age, stone size, stone management, and complications were not significantly different (p-value > 0.05).
Patients’ information classified by the time of referral.
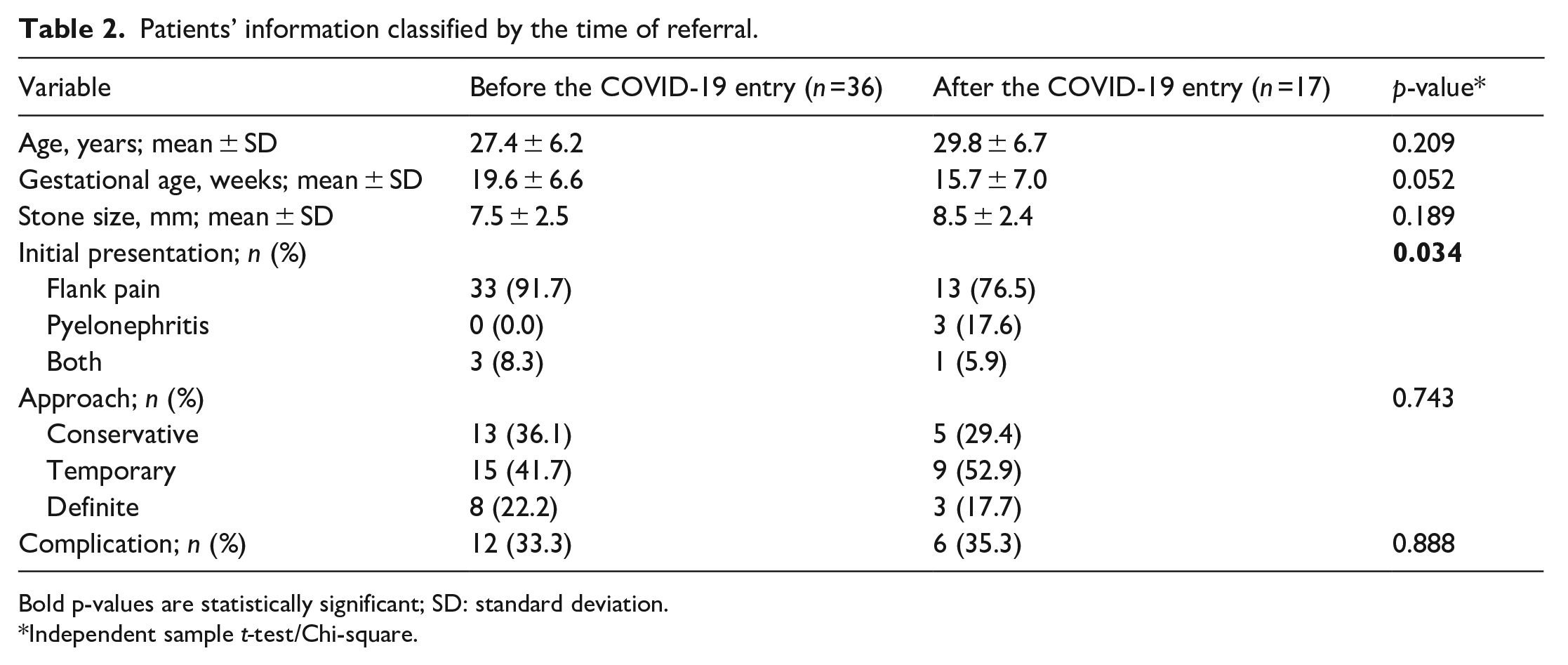
Bold p-values are statistically significant; SD: standard deviation.
Independent sample t-test/Chi-square.
Discussion
The management of ureteral stones during pregnancy includes conservative and interventional approaches; the interventional approach is divided into temporary and definite procedures. In this study, we assessed the optimal management concerning post-therapeutic complications. We observed complications in 70.8% of cases with a temporary approach compared to 9.1% in definite and 0.0% in conservative treatments. Also, as the 26 months of the study were divided into 2 periods of 13 months due to the COVID-19 entry into the country, the impact of COVID-19 on the referral of this population was evaluated. In the pre-COVID period, the visits were twice those in the post-COVID period. However, in comparing the patients’ characteristics between these two periods, only the initial presentation was significantly different, showing that more patients with pyelonephritis were referred after the COVID-19 entry.
Previous studies have shown decreased visits during the COVID-19 pandemic regarding urological diseases, including urolithiasis.13,14,20 This may be more significant in urolithiasis during pregnancy as it is an anxiety-provoking experience in this vulnerable population. In the study by Antonucci et al., 21 it was reported that a significant reduction (48.8%) was noted in patients admitted to the emergency department due to urolithiasis during the COVID-19 pandemic in Rome. More importantly, in their study, patients had more complications, and early stone removal was preferred over urinary drainage in the COVID-19 era. Our study period was 26 months, divided into two 13-month periods before and after the COVID-19 entry into the country. We observed that the number of patients before the COVID-19 entry was more than double that after the COVID-19 entry. This was probably the result of managing the stone-related pain at home instead of going to hospitals or clinics. 14 However, when comparing the patients’ information between those two periods, only the initial presentation was statistically different. Regarding initial presentation, four patients (23.5%) presented with pyelonephritis with/without flank pain after the COVID-19 entry compared to three patients (8.3%) before the COVID-19. This shows that more complicated cases went to hospitals after the COVID-19 entry due to delays in referring. Besides, we hypothesized that stone size might be larger after the COVID-19 entry for the same reason; although the mean stone size was 1 mm higher after COVID-19, this difference did not reach statistical significance. Also, contrary to our exceptions that more invasive approaches may be used post-COVID, the treatment approaches did not significantly differ after the COVID-19 entry. So, our findings showed a decrease in visits with an increase in complicated cases after COVID-19 in pregnant women with ureteral stones. However, the treatment approaches and, as a result, post-therapeutic complications did not differ.
As COVID-19 vaccination has led to changes in hospital management and patient referrals, it may have also altered the patients’ visits, their presentations, and management of urolithiasis. According to a literature review by Foschi et al., 22 COVID-19 vaccines were not associated with adverse urological outcomes, showing that no evidence has been reported against vaccination in patients with urological diseases. Unfortunately, we cannot assess the impact of COVID-19 vaccination in our setting because vaccination in our country began in February 2021 23 ; our study end date is March 2021. We surmise that with the increase of referrals after the vaccination, the referral of complicated cases has decreased. We suggest further studies to show the effect of vaccination on returning the number of patients’ referrals to the previous state.
Urinary stones mainly present with flank pain, abdominal pain, and hematuria during pregnancy. 24 In our study, the most prevalent signs and symptoms of urinary stones were flank pain and hematuria, which concurred with the previous findings.5,11 It is worth mentioning that due to non-specific flank pain, abdominal pain, and hematuria in the pregnancy state, it is often challenging to differentiate urolithiasis from physiologic changes25,26 or other differential diagnoses, including appendicitis, cholecystitis, pyelonephritis, abruption, and pre-eclampsia. 27
The general principle toward managing acute renal colic due to urinary stones is conservative till spontaneous stone passage. It is estimated that 48%–81% of pregnant patients with urinary stones may have a spontaneous stone passage.26,28 In this study, only about one-third (33.9%) of the pregnant women with acute renal colic had spontaneous stone passage. One reason for the lower proportion of spontaneous stone passage in our study may be that we perform interventional treatments early because, as a referral center, most of our patients are complicated and/or are referred from other centers after a failed conservative treatment. Besides, as a significant portion of our patients is referred from other cities, the possibility of follow-up loss is considered an influential factor in our management. As recommended by European Association of Urology guidelines, conservative management is an option when the stone size is <10 mm, 29 while most of the interventional treatments in our patients were done on patients with stones within this range.
If conservative management fails or the patient has sepsis, renal failure, solitary kidney, or bilateral obstructive uropathy, interventional treatment is required, irrespective of its potential risks. In temporary treatment, hydronephrosis caused by the obstructed stone is diverted by a double J stent or percutaneous nephrostomy, leading to the relief of the patients’ pain. In our study, after double J stent or nephrostomy tube insertion, the patients’ pain was relieved significantly from a mean of 7.27 to 2.91 (p-value < 0.001). This result was in line with the results of previous studies.30,31 In this case, the definitive management is postponed to after delivery. Although temporary treatment is an effective procedure in pregnancy, it has some drawbacks, including stent-induced bladder irritation, stent encrustation, stent or tube infection, the potential for tube obstruction by debris, tube dislodgement, bleeding, need to carry a collecting bag, and need for periodic changes.12,32 Besides, in our study, 70.8% of patients who underwent temporary management presented postoperative complications, including hematuria (29.2%), pyelonephritis (20.8%), and lower urinary tract symptoms (20.8%).
Due to the mentioned potential complications of temporary treatment options and significant improvements in flexible and rigid ureteroscopes, with their promising results, TUL is becoming the preferred definitive treatment option during pregnancy.33 –35 In the present study, only one (9.1%) among 11 patients who underwent TUL as the definite treatment presented with postoperative complication, hematuria. This makes definite therapy the suggested interventional approach over temporary management, with 70.8% complication incidence in our study. However, in a group of patients with an emergent clinical setting, including active infection, deteriorating renal function, sign of preterm labor, solitary kidney, etc., double J or nephrostomy tube insertion remains the preferred management method for its fast resolution of obstruction and infection. Regarding other interventional procedures, some studies have found percutaneous nephrolithotomy (PCNL) safe and promising.36,37 However, PCNL is not routinely recommended for definitive treatment of urolithiasis during pregnancy, mainly due to the need for prone positioning and prolonged fluoroscopy and anesthetic time. Of note, extracorporeal shock wave lithotripsy (ESWL) is contraindicated during pregnancy, especially early pregnancy.38,39
Limitations of the study
This study was not without limitations. Our sample size (53 cases) was small, and larger studies are suggested. Also, our study was a single-center study; multicentric studies are recommended for more reliable results. As a cross-sectional study, this study has its limitations, and future studies with a control group are suggested.
Conclusion
When conservative treatment fails to manage acute renal colic during pregnancy, regarding postoperative complications, we suggest TUL (definitive treatment) over double J stent/nephrostomy insertion (temporary management) as the second line of treatment. Of note, in a group of patients with an emergent clinical setting, including active infection, deteriorating renal function, signs of preterm labor, solitary kidney, etc., double J or nephrostomy tube insertion remains the preferred management method for its fast resolution of obstruction and infection. Besides, a decrease in visits with an increase in complicated cases after COVID-19 was observed, maybe due to a delay in referring. However, the treatment approaches and post-therapeutic compilations were not different before and after COVID-19.
Footnotes
Acknowledgements
None.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The Shiraz University of Medical Sciences Ethics committee reviewed and accepted the study protocol (ethical approval: IR.SUMS.REC.1397.886). The study protocol conforms to the provisions of the Declaration of Helsinki. Also, informed consent was provided from patients regarding participation in the study.